





Abstract
Over the past century rigid bronchoscopy has been established as the main therapeutic means for central airway diseases of both benign and malignant aetiology. Its use requires general anaesthesia and mechanical ventilation usually in the form of manual or high-frequency jet ventilation. Techniques applied to regain patency of the central airways include mechanical debulking, thermal ablation (laser, electrocautery and argon plasma coagulation) and cryo-surgery. Each of these techniques have their advantages and limitations and best results can be attained by combining different modalities according to the type, location and extent of the airway blockage. If needed, deployment of airway endoprostheses (stents), as either fixed-diameter silicone or self-expandable metal stents, may preserve the airways patency often at the cost of several complications. Newer generation of customised stents either three-dimensional printed or drug-eluting stents constitute a promise for improved safety and efficacy results in the near future.
Treating central disease of benign or malignant aetiology, foreign body aspiration or massive bleeding in the airways requires a structured approach with combined techniques, a dedicated team of professionals and experience to treat eventual complications. Specific training and fellowships in interventional pulmonology should therefore be offered to those who wish to specialise in this field.
Abstract
Therapeutic bronchoscopy modalities may effectively treat difficult central airway problems in both malignant and benign diseases. This also involves responsibility for treating related complications. Training in interventional pulmonology is warranted. https://bit.ly/2yWlIjM
Introduction
The principal indications for therapeutic bronchoscopy in central airway diseases include intrinsic obstruction, extrinsic compression or their combination (mixed) due to benign or malignant disease, the management of tracheobronchial bleeding, trachea-oesophageal or bronchopleural fistulae and complex foreign body extraction [1]. Early lung cancer, asthma, bronchitis and emphysema are reported elsewhere in this series.
Rigid bronchoscope was first used more than a century ago to treat central airway obstruction due to foreign body aspiration and remains the therapeutic instrument of choice for central airway diseases. With modern high-fidelity optics, jet ventilation port and all the advantages of ablative techniques, together with its large volume suction capability, the rigid bronchoscope enables the effective re-establishment of airway patency and/or airway prosthesis deployment, while safeguarding ventilation. Flexible bronchoscopy, which has been used extensively since the late 1960s, mostly for diagnostic purposes, has been enhanced since then with high-tech modalities, namely high definition video processors, convex and radial endobronchial ultrasound facilities, ultra-thin and large-calibre working channels, grasping accessories of various types, and hot or cold tissue destruction instruments. Both flexible and rigid modalities can and often have to be used in conjunction to treat central airway diseases [2].
The rigid bronchoscope
The barrel of the rigid bronchoscope is a hollow metal tube with a bevelled edge. Its length varies between 33 and 43 cm with an outer diameter of 6–14 mm. Bronchoscopes are thinner and longer than tracheoscopes and can pass telescopically through them to achieve the gradual dilatation of stenosis. Bronchoscopes have side ventilation fenestrations to permit contralateral airway ventilation when a main bronchus has been intubated (figure 1a). The proximal multifunction head has special ports for all types of ventilation and a working channel through which the telescope (connected to a camera and a light source cable) is inserted, and allows for the manipulation of the aspirator tube, the forceps, and all the other ancillary instruments, including catheters for laser, electrocautery, argon plasma or cryotherapy, as well as a flexible bronchoscope (figure 1b).

a) Rigid bronchoscope shaft with ventilation fenestration passed through a wider tracheoscope. b) Rigid bronchoscope multifunction head: 1) video camera mounted on telescope, 2) light cable, 3) rigid suction tube, 4) grasping forceps, 5) LASER catheter, and 6) ventilation port.
Performing rigid bronchoscopy often requires intravenous general anaesthesia using a combination of propofol and an opioid (fentanyl), together with a short-acting muscle relaxant. Due to the open ventilation circuit, volatile gases cannot be used. At some centres, the procedure is performed under deep sedation with local anaesthesia and spontaneous breathing, which has been correlated with increased rate of complications and thus should be avoided [3]. During the procedure, different ventilation strategies can be applied. Most often, high-frequency or manual jet ventilation is used while controlled ventilation and spontaneous-assisted ventilation are used at some centres [2, 4, 5]. When using a flexible bronchoscope for therapeutic purposes, it is recommended to select one with a larger working channel (2.8 mm) and an insulated tip.
Description of ablative, debulking and dilation techniques
Different techniques are used to restore airway patency, either by ablation, debulking or by dilation according the type of stenosis. In any case, it is important to confirm the presence of a potentially patent airway and viable lung tissue distally of the stenosis, without which the intervention is both dangerous and meaningless.
When abnormal tissue reduces the airway lumen, two kinds of approaches are used, often in combination. Tissue can be removed by mechanical extraction using forceps, the tip of the barrel, the micro-debrider or the cryoprobe and thermal energy can be applied in the form of LASER, electrocautery or argon plasma coagulation (APC). Depending on the energy delivered into the tissue, this will either be vaporised, coagulated or devitalised. Ionising radiation (brachytherapy) and photodynamic therapy are alternative options, though they currently offer fewer advantages and are not frequently used.
Mechanical debulking
Abnormal tissue of both malignant and benign origin can be removed directly with forceps or by pushing the distal bevelled edge of the rigid bronchoscope against the base of the lesion and coring it out under direct visualisation, often using a suction tube or grasping forceps. In order to avoid excessive bleeding following the coring out of the lesion, it is advisable to first coagulate/devascularise the lesion using thermal ablation techniques. After resection, the barrel of the rigid bronchoscope is advanced distally so that haemostasis is effectuated by the radial compression that is exerted on the airway wall by the rigid tube (figure 2). This technique is the quickest way to resect and remove tumours and to control bleeding coming from its base. Nevertheless, it can be difficult in long tumours because portions of resected tumour and blood get into the lumen and vision is blurred. At that point it is crucial not to lose the axis of the airway in which the resection is performed otherwise perforation can occur. In cases in which an attempt to resect has provoked massive bleeding and the procedure has been halted it is possible to reschedule the resection after embolisation [6]. A micro-debrider is an auxiliary instrument with a long disposable rotating blade coupled with suctioning. Debulking with this technique is quick, but control of bleeding may require adjunctive bronchoscopic thermal haemostatic/ablative modalities [7]. Whenever there is important bleeding after mechanical debulking which cannot be effectively controlled by standard measures (compression with the shaft or thermal coagulation), the insertion of a Fogarty balloon (4 or 6 Fr) may block the airway and preserve ventilation in the contralateral lung [7].

Mechanical debulking with the tip of the rigid bronchoscope.
Thermal ablation
Laser stands for “light amplification of stimulated emission of radiation”. This light can be delivered through optical fibres suitable for bronchoscopic applications. Laser wavelength and power density (Watts·mm−2) are the main characteristics that define the suitability of each laser for endoscopic treatment. Depending on the laser wavelength, effects can penetrate up to 10 mm and have a bigger or smaller ratio of absorption and scattering in soft tissue (figure 3). The absorption and scattering of the laser beam also depends on tissue composition (e.g. water, blood, fat) and its colour. Dark tissues absorb nearly all the light, whereas clear colours let the light penetrate further. Lasers with high absorption and scattering coefficients, like the Nd:YAP (Nd-doped yttrium-aluminium-perovskite) with a 1340 nm wavelength, are potent coagulators but have poor cutting precision. However, CO2 LASER with a 10 600 nm wavelength has a poor coagulation effect but far superior cutting precision. Power density mainly depends on the watts delivered and the distance between the tip of the laser fibre and the target. Distance is highly determining of power density; as distance increases, the power density diminishes as well as the effect on tissue. Laser can be used in noncontact mode within air-cooled catheters or in contact mode, with nude fibres. Noncontact mode allows the surgeon to work easily without the need for the constantly cleaning of the tip of debris and blood. Current laser equipment is smaller, more portable and more affordable than ever.

Laser yttrium aluminium perovskite photocoagulation on a tracheal tumour.
The photocoagulation effect is easily seen as the tumour surface turns white, which is known as the blanching effect. This is achieved at low power settings and/or by placing the tip of the laser probe 1 cm away from the target. If the power density increases by raising the power and/or advancing the tip of the laser probe, the tissue is carbonised and vaporised, and the operator observes a blackening and charring of the tumour.
The laser fibre can also be used through the flexible bronchoscope while the flexible scope is passing through the rigid scope thus combining all available modalities [8–10]. Protective eyewear is mandatory when the laser beam is activated, though the risk of harm to medical personnel is minimal since observation is performed via video camera. Reducing inspiratory oxygen fraction <40% when activating LASER, electrocautery or APC (discussed below) is advised to prevent endobronchial fire. If jet ventilation is used, it is preferable to discontinue the jet while activating the thermal modality.
Electrocautery is a contact mode ablation technique based on electric current flow. Electrons generate heat for tissue coagulation due to the higher resistance of the target tissue. Different types of unipolar electrodes are available (including blunt probe, knife, forceps and wire snare loops) but achieving the essential contact of the probe with the mucosa (thus suctioning secretion, blood or debris) at the site of treatment is of utmost importance for this technique to be effective. Tissue effect depends on the wattage setting, the surface area of contact (a smaller probe will increase current density) and the time during which energy is applied [11–14]. A new catheter that allows for coagulation and cut modes with a depth of penetrations <2 mm and with an integrated suction function has also been introduced recently with promising results [15]. One of the limitations of monopolar electric current modalities is the interaction they might have with pacemakers, which have to be inactivated before the initiation of the procedure.
APC is a noncontact technique that utilises ionised argon gas (plasma) to conduct monopolar electrical current to the nearest tissue. Its depth of penetration is <3 mm, making APC very safe but useful mainly for coagulation/haemostasis or for treating superficial and flat lesions [16, 17]. APC is suitable for treating bronchial segments at an acute angle (i.e. apical and posterior segments of the upper lobes) because the argon gas flows around bends and corners. This approach offers an advantage over laser bundles, which always leave the probe in a straight path. Although argon is generally safe and is not combustible in itself, endoscopic fire can be ignited in its presence together with high oxygen concentrations. Gas embolisation is a rare, albeit the most severe (sometimes fatal) complication that may be encountered when using APC [12, 18].
Electrocautery/APC purchase and maintenance costs are low; applicators are re-usable and cheap and can be used through the flexible bronchoscope as well, while the technique is simple and easy. In comparison, LASERs come with a much higher cost of implementation and maintenance, have a steeper learning curve and are more dangerous. Although lasers may in general be more powerful and rapidly effective, when building a new interventional pulmonology unit, electrocautery/APC as far as the thermal ablation technique goes, offers more logistical advantages over laser [12, 13].
Photodynamic therapy is a unique biopharmaceutical modality where an injectable photosensitising drug delivered prior to the procedure is selectively retained in tumour cells and is subsequently activated by specific wavelength light. This creates reactive oxygen species resulting in local cytotoxicity and an enhanced anti-tumour response allowing for destruction of tumour sites. The tumour undergoes necrosis after exposure to light and debris accumulates at the site over the next 48 h. A second bronchoscopy is required 2–3 days after each light administration for the debridement and the re-establishment of airway patency. Photodynamic therapy is approved for use as a definitive treatment in early stage superficial lung cancer and palliation in advanced stages of the disease. However, due to its prolonged photosensitisation, it is not practical to use in regions with ample sunlight. Given its high cost and complicated logistics, as well as the delayed effect of its action, it does not present any special advantage over the other thermal techniques described above. Its use, however, is suggested as part of a multimodality approach scheme [19–21].
Cryotherapy
Freezing of the bronchoscopic cryoprobe is achieved with the Joules–Thomson effect: the expansion of a previously compressed gas generates an immediate drop in temperature. The most common gases for medical use are nitrous oxide or carbon dioxide, which are decompressed at the tip of the cryoprobe, generating a freezing effect of −70 to −90°C. The endoscopic application of extreme cold can be used for three purposes. 1) Cryo-recanalisation is a contact mode based on the adherence of the tumour to the end of the frozen cryoprobe and its immediate retraction along with large fragmented tissue. Large pieces of tumour can be removed instantly with this technique, though thermocoagulation may be required afterwards to control bleeding [22–24]. 2) Cryotherapy can also be applied as a delayed effect technique based on the cellular damage produced by repeated cycles of freezing and thawing. It produces delayed necrosis followed by sloughing, which may be expectorated or removed bronchoscopically. 3) Cryo-spray, a noncontact mode, has also been introduced recently. A specialised flexible catheter delivers liquid nitrogen uniformly. This noncontact mode technique achieves 5 mm depth of tissue destruction in <10 s. Despite these advantages and the relative simplicity of the procedure, there is also a risk of severe barotrauma if the gas is not vented. When liquid nitrogen is released into the warm airway, there occurs an almost instantaneous conversion to gas with a resulting volume expansion of the order of 1:645. The main risk is therefore barotrauma including pneumothorax, pneumomediastinum and nitrogen gas embolism, which, though rare, can prove fatal [25].
Balloon dilatation
High-pressure balloon dilatation is a useful and easy-to-perform technique for opening stenotic airways. Balloons are made of low-compliance inflatable polymers that allow for a uniform and reproducible expansion to a specified diameter on inflation. They are filled with saline and hydraulic pressure of the balloon is monitored manometrically, achieving an excellent correlation between diameter and pressure. Wire guidance with or without fluoroscopy support is used to pass through a high-grade stenosis or across an irregular stenosis when bronchoscopic guidance is not feasible.
It is important to select an appropriate size for the balloon, in terms of both length and final diameter, as too short a length will result in the slipping of the balloon, while excessive length could potentially result in distal airway trauma. Excessively small diameters will not obtain significant changes and too large diameters can easily provoke complications. Mucosal and transmural tearing, bleeding, pneumomediastinum and pneumothorax have been reported [26, 27]. Special caution is needed when the stenosis is not fully circumferential and the healthy posterior wall is exposed to high pressure. To prevent many complications, a step-by-step increment of pressure in 30 s to 1-min periods is recommended to achieve smooth dilatation.
The dilation effect of the balloon is usually temporary and complementary techniques are therefore usually required after dilatation, such as debulking, resection, ablation, stent placement and mitomycin C application [28–30].
Stents
Silicone or self-expandable metallic stents (SEMS), either fully or partially covered, may achieve sustained dilatation on the stenotic portion of the airway and assure ventilation. Silicone stents have thicker walls than metallic stents (1 mm versus 0.25 mm), are less adaptable to airway anatomy and always require a rigid bronchoscope to be implanted and removed (figure 4). However, they can remain in place for years and are much easier to remove.
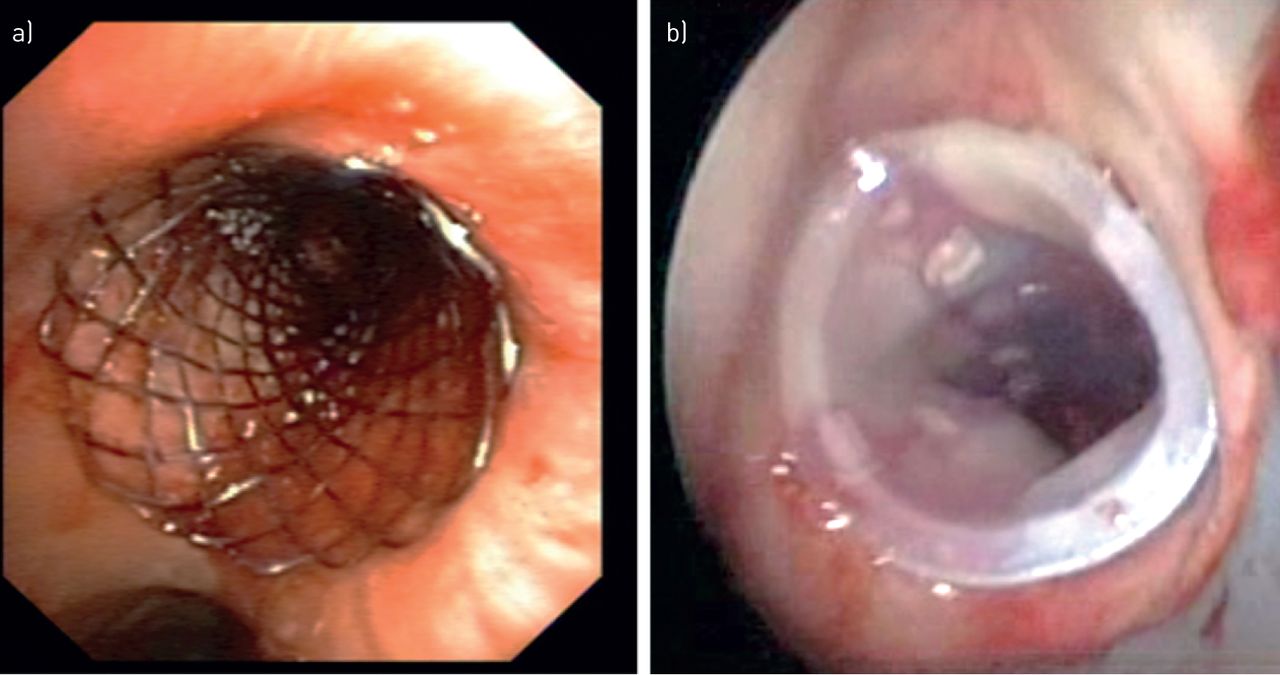
a) Silicon and b) metal stents.
SEMS have a better performance in malignant airway stenosis with a complex or conical anatomy including fistulas and can be implanted with a flexible or rigid bronchoscope. Nevertheless, rigid bronchoscopy always guarantees a better airway control.
Since 2005, following a US Food and Drug Administration (FDA) recommendation, metallic stents have not been used for benign airway strictures due to the high rate of complications and even deaths reported. Nevertheless, a new generation of SEMS has been commercialised since this warning. These fully covered SEMS have been tested in small retrospective studies. One study with 16 patients did not register deaths associated with the stents and their removal was feasible in all the cases reported [31]. In a more recent study with 30 patients there were no associated deaths and successful removal was achieved in 90% of cases [32]. These studies show the feasibility and safety of these new stents, though a comparative study with the silicone stent as the gold standard is needed to draw robust conclusions. Complications are frequent with both types of stents. In a retrospective cohort study with follow-up bronchoscopies in 94 patients bearing 100 stents of various types, complications were detected in 69%. They were mainly obstruction by secretions (37%), obstruction by tumour/granulation tissue growth (27%) and migration (20%). A univariate analysis comparing fully covered SEMS and straight silicone stents did not reach statistical significance (OR 0.17 (95% CI) 0.03–1.00) [33].
The introduction of self-expanding metallic tracheobronchial bifurcated “Y-shaped” stents has resolved some of the limitations of the silicone Y stents, including asymmetrical main bronchi diameters, pure extrinsic compression and wide main carinas. The procedure is usually performed under fluoroscopy, which provides full visual control. On some occasions, these stents have been implanted with flexible bronchoscopy [34]. Nevertheless, their removal is only possible under rigid bronchoscopy.
Customised silicone stents are set to play an essential role in the near future as complex anatomy indications are resolved and many complications, such as migration and granulation, are considerably diminished. The first published use of an airway customised three-dimensional (3D)-printed silicone stent took place in France in 2017. This stent was used successfully on a patient with stenosis and partial dehiscence of the bronchial anastomosis in his lung allograft [35]. More recently, US FDA clearance to implant a 3D-silicon stent that had been customised for compassionate use was obtained for the first time in the USA. Two patients with complicated airway disease due to granulomatosis with polyangiitis were successfully stented [36]. Nevertheless, there remain regulatory and technological difficulties to overcome before customised silicone stents can be made commercially available. Randomised comparative studies will be needed before the inclusion of new generation stents in the guidelines.
Management of malignant central airway disease
More than one-third of patients with nonsmall cell lung cancer develop clinically significant central airway obstruction at presentation or during the course of the disease. Primary tracheal tumours, as well as metastatic tumours of any histology from distant sites, can grow in the central airways. Symptoms include inspiratory or expiratory stridor, exertional dyspnoea, post-obstructive pneumonia, haemoptysis and atelectasis of varying degrees depending on their size and location. Extrinsic compression from mediastinal nodes, lymphomas, thyroid, or oesophageal cancer can also produce stenosis and/or fistulae. Imaging and endoscopic assessment are required to classify the obstruction as endoluminal, extraluminal, causing extrinsic compression or mixed and treat it accordingly. Interventional management in malignant central airway obstruction is warranted in symptomatic patients and when distal airways are potentially patent. If the disease invades peripheral airways and lung parenchyma entirely, there is no indication for interventional management [37].
Recanalisation endoscopic modalities include mechanical and cryo-debulking techniques and/or thermal ablation and coagulation (electrocautery, argon plasma, laser or photodynamic treatment). If after debulking of endoluminal tumour, a substantial grade of stenosis persists either because of coexisting extrinsic compression (mixed disease) or because of focal tracheomalacia leading to expiratory airway collapse, the insertion of a stent should be encountered. In cases of pure extrinsic compression, airway wall involvement and related tracheo-bronchomalacia, stent placement is usually required to maintain airway patency. Carinal involvement may require interventions in both main bronchi, as well as the deployment of a bifurcated Y-shaped stent to retain patency. Tracheoesophageal fistulae due to malignant erosion of the airway wall or following external beam radiation may severely impact the clinical status of the patient and require urgent management, usually by the deployment of tracheal and/or oesophageal stents. However, the dual stenting of trachea and oesophagus has been related to catastrophic complications due to extreme ischaemia of both lumen walls and should therefore be avoided when possible. As long as the restoration of airway patency is achieved, the clinical result is equally important regardless of the modality that has been applied [38].
If interventional procedures succeed in re-establishing patency of the airways, survival rates are comparable to those for patients without central airway obstruction [39, 40]. Other studies have shown that the interventional management of patients with malignant central airway obstruction may achieve immediate clinical and pulmonary function improvement with less dyspnoea and better quality of life. There is also evidence that these functional and clinical benefits are sustained over time and are related to prolonged survival when included in a multidisciplinary oncological management algorithm [3, 41].
Early complications related to airway intervention include airway bleeding, hypoxia, hypercapnia vocal cord injury and pneumothorax. In the AQuiRe study, the 30-day mortality rate (14.8%) varied substantially among centres (range 7.7–20.2%, p=0.002). Risk factors included impaired clinical status, intrinsic or mixed obstruction and stent placement [42].
Management of nonmalignant central airway disease
Nonmalignant tracheal stenosis encompasses a wide variety of disorders producing either fixed or dynamic airway narrowing. Post-tracheostomy and post-intubation tracheal stenosis are the most commonly encountered disorders. The erosion of cartilages around the stoma or inflated tracheal tube cuff and their consequent healing through contraction produces either a triangular (A-shape) or web-like stenosis. To these cicatricial lesions, a degree of tracheomalacia is often added.
When tracheal stenosis starts to become symptomatic, it already affects 50–75% of the airway calibre, and the remaining patent airway does not exceed 5 mm. A detailed characterisation and classification of the aetiology, morphology, localisation, extent of disease, and degree of functional impairment is warranted before a therapeutic decision is made [42, 43]
Interventional bronchoscopic techniques include dilatation, laser or electrocautery web resection and silicone stent (including T-tube) placement. Radial incisions and gentle dilatation may cure short, web-like stenoses definitively.
In complex cases, surgical management (sleeve resection of the trachea with end-to-end anastomosis) remains the treatment of choice. However, this is a demanding surgical operation in which few thoracic surgeons have substantial experience. Post-surgery, the long-term recurrence rate has been reported to be as high as 15%, and the reported post-operative mortality rate ranges from 1.8% to 5% [44–46]. In a large surgical study on 494 patients reporting a relapse rate of 10.5%, length of stenosis, tension at the site of anastomosis, subglottic involvement and anastomotic infection were the factors which corelated with the surgical failure [47]. If the surgeon is not willing to proceed in the first place or the patient (or the stricture) is not amenable to surgery, silicone stents help to splint lengthy and complex strictures and relieve obstructive symptomatology.
However, a stent is always a foreign body implanted in the trachea and may therefore be related to a number of complications, such as mucous retention, biofilm development and foul breath, granulation tissue formation over the edges of the stent, stent migration and stent fracture. Stent removal after 12–18 months and re-evaluation of the situation is recommended. If an indication persists, surgical management may be proposed, or if the patient is still deemed inoperable, replacement of the stent may be indicated. A recent randomised trial has suggested that endoscopic management is superior to surgical management for patients with idiopathic subglottic stenosis [48]. A multidisciplinary approach involving pulmonologists, thoracic and ear, nose and throat surgeons is crucial for the optimum management of patients.
Foreign body aspiration, bronchial haemorrhage management and atelectasis due to mucus retention
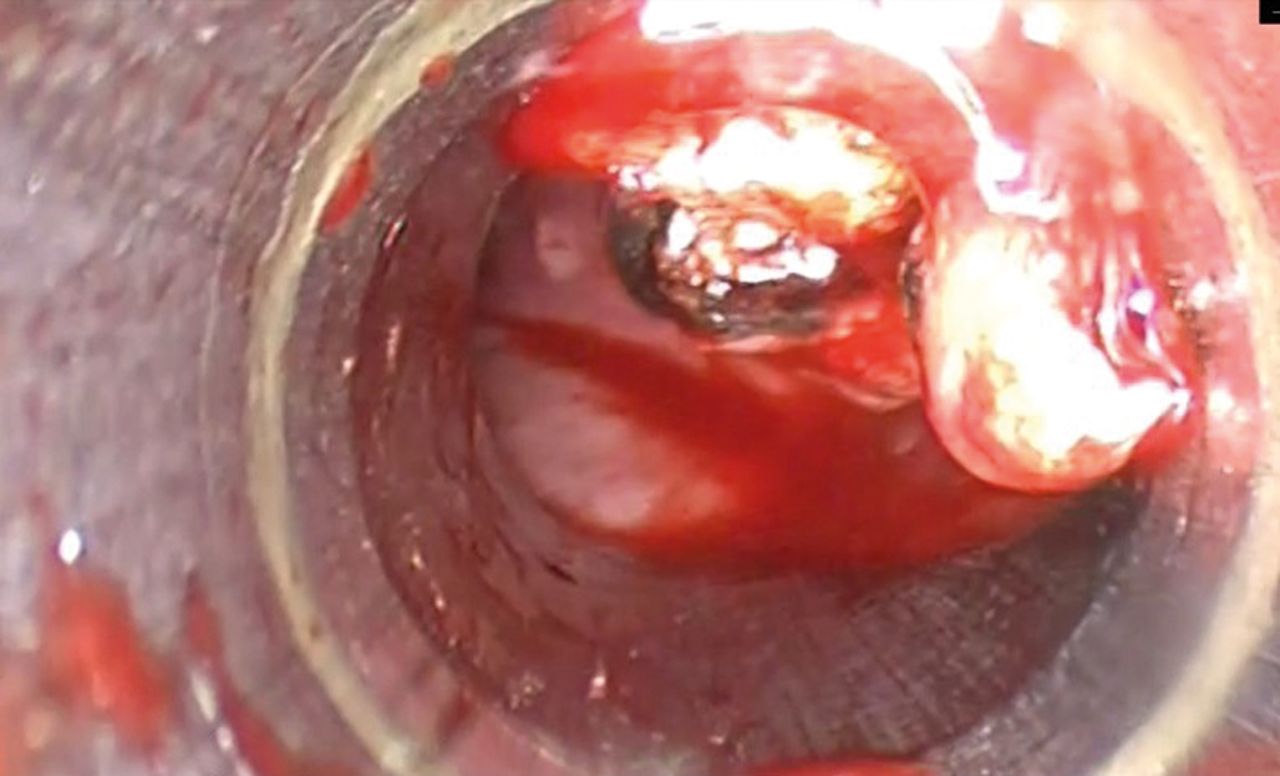
Rigid bronchoscopy plays a crucial role in foreign body aspiration, especially in those that are bigger than the laryngeal introit, have cutting, sharp or pointed ends and are difficult to hold with flexible instruments, or need previous granuloma coagulation and debulking (figure 5). Rigid bronchoscopy is strongly recommended in children and in those cases with stridor or asphyxia, where fast action is required to assure ventilation. Flexible bronchoscopy (through the mouth), performed with the adequate ancillary instruments, can also be effective at removing foreign bodies, though the procedure without orotracheal intubation may be risky and jeopardise ventilation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Foreign body removal.
In those patients with massive haemoptysis, urgent rigid bronchoscopy is not indicated unless bleeding from a well-localised endoluminal lesion is the cause. In the case of clot removal, rigid or flexible bronchoscopy, with or without cryoprobe extraction, can be very quick and safe. The demand for extracting clots in intubated patients in intensive care units is increasing as veno-venous extracorporeal membrane oxygenation is more often indicated. Unfortunately, this development carries with it a higher prevalence of pulmonary haemorrhage. In literature, bleeding complications under extracorporeal membrane oxygenation are reported in around 29% of investigated cases [49]. Cryo-extraction is successful in >90% of cases, though the procedure has to be repeated in nearly 50% of cases [50].
Mucus plugs are mostly related to a stent complication. In cases of thick and dense mucus, warm saline flushing through a flexible bronchoscope with a working channel of at least 2.8 mm may be enough to aspirate the mucus plugs. The instillation of mucolytic agents has not proved to be effective so far. When mucus plugs represent a life-threatening situation or when flexible bronchoscopy removal has failed, rigid bronchoscopy is recommended. A 3-mm inner aspiration catheter or even debulking with the tip of the instrument can solve the problem rapidly. Pseudo-membranes are formed by the ischaemic and necrotic mucosa especially after the removal of longstanding stents or an orotracheal tube. They may be sticky and hard to expectorate and can lead to airway obstruction and suffocation. Rigid bronchoscopy is the safest and most efficient way of removing them.
Conclusions
Modern rigid bronchoscopic modalities are the most efficient methods for treating central airway disease of either a malignant or a benign pathology. It is performed more safely under general i.v. anaesthesia and muscle relaxation with jet ventilation. Flexible bronchoscopy is commonly performed through a rigid tracheoscope. If necessary, after regaining the patency of the airway, the deployment of stents may be performed to retain patency and avoid restenosis. Combining multiple ablative modalities with flexible and/or rigid instruments may result in optimal patient outcomes. Performing therapeutic interventions in the central airways also involves accepting responsibility for treating resulting complications. Specific training and fellowships in interventional pulmonology should be made available for those who wish to specialise in this field.
Footnotes
Number 4 in the Series “Interventional pulmonology” Edited by David Feller-Kopman and Hervé Dutau
Previous articles in this series: No. 1: DeMaio A, Sterman D. Bronchoscopic intratumoural therapies for nonsmall cell lung cancer. Eur Respir Rev 2020; 29: 200028. No. 2: Chandrika S, Yarmus L. Recent developments in advanced diagnostic bronchoscopy. Eur Respir Rev 2020; 29: 190184. No. 3: Kniese CM, Musani AI. Bronchoscopic treatment of inoperable nonsmall cell lung cancer. Eur Respir Rev 2020; 29: 200035.
Provenance: Commissioned article, peer reviewed.
Conflict of interest: A. Rosell has nothing to disclose.
Conflict of interest: G. Stratakos has nothing to disclose.
- Received December 12, 2019.
- Accepted April 27, 2020.
- Copyright ©ERS 2020.
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










Jump To
- Article
- Abstract
- Abstract
- Introduction
- The rigid bronchoscope
- Description of ablative, debulking and dilation techniques
- Management of malignant central airway disease
- Management of nonmalignant central airway disease
- Foreign body aspiration, bronchial haemorrhage management and atelectasis due to mucus retention
- Conclusions
- Footnotes
- References
- Figures & Data
- Info & Metrics