





Figures
- FIGURE 1
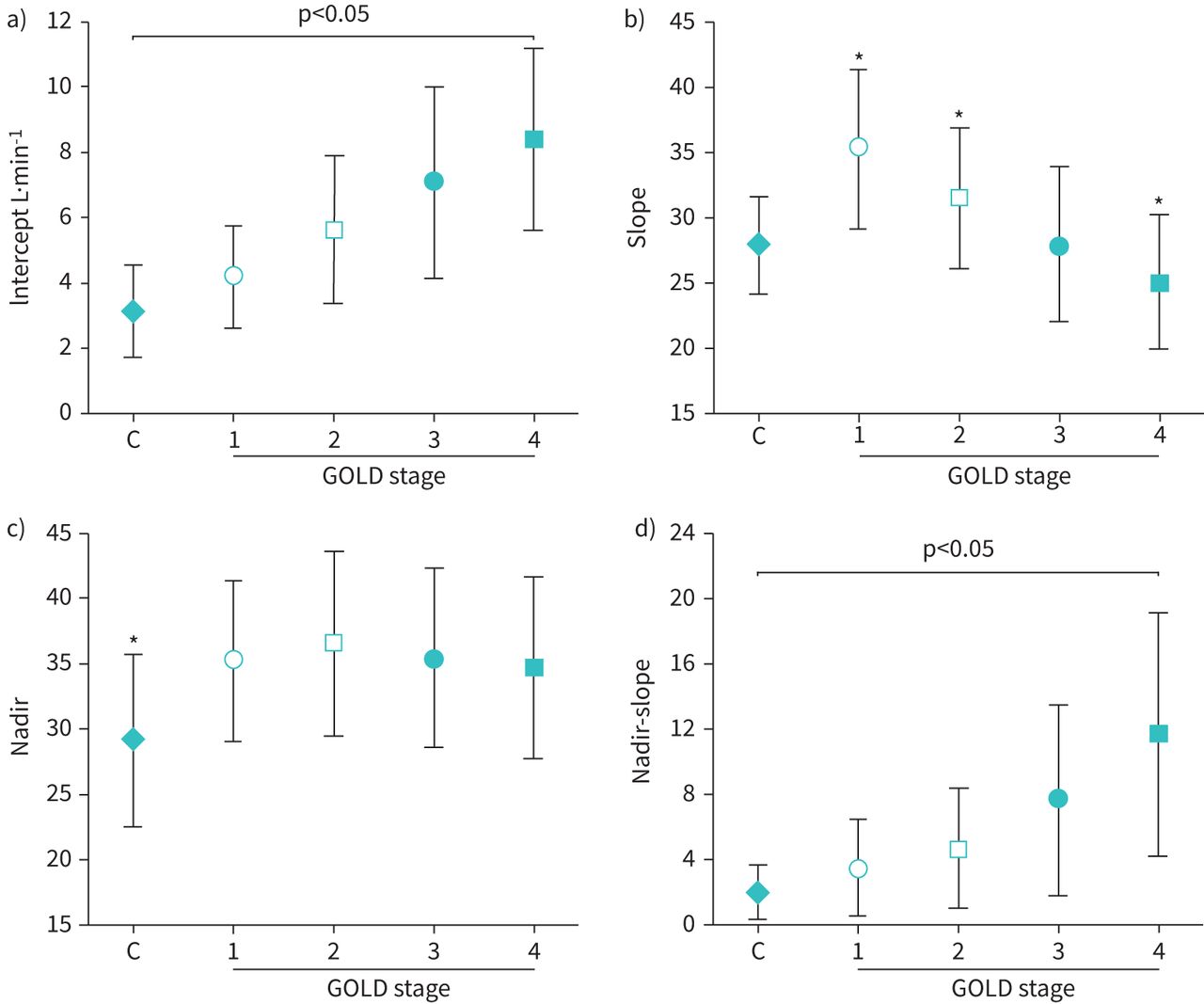
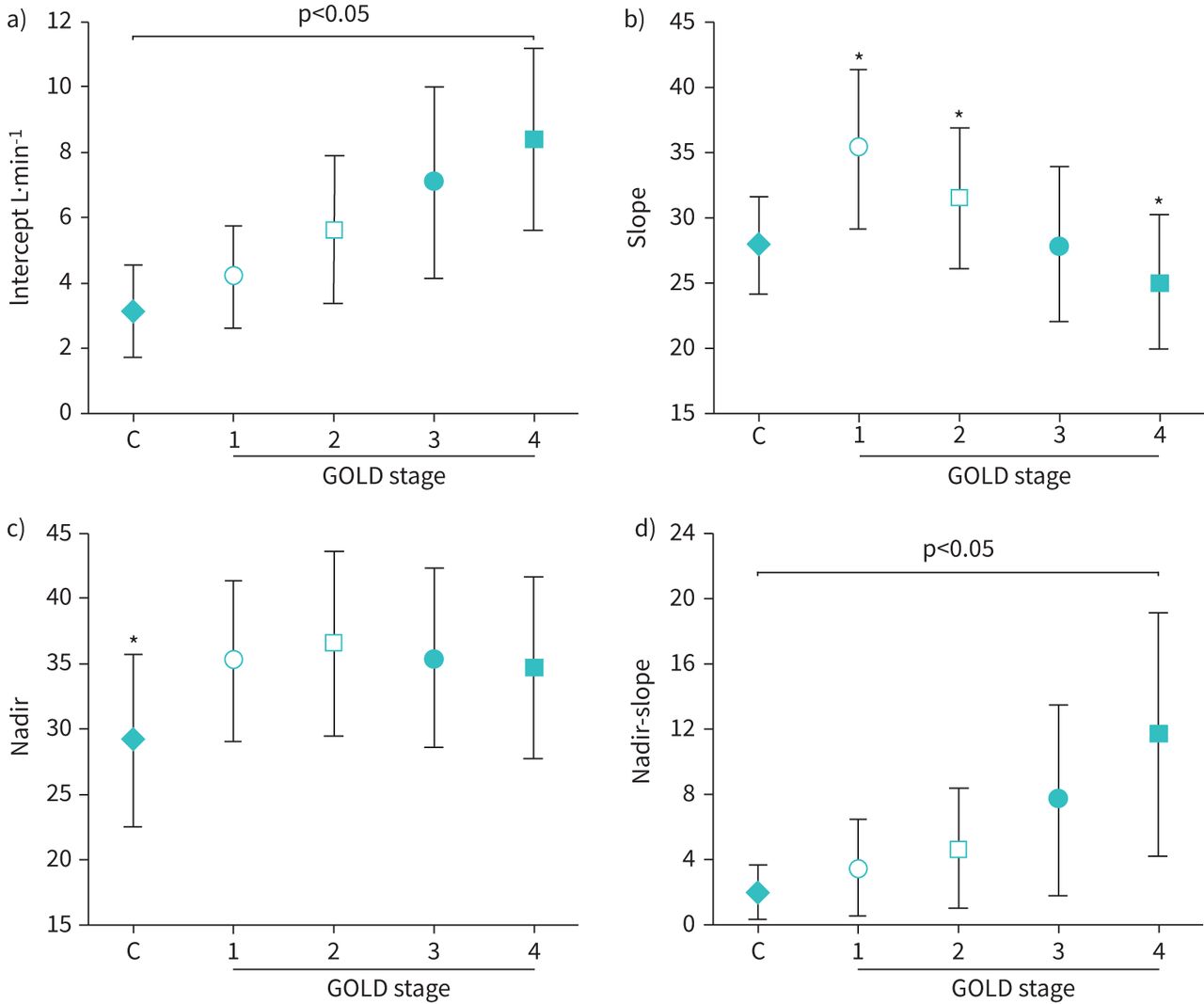
Effects of COPD severity on different parameters of the minute ventilation (V′E)/carbon dioxide output (V′CO2) relationship. a) V′E/V′CO2 intercept increased and b) V′E/V′CO2 slope diminished as the disease progressed from Global Lung Initiative for Chronic Obstructive Lung Disease (GOLD) spirometric stages 1 to 4. c) As the V′E/V′CO2 nadir depends on both slope and intercept, it remained elevated (compared to controls (C)) across disease stages. d) Increasing nadir-slope differences from GOLD stages 1 to 4 reflects the impact of a progressively higher intercept. Data are presented as mean±sd. *: p<0.05 different from controls. Reproduced with permission [39].
- FIGURE 2
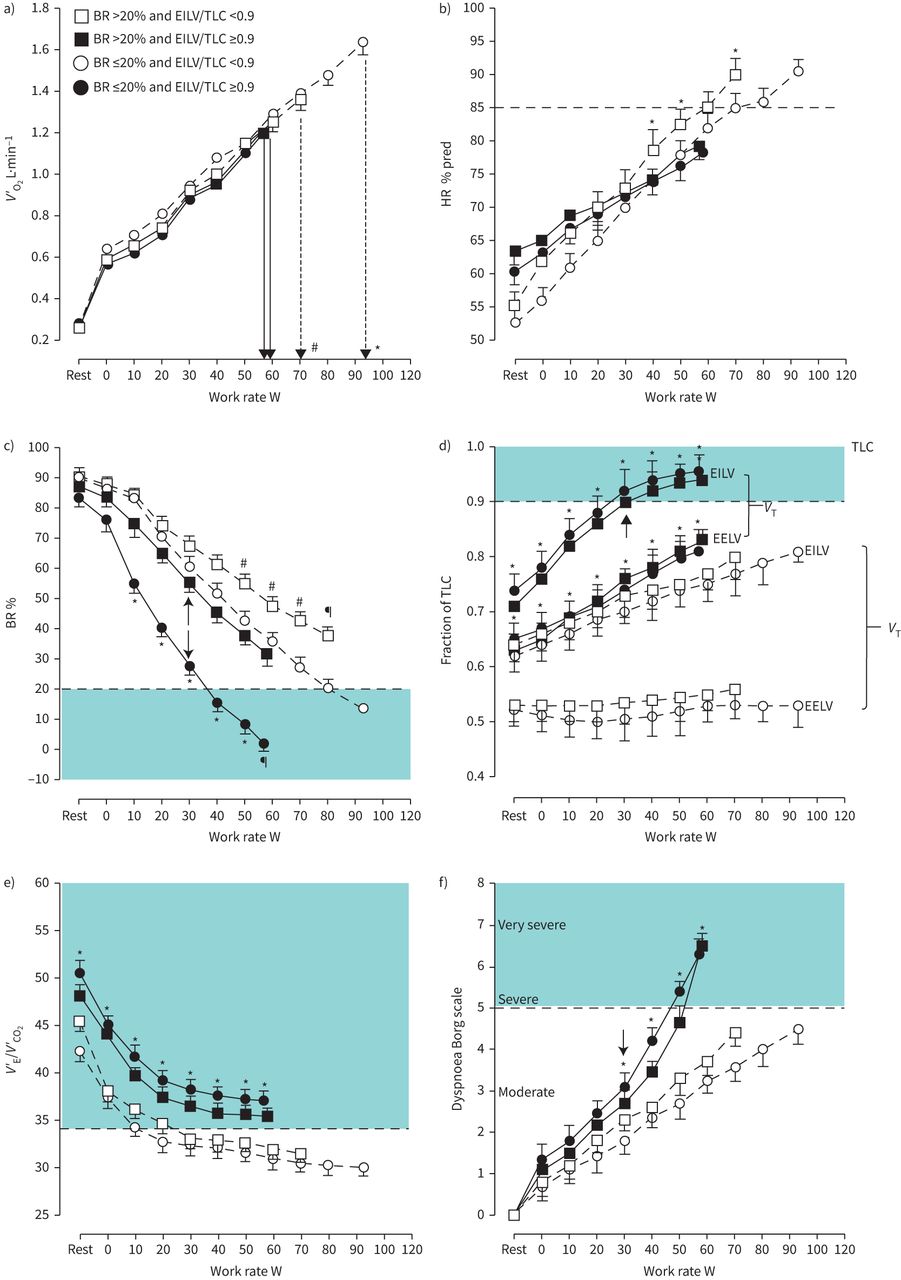
a) Metabolic, b) cardiovascular, c–e) ventilatory and f) sensory responses to symptom-limited incremental cardiopulmonary exercise testing in COPD patients presenting or not with a low breathing reserve ((BR) ≤20% or >20%, respectively) and/or high inspiratory constraints (end-inspiratory lung volume (EILV)/total lung capacity (TLC) ≥0.9 or <0.9, respectively). Commonly used ranges for severe physiological and sensory impairment are highlighted (shaded areas in panels c–f). The arrows in panels c), d) and f) emphasise the exercise intensity associated with a disproportionate increase in dyspnoea relative to metabolic and ventilatory demand. Note that patients who were particularly limited due to f) exertional dyspnoea (closed symbols) presented with d) high inspiratory constraints and e) high ventilation (V′E)/carbon dioxide output (V′CO2) ratio, regardless of c) the breathing reserve. *: p<0.05 versus the other groups; #: p<0.05 versus the remaining groups; ¶: p<0.05 versus BR ≤20% or EILV/TLC <0.9 and BR >20% or EILV/TLC ≥0.9. Data are presented as mean±sem. V′O2: oxygen uptake; HR: heart rate; EELV: end-expiratory lung volume; VT: tidal volume. Reproduced from [44] with permission.
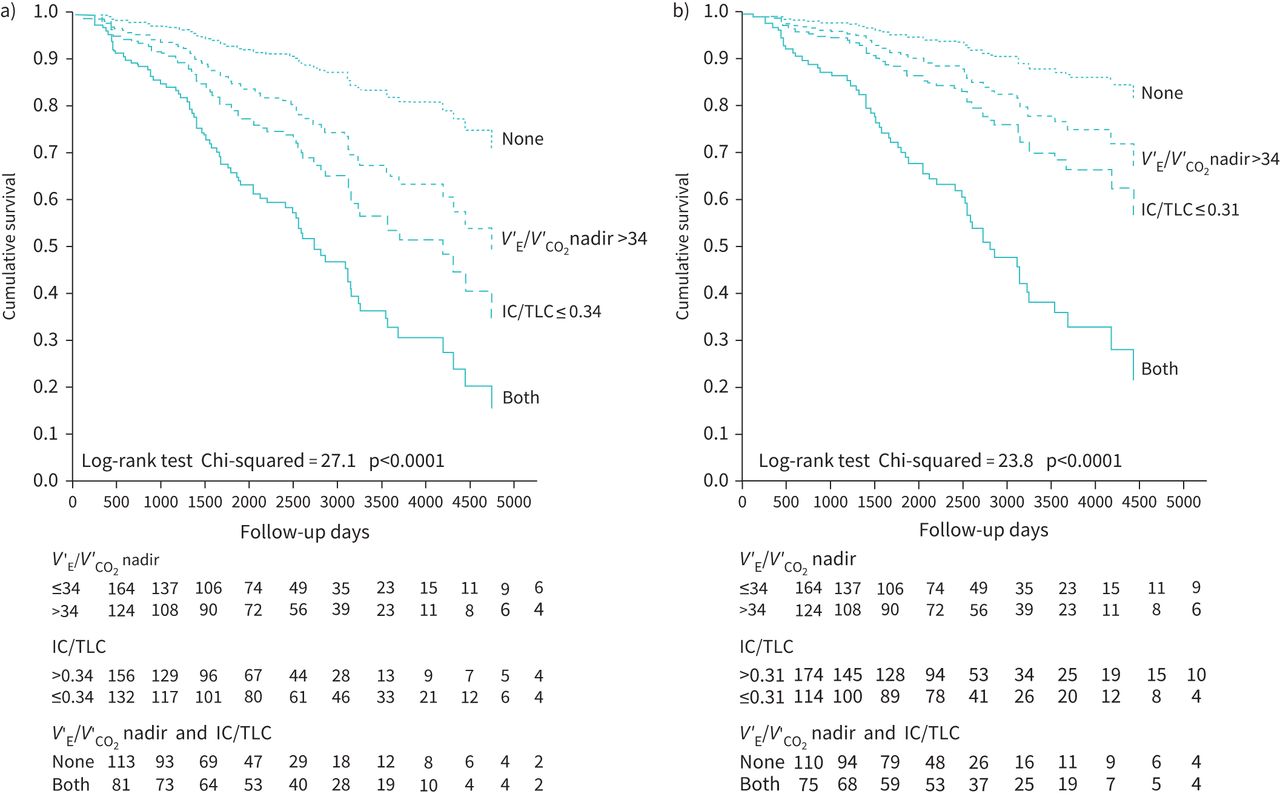
- FIGURE 3
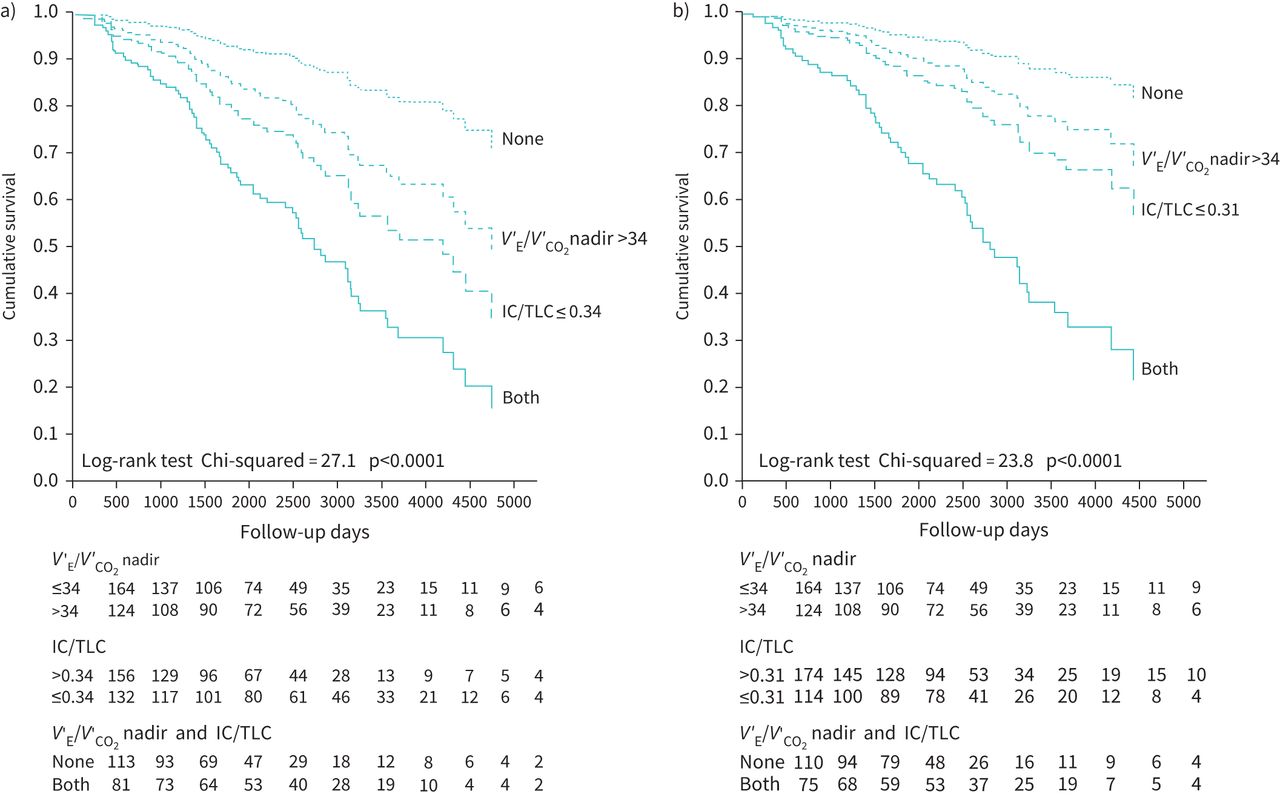
Value of high ventilation (V′E)/carbon dioxide output (V′CO2) nadir in isolation and associated with resting lung hyperinflation (low inspiratory capacity (IC)/total lung capacity (TLC) ratio) to predict a) all-cause and b) respiratory mortality in patients with mild to severe COPD. Reproduced from [67] with permission.
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Overview of cardiopulmonary exercise testing-based studies on the minute ventilation (V′E)/carbon dioxide output (V′CO2) relationship in different clinical scenarios in COPD
Subjects n Disease severity Main result Structural and functional determinants O’Donnell (2002) [15] 20 FEV1 34±3% ⇓ V′E at a given V′CO2 in CO2 retainers compared to non-retainers Nakamoto (2007) [16] 10 FEV1 27–70% V′E–V′CO2 slope not related to increased muscle ergoreflex activity Paoletti (2011) [17] 16 FEV1 54±18% ⇓ V′E–V′CO2 slope in more extensive emphysema Chin (2013) [18] 40 FEV1 87±11% ⇑ V′E/V′CO2with added external dead space in mild COPD Neder (2015) [19] 276 GOLD 1–4 ⇑ V′E–V′CO2 slope associated with ventilation inhomogeneity in GOLD 1 and 2 Elbehairy (2015) [20] 22 FEV1 94±10% ⇑ V′E/V′CO2 associated with greater VD/VTphys in symptomatic GOLD 1 Crisafulli (2016) [21] 51 FEV1 55±16% ⇑ V′E–V′CO2 slope associated with emphysema extension on chest CT Elbehairy (2017) [22] 62 FEV1 65±8% ⇑ V′E/V′CO2 associated with ⇓ TLCO and ⇓ V′O2 peak in smokers with mild obstruction Jones (2017) [23] 19 FEV1 82±13% ⇑ V′E/V′CO2 linked ⇑ emphysema and ⇓ TLCO to exercise intolerance in mild COPD Behnia (2017) [24] 32 FEV1 56±16% ⇑ V′E/V′CO2 inversely related to exercise TLCO Smith (2018) [25] 67 GOLD 1–4 ⇑ V′E/V′CO2 positively related to emphysema extent Tedjasaputra (2018) [26] 17 FEV1 94±11% V′E/V′CO2 nadir ≥34 associated with ⇓ pulmonary capillary blood volume and ⇑ dyspnoea Elbehairy (2019) [27] 300 FEV1 61±25% ⇑ V′E/V′CO2 nadir in tandem with progressively ⇓ TLCO across FEV1 and IC tertiles Rinaldo (2020) [28] 50 FEV1 56±16% ⇑ V′E/V′CO2 nadir in patients with an emphysematous phenotype Influence on physiological and sensory responses to exercise Palange (2000) [29] 9 FEV1 <50% ⇑ V′E–V′CO2 slope in walking than cycling Ofir (2008) [30] 42 FEV1 91±8% ⇑ V′E/V′CO2 nadir in smokers with chronic dyspnoea Ora (2009) [31] 36 FEV1 49±10% ⇓ V′E/V′CO2 nadir in obese patients with COPD Guenette (2011) [32] 64 FEV1 86±11% No sex effect on V′E/V′CO2 nadir Caviedes (2012) [33] 35 FEV1 59±22% ⇑ V′E/V′CO2 nadir associated with lower maximal exercise capacity Teopompi (2014) [34] 56 FEV1 26–80% ⇑ V′E–V′CO2 intercept related to greater dynamic hyperinflation
⇑ V′E–V′CO2 slope associated with lower maximal exercise capacityGuenette (2014) [35] 32 FEV1 93±9% ⇑ V′E/V′CO2 throughout incremental exercise in mild COPD Ciavaglia (2014) [36] 12 FEV1 60±13% No effect of exercise modality on V′E/V′CO2 in obese patients with COPD Barron (2014) [9] 24 FEV1 60±13% V′E/V′CO2 nadir showed excellent test–retest reliability (superior to V′E–V′CO2 slope)
V′E/V′CO2 nadir showed better test–retest reliability in COPD than HFO’Donnell (2014) [37] 208 GOLD 1 and 2 ⇑ V′E/V′CO2 throughout incremental treadmill tests in GOLD 1 and 2 Elbehairy (2015) [38] 20 FEV1 91±10% ⇑ V′E/V′CO2 nadir in GOLD grade 1B Neder (2015) [39] 316 GOLD 1–4 ⇑ V′E–V′CO2 intercept from GOLD 1 to 4 associated with exertional dyspnoea
⇑ V′E–V′CO2 slope in GOLD 1 and 2, but lower slopes in GOLD 3 and 4Faisal (2016) [40] 48 FEV1 63±22% ⇑ V′E/V′CO2 in COPD and ILD presenting with similar resting inspiratory capacity Elbehairy (2016) [41] 20 FEV1 101±13% Similar V′E–V′CO2 in smokers without COPD and healthy controls Crisafulli (2018) [42] 254 FEV1 51±14% V′E–V′CO2 slope >32 and inspiratory constraints associated with impaired HR recovery Bravo (2018) [43] 16 FEV1 42±9% ⇑ V′E/V′CO2 accelerates mechanical constraints and dyspnoea during interval exercise Neder (2019) [44] 288 GOLD 1–4 Ventilatory inefficiency and inspiratory constraints best predicted dyspnoea severity Kuint (2019) [45] 20 FEV1 63±21% Worsening gas trapping associated with lower ΔV′E/V′CO2 peak-nadir Neder (2020) [46] 284 GOLD 1–4 Resting V′E/V′CO2 predicts V′E/V′CO2 nadir and exertional dyspnoea Neder (2020) [5] NA NA Regardless of ventilatory capacity, major ⇓ in modelled WR peak as V′E/V′CO2 ⇑ Influence of comorbidities Holverda (2008) [47] 25 NA ⇑ V′E/V′CO2 nadir associated with mean pulmonary artery pressure Vonbank (2008) [48] 42 FEV1 1.1±0.5 L ⇑ V′E/V′CO2 rest and peak in patients with associated PAH Boerrigter (2012) [49] 47 FEV1 55±17% Pronounced ⇑ V′E–V′CO2 slope in a sub-group (n=9) with severe PAH Thirapatarapong (2013) [50] 48 FEV1 31±10% No effect of β-blockers on V′E/V′CO2 nadir in a retrospective study Thirapatarapong (2014) [51] 98 FEV1 20±7% No association of V′E/V′CO2 peak with PAH in severe to very severe COPD Teopompi (2014) [52] 46 FEV1 52±16% ⇓ V′E–V′CO2 slope in COPD compared to HF in patients with poorer exercise capacity
⇑ V′E–V′CO2 intercept in COPD compared to HFThirapatarapong (2014) [53] 108 FEV1 26±14% ⇑ V′E/V′CO2 nadir in COPD patients with coexistent coronary artery disease Apostolo (2015) [54] 95 FEV1 53±13% ⇑ V′E–V′CO2 intercept in COPD and COPD-HF compared to HF Arbex (2016) [55] 98 FEV1 55±17% ⇑ V′E–V′CO2 slope and V′E/V′CO2 nadir in COPD-HF compared to COPD
⇓ V′E–V′CO2 intercept in COPD-HF compared to COPDRocha (2016) [56] 68 FEV1 60±18% ⇑ V′E–V′CO2 slope in COPD-HF with exercise oscillatory ventilation Rocha (2017) [57] 22 FEV1 60±11% ⇑ V′E/V′CO2 more associated with hyperventilation than ⇑ VD/VTphys in COPD-HF Muller (2018) [58] 40 FEV1 43±13% V′E/V′CO2 not related to diastolic dysfunction Cherneva (2019) [59] 104 FEV1 1.4±0.4 L ⇑ V′E–V′CO2 slope associated with stress-induced diastolic dysfunction Smith (2019) [60] 22 FEV1 60±11% ⇑ V′E–V′CO2 intercept in COPD compared to HF with preserved and low ejection fraction Goulart (2020) [61] 10 FEV1 1.6±0.1 L ⇑ V′E–V′CO2 slope associated with disease severity in COPD-HF Costa (2020) [62] 42 FEV1 52±14% ⇑ V′E/V′CO2 was a key correlate of dyspnoea and exercise intolerance in CPFE Plachi (2020) [63] 28 NA Mechanical constraints modulate dyspnoea-V′E differently in COPD and HF Risk assessment/prognosis Torchio (2010) [64] 145 FEV1 73±16% ⇑ V′E–V′CO2 slope predicted mortality after lung resection surgery Brunelli (2012) [65] 70 FEV1 81±18% V′E–V′CO2 slope >35 predicted poor outcome after lung resection surgery Shafiek (2016) [66] 55 FEV1 60±17% V′E–V′CO2 slope >35 predicted poor outcome after lung resection surgery Neder (2016) [67] 288 FEV1 18–148% V′E/V′CO2 nadir >34 added to resting hyperinflation to predict mortality Alencar (2016) [68] 30 FEV1 57±17% V′E/V′CO2 nadir >34 and right ventricular function predicted mortality in COPD-HF Torchio (2017) [69] 263 GOLD 1–4 ⇑ V′E–V′CO2 slope was the best predictor of death after pneumonectomy Miyazaki (2018) [70] 974 FEV1 78±23% V′E–V′CO2 slope predicted 90-day and 2-year survival after lung resection for cancer Ellenberger (2018) [71] 151 FEV1 82±21% V′E/V′CO2 nadir >40 predicted 4-year survival after lung resection for cancer Crisafulli (2018) [42] 254 FEV1 51±14% ⇑ V′E–V′CO2 slope associated with a delay in post-exercise heart rate Effects of interventions Orens (1995) [72] 5 FEV1 57±4% Single lung Tx decreased V′E/V′CO2 peak Somfay (2001) [73] 10 FEV1 31±10% Decrements in V′E with hyperoxia correlated with decreases in V′CO2 O’Donnell (2001) [74] 11 FEV1 31±3% Proportional decrements V′E and V′CO2 with hyperoxia in advanced COPD O’Donnell (2004) [75] 23 FEV1 42±3% Salmeterol proportionally increased V′E and V′CO2 during constant work rate exercise Palange (2004) [76] 12 FEV1 <50% pred Heliox increased V′E/V′CO2 during constant work rate exercise O’Donnell (2004) [77] 187 FEV1 44±13% ⇑ V′E (due to higher VT) at a given V′CO2 with tiotropium compared to placebo Porszasz (2005) [78] 24 FEV1 36±8% Exercise training proportionally reduced V′E and V′CO2 during constant exercise Bobbio (2005) [79] 11 FEV1 53±20% Lobectomy increased V′E–V′CO2 slope Eves (2006) [80] 10 FEV1 47±17% Normoxic heliox increased V′E/V′CO2 more than hyperoxic heliox Chiappa (2009) [81] 12 FEV1 45±13% Heliox increased V′E/V′CO2 during constant work rate exercise Habedank (2011) [82] 8 NA Bilateral lung Tx decreased V′E–V′CO2 slope Gagnon (2012) [83] 8 FEV1 7±8% Spinal anesthesia reduced V′E/V′CO2 during constant work rate exercise Kim (2012) [84] 1475 FEV1 <45% LVRS reduced V′E/V′CO2 during unloaded exercise Guenette (2013) [85] 15 FEV1 86±15% ⇑ V′E/V′CO2 at isotime with fluticasone/salmeterol compared to placebo Queiroga (2013) [86] 24 FEV1 35±10% Heliox increased V′E/V′CO2 during constant work rate exercise Armstrong (2015) [87] 55 FEV1 26±7% LVRS reduced V′E/V′CO2 peak and nadir Gloeckl (2017) [88] 10 FEV1 38±8% No effect of whole-body vibration training on V′E/V′CO2 in severe COPD Langer (2018) [89] 20 FEV1 47±19% No effect of inspiratory muscle training on V′E/V′CO2 during constant-WR exercise O’Donnell (2018) [90] 14 FEV1 62±10% No effect of dual bronchodilation on V′E/V′CO2 during constant-WR exercise Behnia (2018) [91] 25 FEV1 1.5±0.6 L No effect of dietary nitrate supplementation on V′E/V′CO2 nadir Elbehairy (2018) [92] 20 FEV1 50±15% No effect of acute bronchodilation on VD/VT and V′E/V′CO2 Perrotta (2019) [93] 25 FEV1 61±22% ⇓ V′E–V′CO2 slope and ⇑ peak V′O2 after high-intensity exercise training Gravier (2019) [94] 50 FEV1 62±19% No effect of pulmonary rehabilitation on lung cancer patients undergoing PR Hasler (2020) [95] 20 FEV1 64±19% ⇓ V′E/V′CO2 and ⇑ WR peak with supplemental O2 in non-hypoxaemic patients ⇓: decreased; ⇑: increased; FEV1: forced expiratory volume in 1 s; CO2: carbon dioxide; GOLD: Global Initiative for Chronic Obstructive Lung Disease; VD/VTphys: physiological dead space; CT: computed tomography; TLCO: transfer factor of the lung for carbon monoxide; V′O2: oxygen uptake; IC: inspiratory capacity; HF: heart failure; ILD: interstitial lung disease; NA: not available/not applicable; WR: work rate; PAH: pulmonary arterial hypertension; CPFE: combined pulmonary fibrosis and emphysema; Tx: transplant; LVRS: lung volume reduction surgery; PR: pulmonary rehabilitation; O2: oxygen; VT: tidal volume; HR: heart rate.
- TABLE 2
Key unanswered questions on the mechanisms and consequences of minute ventilation (V′E)/carbon dioxide output (V′CO2) abnormalities in COPD
Exercise intolerance What are the structural determinants of increased VD/VTphys in milder disease?
What is the relevance of alveolar hyperventilation to increase V′E/V′CO2? Does it change with disease severity?
What is the physiological meaning (if any) of the V′E–V′CO2 intercept?
Is the V′E/V′CO2 consistently associated with specific disease phenotypes?
How does very severe, end-stage disease influence V′E/V′CO2?
Is resting V′E/V′CO2 useful to predict exercise intolerance and dyspnoea in patients unable to exercise?Influence of comorbidities Do emphysema severity and COPD phenotype influence V′E/V′CO2 in COPD-HF?
Do HF aetiology and HF with preserved ejection fraction influence V′E/V′CO2 in COPD-HF?
What is the effect of exertional hypoxia on V′E/V′CO2 in hypoxaemic patients with COPD-HF?
Does V′E/V′CO2 relate to right ventricular–pulmonary arterial coupling in COPD?
How does the severity of restriction influence V′E/V′CO2 in CPFE?Risk assessment/prognosis Why does a high V′E/V′CO2 predict poor peri-operative outcome in lung resection surgery?
What is the best V′E/V′CO2 parameter to predict poor surgical outcome across the spectrum of disease severity?
Does V′E/V′CO2 independently predict poor outcome in severe to very severe patients?
How to best associate V′E/V′CO2 with clinical data to determine prognosis?
Does the longitudinal assessment of V′E/V′CO2 improve prognosis estimation?Effects of interventions What is the most sensitive parameter to detect improvement in V′E/V′CO2?
Can exercise training and/or inspiratory muscle training improve V′E/V′CO2 in selected patients?
Do interventions aimed to improve pulmonary vascular function impact on V′E/V′CO2?
Is there any beneficial effect of specific pharmacological interventions on V′E/V′CO2 in COPD-HF and disproportionate pulmonary hypertension?
Can long-term bronchodilation improve V′E/V′CO2 in selected patients?VD/VTphys: physiological dead space; HF: heart failure; CPFE: combined pulmonary fibrosis and emphysema.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary_figures ERR-0190-2020_Supplementary_figures











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Structural and functional determinants of V′E/V′CO2 in COPD
- Influence of V′E/V′CO2 on the physiological and sensory responses to exercise in COPD
- Impact of COPD comorbidities on V′E/V′CO2
- V′E/V′CO2 for risk assessment and prognosis in COPD
- Effects of interventions on V′E/V′CO2 in COPD
- Applying V′E/V′CO2 to clinical management of COPD
- Conclusions
- Supplementary material
- Footnotes
- References
- Figures & Data
- Info & Metrics