





Abstract
Background Asthma exacerbations in children is one of the most common medical conditions requiring urgent visits to primary healthcare providers or emergency departments, and even hospitalisations. Currently, there is significant variation in the management of asthma exacerbations expressed in guideline recommendations versus clinical practice. This disconnect affects diagnostic and treatment decisions for the clinician and patient.
Objective We systematically reviewed the available guidelines providing recommendations for diagnostic and therapeutic management of asthma exacerbations in the paediatric population.
Methods A systematic review of the literature for guidelines published between January 2009 and October 2019 was conducted, using a protocol registered with the international prospective register of systematic reviews (PROSPERO CRD42020221562).
Results 16 asthma exacerbation clinical practice guidelines for children were included. Despite general agreement between guidelines on the definition of asthma exacerbation, there was great variability in the definition of disease severity and assessment of asthma control. This systematic review also highlighted a paucity of recommendations for criteria for hospitalisation and discharge. Many guidelines scored poorly when measured for stakeholder involvement and editorial independence.
Conclusion Comprehensive and updated guidelines compliant with international standards for clinical guidelines may significantly improve clinical practice quality, promote evidence-based recommendations and provide uniformity of treatment between countries.
Abstract
There is wide variation in the management of asthma exacerbations in children. This systematic review suggests that updated guidelines aligned with international standards for clinical guidelines may improve uniformity of treatment and clinical practice quality. https://bit.ly/32Pgdiz
Introduction
Asthma is a chronic respiratory disease featured by inflammation causing bronchoconstriction, oedema and increased mucous production in the airways. It is the most common chronic disease of childhood, affecting 1–18% of the population in different countries [1]. Asthma is responsible for more than €20 billion per year in healthcare expenditures, driven primarily by asthma exacerbations and the need for emergency department (ED) visits, hospitalisations, school absences and loss of parental workdays [2].
Risk factors for childhood asthma span from genetic and perinatal risk factors to environmental triggers and host factors [1]. Wheezing is very common in the first years of life, but only a small proportion of infants and young children with wheezing progress to asthma in childhood and adolescence [3]. Several early-childhood wheezing phenotypes have been described based upon the presence or absence of atopy, the temporal patterns of symptoms, triggers of symptoms, disease severity, patterns of airway inflammation, and response to treatment [3]. However, the ability to identify young children at high risk of developing persistent asthma remains limited [4, 5].
Positive family history of asthma and atopy, genetic polymorphisms, epigenetic markers, respiratory tract infections early in life, allergic comorbidities (e.g., eczema, allergic rhinitis), active smoking in adolescence, and lung function deficits have all been identified as important determinants of persisting asthma symptoms from childhood through to adulthood [3, 6]. In comparison, for adult-onset asthma, the most common risk factors include female gender, allergic sensitisation and comorbidity, smoking, low socioeconomic status and poor adherence to medications, especially in the first years after diagnosis. In the adult population, asthma is a less quiescent disease than the childhood-onset disease, as there are more relapses and fewer remissions, and it generally exhibits a poor treatment response and worse prognosis [3, 6].
The shift from phenotype evaluation towards endotype analysis has recently allowed a better understanding of the clinical differences between childhood asthma and adult-onset asthma [7–9]. Considerable progress has been made in this area, with most asthma experts now classifying patients with asthma based on the amount of type 2 (T2) inflammation. While the T2-low asthma endotype, featured by either neutrophilic or paucigranulocytic airway inflammation sustained by interleukin (IL)-8, IL-17, IL-22 and other T-cell-related cytokines, is more common in adults, the T2-high asthma endotype, sustained by eosinophilic airway inflammation and allergic sensitisation, primarily driven by IgE and IL-4, IL-5 and IL-13, is more commonly detected in asthmatic children [10]. Improved knowledge of molecular pathways underlying asthma has enabled the characterisation of asthma phenotypes and the identification of novel biological therapies that have proven effective in treating severe asthma.
Still, despite advances in asthma management, asthma exacerbations in children remain a major issue. They can cause significant morbidity and mortality in patients. Real-life data from the Netherlands on the incidence of severe asthma exacerbations in children in primary care reported that four out of 1000 children with asthma would experience a severe exacerbation per follow-up year, and 25% of children with a severe asthma exacerbation will experience another one within 1 year [11, 12].
Many pharmacological interventions are currently available for asthma exacerbation treatment, but there is significant variation in the management of asthma exacerbations expressed in guideline recommendations versus clinical practice, affecting diagnostic and treatment decisions for the clinician and patient.
We aimed to systematically review the available guidelines, providing recommendations for the diagnostic and therapeutic management of asthma exacerbations in the paediatric population. We also sought to evaluate the recommendations stated in the included guidelines.
Methods
Literature review
This systematic review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) [13] and including guidelines published between January 2009 and October 2019. The protocol of our systematic review was registered and published with the international prospective register of systematic reviews (www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020221562; register number CRD42020221562).
Two reviewers (A. Licari and S. Manti) independently conducted searches of electronic medical literature databases, including PubMed, EMBASE and Global Health. The search strategy of each reviewer is detailed in Supplementary Appendix E1. Manual searches of grey literature and guideline-focused databases/repositories (Web of Science, Google Scholar, BMJ Best Practice, National Institute for Health and Care Excellence, and World Health Organization (WHO)) were conducted using variations on terms for “asthma”, “exacerbation”, “acute”, “children”, “child”, “adolescent” and “guidelines”. Also, selected references from the included guidelines were searched to identify any other relevant documents for inclusion.
Eligibility criteria
Inclusion criteria were: paediatric population; clinical practice guideline or guidance document with recommendations for the management of asthma exacerbations produced by global or national bodies; and the most up-to-date versions of guidelines (if multiple iterations were available). Exclusion criteria were: clinical trials, meta-analysis or systematic reviews not part of clinical practice guidelines; withdrawn or superseded guidelines; and guidelines focusing exclusively on asthma control or chronic asthma.
Guideline review
Data extraction was performed by the two independent reviewers (A. Licari and S. Manti), using standard templates to report recommendations in support of, or against, each specific area, and noting whether guidelines reported equivocal evidence.
Quality assessment
The AGREE II instrument, as described by Brouwers et al. [14], was used to assess the quality of guidelines in six domains: scope and purpose; stakeholder involvement; rigour of development; clarity of presentation; applicability; and editorial independence. Each domain contains 2–8 specific items. The quality of each item was scored by two independent reviewers using a 7-point scale. When differences of ≤2 were found between reviewers for a specific item, the average of the two scores was used as the final score for that item. When differences of ≥3 points were recorded for a specific item, the reviewers discussed the criterion and agreed on its final score. In accordance with AGREE II instructions, the overall quality of each domain was calculated as a percentage, as follows: (total actual domain score – minimum possible domain score)/(maximum possible domain score – minimum possible domain score)×100. No specific cut-off exists as a measure of high-quality guidelines [5], so a score above a threshold of 60% was adopted as a measure of high-quality guidelines. The instrument includes a guidance on how to rate the guidelines [14] (Supplementary Appendix E2).
Results
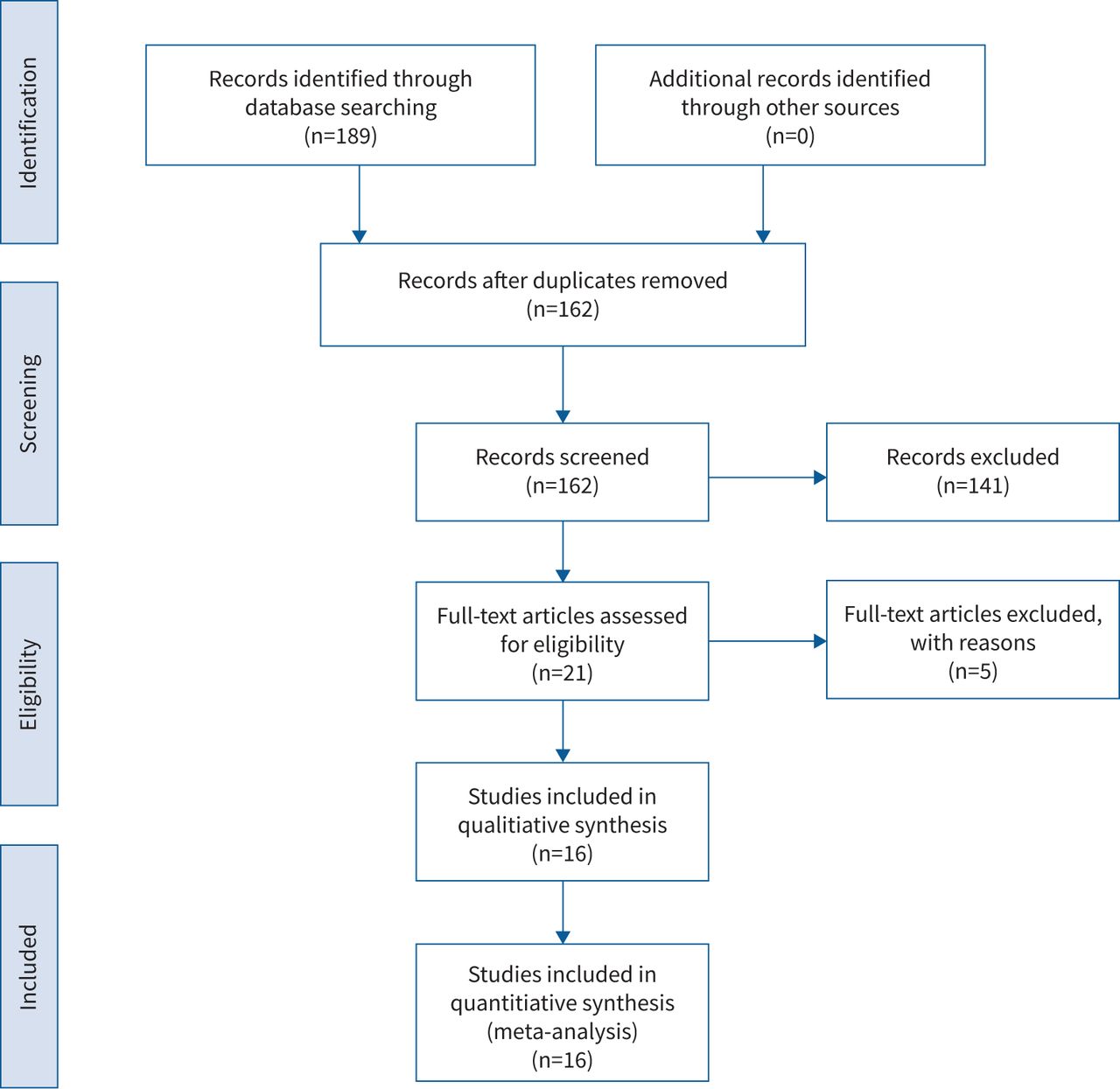
A total of 16 asthma exacerbations clinical practice guidelines were included in this review (figure 1) [1, 15–29].

{kind=link}
PRISMA flow diagram of the literature research.
Guideline characteristics
Table 1 details the characteristics of the 16 clinical practice guidelines included in this systematic analysis. Guidelines were published between 2009 and 2019, seven of which were from the WHO European region, one was from Canada, five from Asia, one from Oceania and one from the African region, according to WHO regional classifications.
Characteristics of guidelines included in the study
The characteristics of the clinical practice guidelines excluded from this systematic analysis [30–34] are given in table 2.
Characteristics of excluded guidelines
Quality assessment
Table 3 summarises the median score across guidelines for each domain of assessment. The guidelines provided good descriptions of their scope and purpose domains, but most (nine out of 16) did not score well for stakeholder involvement, which Brouwers et al. [14] refer to as reaching out to individuals from all the relevant professional groups, and seeking patients’ views and preferences. Seven out of 16 guidelines performed sufficiently in terms of editorial independence. As for rigour of development, six guidelines scored poorly, leading to little clinical applicability. Clarity of presentation scored well, with all guidelines scoring above the 60% threshold, and four reaching the 100% level. Overall, six of the guidelines were not recommended, four of them were recommended with modifications, and the remaining six were recommended without modifications.
Evaluation of guidelines: AGREE II Instrument scores for each domain
Definition of asthma exacerbations
Six guidelines did not specify a definition of asthma exacerbation, but there was a general agreement among the others regarding its definition, based on clinical and objective assessments. Most often, asthma exacerbation was defined as acute or subacute worsening of symptoms and lung function compared with the patient's normal status, and requiring a change in treatment or hospitalisation (table 4).
Definition of asthma exacerbation included in guidelines
Assessment of asthma control
Definition of asthma exacerbation severity
There was no unanimous definition of asthma exacerbation severity. In three of the guidelines, asthma exacerbation severity was not specified, and in four of them, classification of asthma exacerbation severity was not provided.
Five guidelines adopted the terms “mild”, “moderate” and “severe” to define asthma exacerbation, whereas another guideline defined those same terms, plus “very severe”. These terms, in addition to “near-fatal”, were adopted by one guideline. Nonsevere, severe and life-threatening asthma exacerbations were defined by one guideline, and another one adopted the terms “mild”, “moderate”, “severe” and “respiratory failure”.
The terms “mild”, “moderate”, “severe”, and “life-threatening” were used in two guidelines to define asthma exacerbations and, finally, “moderate”, “severe”, and “life-threating” terms were used by one guideline to define asthma exacerbations (Supplementary table E1).
Assessment of asthma control
Guidelines varied in their statements about specific recommendations for assessment of asthma control. Daytime and nocturnal symptoms, activity limitations and exacerbations were considered by seven guidelines as factors for evaluating asthma control. Eight guidelines evaluated the need for reliever medication and lung function assessment (peak expiratory flow (PEF) or forced expiratory volume in 1 s (FEV1)) as tools for assessing asthma control. Seven guidelines did not name mild and apparent symptoms as criteria for assessment of asthma control. Medication side-effects were considered helpful in assessing asthma control in four guidelines. As for the Latin American and Spanish guidelines, it was not possible to extract data focused exclusively on the paediatric population [28].
There was poor agreement between guidelines regarding the use of questionnaires/tests (Asthma Control Questionnaire (ACQ)/Asthma Control Test (ACT)), asthma diaries and other programmes and tools to assess asthma control. Absence from work or school due to asthma was considered a criterion for assessment of asthma control by one guideline (table 4). Finally, of the 16 guidelines, five did not provide any information on assessment of asthma control (table 5).
Risk factors for asthma exacerbations
Between the guidelines [1, 15–28], there was poor agreement about risk factors for asthma exacerbations. Allergen exposure and environmental tobacco were reported as risk factors for asthma exacerbations in 12 guidelines. In nine guidelines, air pollution was considered a risk factor. An array of other risk factors for asthma exacerbations included: diet, cold air, physical exercise, hospitalisation or ED visits for asthma in the last year, extreme inhaled bronchodilator use, poor inhaler technique, obesity and sputum or blood eosinophilia.
The protective effects of an influenza vaccination against asthma exacerbations were discussed in one guideline. Six of them agreed on comorbidities, and aspirin and other nonsteroidal anti-inflammatory drug use as risk factors for asthma exacerbations. Poor asthma control, underuse or poor adherence to treatment, and socioeconomic disadvantage were named as risk factors in four guidelines. 14 guidelines did not report extreme emotional upset, beta blocker use, requirement for long-term oral corticosteroid use, alternative therapies, hyoxaemia at initial management and psychological factors as risk factors for asthma exacerbations.
Intensive care admission or intubation and discontinued medical care were defined as risk factors in two guidelines.
Two guidelines did not cite any risk factors for asthma exacerbations (Supplementary table E2).
Assessment of asthma exacerbation
The Canadian guidelines and the International Consensus On (ICON) pediatric asthma did not provide any information on the assessment of asthma exacerbation. With the exception of the Indian and French guidelines, pulse rate, respiratory rate and degree of breathlessness, use of accessory muscles of respiration/dyspnoea, amount of wheezing, degree of agitation, level of consciousness and heart rate were mentioned in 12 guidelines as indicators of this condition. Among the instrumental/laboratory investigations, pulse oximetry was adopted by 11 guidelines, although the oxygen saturation cut-off point for detecting hypoxaemia varied from 90% to 92% between the guidelines. Only four guidelines also suggested arterial carbon dioxide tension determination. PEF monitoring to assess asthma exacerbations was suggested in nine guidelines.
Whether clinically indicated or in the presence of complications, seven guidelines suggested performing arterial blood gas measurements. One guideline supported the use of an electrocardiogram and/or echocardiogram and blood examination as laboratory and instrumental investigations to assess asthma exacerbations (Supplementary table E3).
Treatment of asthma exacerbations according to severity
β2 agonists
Inhaled salbutamol was consistently recommended for treatment of asthma exacerbations. Specifically, inhaled salbutamol was used for treatment of mild exacerbations by all guidelines. 12 guidelines also recommended inhaled salbutamol in moderate exacerbations, and nine of them supported the use of inhaled salbutamol in addition to oxygen supplementation for severe exacerbations. Five guidelines suggested intravenous salbutamol for severe asthma exacerbations.
The administration of inhaled terbutaline and formeterol was supported by two guidelines. Japanese guidelines supported the use of inhaled procaterol in mild asthma exacerbation. German guidelines supported the use both of i.v. terbutaline and i.v. reproterol in severe asthma exacerbations (Supplementary table E4).
Ipatropium bromide
The use of this medication was recommended for the treatment both of mild (two guidelines) and moderate (three guidelines), as well as severe exacerbations. In addition, 10 of the guidelines mentioned its use in conjunction with inhaled salbutamol and oxygen supplementation (Supplementary table E4).
Corticosteroids
Inhaled budesonide was indicated in one guideline; however, the severity of asthma exacerbations was not stated. Inhaled corticosteroids (ICSs) were not recommended in South African and Indian guidelines. In contrast, Swiss guidelines suggested ICSs use for both mild and moderate exacerbations.
The use of oral corticosteroids was suggested for the treatment of both mild (five guidelines) and moderate (11 guidelines), as well as severe exacerbations (four guidelines).
Seven guidelines suggested the use of i.v. corticosteroids when a severe exacerbation is occurring. Their use was also recommended for moderate exacerbations in two guidelines (Supplementary table E4).
Oxygen supplementation
With the exception of the Canadian and Turkish guidelines, oxygen supplementation was recommended in all guidelines for the treatment of mild (one guideline), moderate (six guidelines), and severe (15 guidelines) asthma exacerbation. There was no agreement in terms of oxygen saturation ranging from 92% to 95% (Supplementary table E4).
Disodium cromoglycate
There was no evidence of the use of inhaled disodium cromoglycate for the treatment of asthma exacerbation, except for a recommendation in the Japanese guidelines as a treatment for mild exacerbations (Supplementary table E4).
Alkaloids
For treatment of severe exacerbation, three of the 16 guidelines suggested the use of theophylline (Supplementary table E4).
Xantines
Five guidelines suggested the use of aminophylline for treatment of severe exacerbation, and one guideline suggested also using it for moderate exacerbation. Two guidelines discouraged the use of xantines entirely (Supplementary table E4).
Antibiotics
Three guidelines discouraged the use of antibiotics in asthma exacerbation treatment. One guideline suggested the use of antibiotics if complications were recurring (Supplementary table E4).
Leukotriene receptor antagonists
Leukotriene receptor antagonists were not mentioned in 14 of the 16 guidelines, and one guideline did not recommend their use for treatment of asthma exacerbation. Only one guideline suggested using them for mild asthma exacerbations (Supplementary table E4).
Magnesium sulfate
For severe asthma exacerbations, nine guidelines suggested the use of i.v. magnesium sulfate. Inhaled magnesium sulfate was proposed for treatment of mild and moderate exacerbations in one guideline (Supplementary table E4).
Helium
Three guidelines supported the use of helium in cases of severe asthma exacerbations, although it should be not routinely used (Supplementary table E4).
Noninvasive ventilation
Sufficient evidence is lacking to support noninvasive ventilation (NIV) use for exacerbation treatment (Supplementary table E4).
Drug dosages according to each of the included guidelines
Inhaled salbutamol given via metered-dose inhaler (MDI)-spacer was strongly recommended by all but two guidelines. However, there was no agreement regarding dosage, which ranged from two to 10 puffs (200–1000 μg), and timing administration, ranging from 20–30 min for the first hour. When salbutamol was given via nebuliser, the dosage most commonly reported was 2.5–5.0 mg up to three times every 20 min, over the first hour.
Wide variability in ipatropium bromide dosages were recorded. The recommended dosages ranged from four to eight puffs every 20 min, and then every 4–6 h as needed via MDI with spacer. Also recommended was a range from 0.25–5 mg every 20 min for three doses by the nebulised route, followed by every 4–6 h as needed via nebulisation.
Dosing recommendations for ICS administration have been not reported. In contrast, there was unanimous consensus on dosing for oral corticosteroids, i.v. magnesium sulfate and i.v. aminophylline dosage. In the guidelines included, i.v. methylprednisolone dosage was 1–2 mg·kg−1 8 h; dexamethasone dosage was 0.6 mg·kg−1 24 h; hydrocortisone dosage was 4–7 mg·kg−1 (to a maximum of 40 mg) per 24 h for 3–5 days; prednisolone dosage was 1–2 mg·kg−1 (to a maximum of 40 mg) per 24 h for 3–5 days; and prednisone dosage was 30–50 mg·day−1 for 7 days.
Regarding oxygen supplementation, targeted arterial oxygen saturation levels differed between guidelines, ranging from 92% to 95% (Supplementary table E5).
Hospitalisation criteria for asthma exacerbations
Most of the included guidelines (nine out of 16) did not report criteria for hospitalisation for asthma exacerbations. Of the guidelines that discussed the presence of poor respiratory effort, hypotension, bradycardia, agitation, accessory muscle use and tachypnea, only one suggested these clinical findings as indications for hospital admission. Silent chest, cyanosis, exhaustion, inability to complete sentences in one breath and/or too breathless to talk or eat, PEF value, moderately severe asthma not responding to β2-agonist therapy, complications and age were recommended as indications for hospital admission by the three guidelines that discussed these issues. Nocturnal asthma exacerbations indicated hospital admission in only one guideline.
Confusion or drowsiness; oxygen saturation; home circumstances, which do not allow safe or reliable treatment; severe exacerbations and respiratory failure; and moderate exacerbations with past history of severe exacerbations or not improved by ambulatory treatment for approximately 2 hours were mentioned in four guidelines as indicators for hospital admission.
Four guidelines suggested history of previous severe life-threatening asthma episodes as an indication for hospital admission (Supplementary table E6).
Discharge criteria for asthma exacerbation
Discharge criteria for asthma exacerbations were not mentioned in more than half of the included guidelines (nine out of 16). The other seven guidelines recommended the need for appropriate home care and for a written asthma action plan to be arranged. Of these seven guidelines, two suggested clinical stability, improved level of oxygen saturation and lung function, expressed in terms of FEV1 and PEF, as criteria for discharge. Of these two guidelines, one also adopted normal breath rate and the absence of chest wall indrawing as a guide for discharge (Supplementary table E7).
Discussion
We performed a systematic review of the available clinical guidelines providing recommendations on the diagnostic and therapeutic management of asthma exacerbations in the paediatric population.
Although there was general agreement between guidelines regarding the definition of asthma exacerbation and its risk factors and their assessment, we found great variability in the definition of disease severity and assessment of asthma control. Specifically, across the guidelines, “severe asthma”, “acute asthma”, “near-fatal asthma” and “life-threating asthma” sometimes seemed to have the same meaning, yet these terms differ from one another. “Severe asthma” refers to a degree of severity; “acute asthma” expresses a time window; “near-fatal” indicates that the exacerbation is due to severe asphyxia caused by hypoxaemia and hypercapnia; and “life-threating asthma” describes an asthma exacerbation due to hypoxaemia [35]. Thus, it does not seem possible to extract a unique definition of asthma exacerbation severity. As a result, we hypothesised that this wide variability could be due to the difficulty in staging the disease, hampered by a lack of validated diagnostic tools with minimum acceptable cut-offs. Accordingly, the comparisons between guidelines highlighted the variation in the diagnosis of asthma exacerbation. The choice for the best diagnostic management is still under debate and, although the PEF/FEV1 measurements are more reliable indicators of the severity of asthma exacerbations [1], the frequency and severity of clinical symptoms are more commonly adopted in clinical practice, even if they change substantially and are not uniformly adopted by experts.
Given the numerous classifications for disease severity proposed by the included guidelines, several therapeutic approaches were suggested. For example, even if the administration of ß-2 agonists and inhaled and systemic corticosteroids were recommended by all guidelines, the medication timing and dosage differed, leading to conflicting practices and interventions. Also, there was little discussion and wide variability of second-line treatment recommendations, namely i.v. β2-agonists, i.v. theophylline, i.v. aminophylline, inhaled or i.v. magnesium sulfate, helium and NIV.
The achievement of asthma control can be viewed as the result of the complex interaction between objective factors, such as the disease, airway status, and disease-related factors (comorbidities), and subjective factors, such as the patient's reporting of symptoms, use of medications and other variables [36–38]. Moreover, as discussed, several discrepancies have occurred between guidelines recommendations, clinical practice, and the questionnaires’ rating of asthma control [36–38]. Consequently, it is hardly surprising to find little consensus between guidelines regarding the assessment of asthma control.
This systematic review also highlighted a shortage of recommendations for criteria for hospitalisation and discharge. This lack of recommendations leads to underestimating the severity of disease, which increases both the risk of treatment failure and complications. A better approach would be to have standardised discharge criteria designed to guarantee improved stratification of hospitalised patients. Specifically, this would enable distinguishing between patients who can safely be discharged from the hospital because they are familiar with their clinical condition and can self-manage worsening symptoms and rescue medications, versus patients who need to remain hospitalised for further diagnostic evaluation or treatment.
The current lack of uniform guidelines is unacceptable, as asthma exacerbations should be considered a failure of the current diagnostic and therapeutic management. Meaningful change requires an urgent revision to guidelines, and follow-up for physicians, parents and patients. As part of this effort, the availability of recommendations for criteria for hospitalisation and discharge could result in improved clinical outcomes and more efficient use of hospital resources.
This systematic review includes guidelines published from the year 2009 onwards, so it is reasonable to hypothesise that older guidelines might be based on outdated evidence, affecting the final analysis. Moreover, the disagreement between guidelines reflects the low quality of the applicability domain as highlighted in the AGREE II instrument. Furthermore, many guidelines scored poorly in the stakeholder involvement and editorial independence domains.
Stakeholder involvement refers to a two-way communication channel that begins with clinical research, and through the interaction of a multidisciplinary team involved in decision-making processes, achieves the desired outcomes, solves critical health issues and provides significant results to research subjects and patients. Given the importance of this process, poor stakeholder involvement can contribute to the lack of guideline applicability. Additionally, as it can be quite difficult to insulate editorial decisions from bias, such as personal and/or economic interests, processes minimising the risk of editorial decisions influenced by external factors should be applied.
There were several limitations to our systematic review. First, it was impossible to identify specific clinical characteristics (e.g. atopic predisposition and sensitisation, age, asthma endotype, severity of asthma, comorbidities) and setting characteristics (e.g. home, ED, paediatric unit, paediatric intensive care unit) that physicians would consider when designing diagnostic and therapeutic management for the patient. Also, despite all of the analysis of guidelines included in this systematic review, it became impossible to include safety data, comparisons between different devices for drug administration, and clinical outcomes following first- and second-line treatments. We strongly suggest that a systematic review of randomised clinical trials could represent one of the most important research opportunities for exploring these issues.
Conclusion
The guidelines included in our systematic review showed significant variability in recommendations for the diagnostic and therapeutic management of asthma exacerbations in the paediatric population. Variable recommendations between guidelines may reflect the difference in health care systems, health education, broad economic, social and political issues, as well as changes in the evidence base for asthma exacerbation management. We strongly believe that comprehensive and updated guidelines compliant with international standards for clinical guidelines may significantly improve clinical practice quality, promote evidence-based recommendations and provide uniformity and appropriateness of treatment between countries.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Appendixes ERR-0367-2020_Appendixes
Footnotes
Provenance: Submitted article, peer reviewed.
This article has supplementary material available from err.ersjournals.com
Conflict of interest: S. Manti has nothing to disclose.
Conflict of interest: A. Licari has nothing to disclose.
Conflict of interest: S. Leonardi has nothing to disclose.
Conflict of interest: G.L. Marseglia has nothing to disclose.
- Received November 19, 2020.
- Accepted April 20, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










