





Abstract
Pulmonary hypertension (PH) is a clinical condition characterised by elevation of pulmonary arterial pressure (PAP) above normal range due to various aetiologies. While cardiac right-heart catheterisation (RHC) remains the gold standard and mandatory for establishing the diagnosis of PH, noninvasive imaging of the heart plays a central role in the diagnosis and management of all forms of PH. Although Doppler echocardiography (ECHO) can measure a range of haemodynamic and anatomical variables, it has limited utility for visualisation of the pulmonary artery and, oftentimes, the right ventricle. Cardiovascular magnetic resonance (CMR) provides comprehensive information about the anatomical and functional aspects of the pulmonary artery and right ventricle that are of prognostic significance for assessment of long-term outcomes in disease progression. CMR is suited for serial follow-up of patients with PH due to its noninvasive nature, high sensitivity to changes in anatomical and functional parameters, and high reproducibility. In recent years, there has been growing interest in the use of CMR derived parameters as surrogate endpoints for early-phase PH clinical trials. This review will discuss the role of CMR in the diagnosis and management of PH, including current applications and future developments, in comparison to other existing major imaging modalities.
Abstract
This review discusses the role of cardiovascular magnetic resonance in the diagnosis and management of pulmonary hypertension, including current applications and future developments, in comparison to other existing major imaging modalities. http://bit.ly/39RXPb0
Epidemiology, classification and clinical manifestations of pulmonary hypertension
The taskforce for the 6th World Symposium on Pulmonary Hypertension (2019) proposed a modified haemodynamic definition for pulmonary hypertension (PH) of mean pulmonary arterial pressure (PAP) >20 mmHg and defined precapillary PH (also known as pulmonary arterial hypertension (PAH)) by the concomitant presence of mean PAP >20 mmHg, pulmonary vascular resistance (PVR) ≥3 Wood units and pulmonary artery wedge pressure (PAWP) ≤15 mmHg [1]. Clinical PH groups (table 1) previously classified at the 4th World Symposium on PH and endorsed by the European Society of Cardiology (ESC)/European Respiratory Society (ERS) [2] were updated.
World Health Organization (WHO) groups of pulmonary hypertension (PH) and cardiovascular magnetic resonance (CMR)
PH is characterised by excessive intimal proliferation, fibrosis and severe vasoconstriction in the pulmonary vasculature with resultant pressure overload on the right ventricle. Although the actual prevalence of PH is not certain, data from registries estimate mortality at 6.5 deaths per 1000 000 people with 131 hospitalisations per 100 000 discharges in the United States between 2001 and 2010 [3]. PH is more common amongst women with a median survival of 2.8 years without treatment [4]. There are three defined stages of the disease: asymptomatic compensated, symptomatic compensated and advanced decompensated [5–7]. The clinical manifestations of PH are due to progressive right ventricular failure with symptoms of dyspnoea, fatigue, angina and, in advanced cases, syncope.
Importance of evaluating the right ventricle
Despite the morbidity and mortality associated with PH from right ventricular dysfunction and failure, the focus of management has been primarily on pulmonary circulation (probably because of the availability of medications that cause pulmonary vasodilatation). The three major classes of therapy currently available also specifically target pulmonary circulation. The rationale for this strategy is that improvement in pulmonary haemodynamics would naturally improve the right ventricle as the afterload abates. However, recent studies have cast credible doubt on this theory [8–11]. Two widely accepted observations that have influenced thinking about this are that patients with idiopathic PAH (IPAH) have much better right ventricular function and better clinical course than patients with systemic sclerosis (SSc) despite having similar haemodynamics. Also, despite the improvement in haemodynamics, right ventricular function may continue to deteriorate as evident from the study by van de Veerdoonk et al. [8]. The disease progression in PH is mainly due to two interrelated factors, pulmonary artery non-compliance and right ventricular dysfunction. Therefore, for a true evaluation of the disease process it is crucial to assess both the right ventricle and pulmonary artery (table 1) [12].
Diagnosis of pulmonary hypertension with other existing modalities and their challenges
Right-heart catheterisation (RHC) is the current guideline-recommended gold standard for confirming PH. RHC offers reliable assessment of PAP but fails to provide a comprehensive assessment of the condition of the right ventricle, thereby limiting assessment of vital data such as right ventricle–pulmonary artery coupling and left ventricle–right ventricle interdependence [12]. RHC is invasive with potential for serious complications including bleeding, pneumothorax, pulmonary artery rupture, infection and heart block, especially in the presence of existing conduction abnormalities. Early studies reported a high fatality rate (4.2%, Fuster et al. [13]) and a major procedure-related complication rate (5.3%, Rich et al. [14]) for RHC. Recent studies indicate that when RHC is performed in experienced centres it is a relatively safe procedure with low risk for major complications (around 1%) and procedure-related mortality (around 0.1%) [15–17]. The higher complication risk is reported when RHC is performed in paediatric patients [16], under general anaesthesia [16], or using the femoral vein route [15, 17] and is likely performed in less experienced medical centres. The Multicenter RePHerral study demonstrated that many newly diagnosed patients with PH referred to an expert centre did not receive RHC as part of their diagnostic procedure and a substantial portion of such patients were misdiagnosed and inappropriately treated [18]. Lack of training, cost and perceptions of complication risks were possible reasons for not performing RHC. This emphasises the need for reliable noninvasive tools for initial screening and management of PH patients.
The current routine noninvasive imaging modality for screening patients with clinical suspicion of PH is a transthoracic echocardiography (ECHO) (figure 1) [2]. Transthoracic ECHO uses the modified Bernoulli equation for assessing right ventricular systolic pressure (RVSP) by calculating the pressure difference between the right ventricle and the right atrium based on the velocity of the tricuspid regurgitant jet and adding the right atrial pressure [19]. Transthoracic ECHO allows evaluation of right ventricular adaptation to increased afterload, using the right ventricle myocardial performance index (also known as the Tei index) [20]. However, transthoracic ECHO has significant critical limitations as the technique is operator dependent and often fails to provide a reliable assessment of right ventricular function due to the lack of standard geometry to allow use of model assumptions [21]. A study by Fisher et al. [19] looking into the accuracy of transthoracic ECHO in comparison to RHC found transthoracic ECHO estimates of PAP to be accurate in only 50% of patients. The tricuspid annular plane systolic excursion (TAPSE) is a common and widely utilised echocardiographic metric used to approximate right ventricular ejection fraction (RVEF) [22]. TAPSE is easily obtained by M-mode ECHO of the right ventricular annulus, with normal values being >20 mm and markedly reduced in the case of right ventricular dysfunction [23]. However, diagnostic and prognostic values of TAPSE suffer from several prominent limitations [24]. Since it focuses only on a small part of the right ventricular myocardium and is affected by overall heart motion, it cannot be considered a comprehensive surrogate for entire right ventricle function [25]. TAPSE is both angle and load dependent, and this needs to be considered in the case of significant tricuspid regurgitation, when right ventricular base active motion may falsely reflect overall right ventricular contractile function. Due to ventricular interdependence, left ventricular systolic motion may also affect TAPSE [26, 27].

{kind=link}
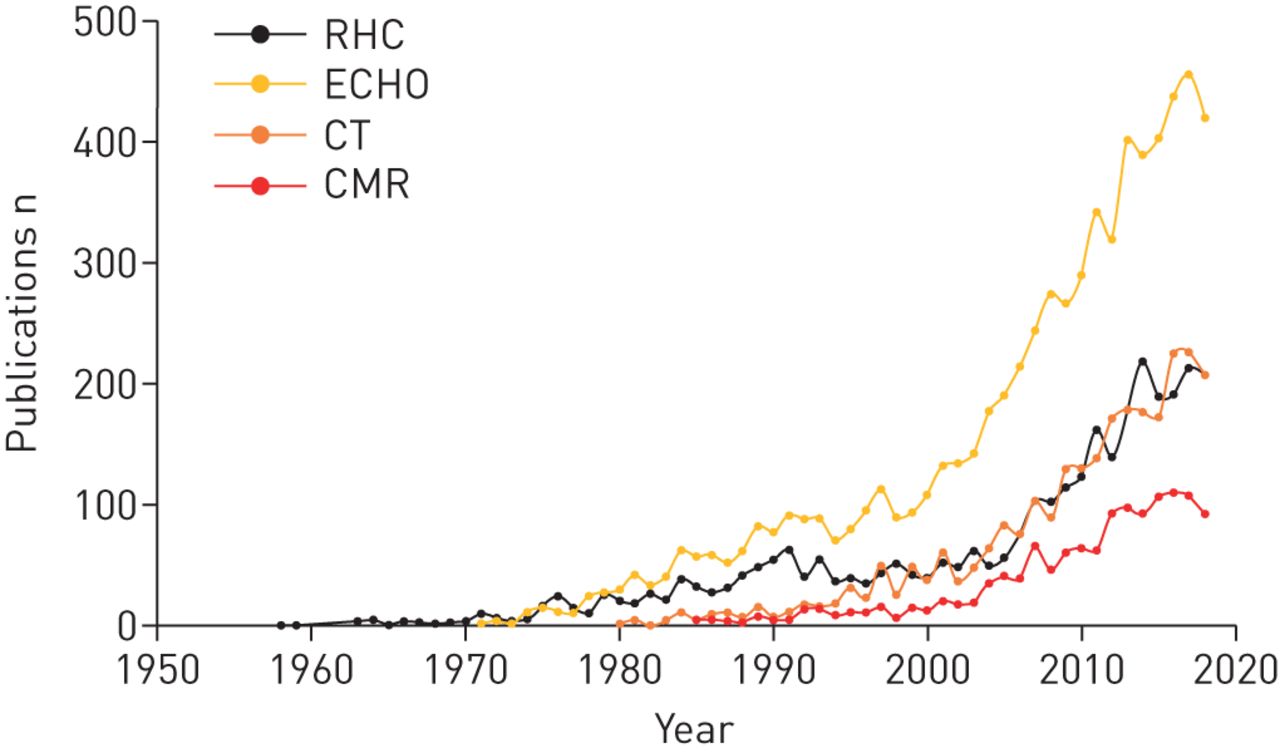
Number of clinical publications on the use of evaluation modalities in humans with pulmonary hypertension (PH), as indexed in PubMed between 1958 and 2018 (unadjusted, searched in October 2019). RHC: right-heart catheterisation; ECHO: echocardiography; CT: computed tomography; CMR: cardiovascular magnetic resonance.
Computed tomography (CT) is another preferred imaging modality for the assessment of PH, due to its excellent spatial and temporal resolution, and quick scan time, which offers a comprehensive evaluation of cardiopulmonary structures [28]. Patients with suspicion of PH routinely undergo non-electrocardiogram (ECG)-gated, contrast-enhanced CT for the evaluation of pulmonary artery and lung parenchyma. In the event of clinical suspicion of pulmonary embolism (PE), an ECG-gated computed tomography angiography (CTA) is performed. ECG-gated CTA can demonstrate signs of right ventricular failure such as right ventricular hypertrophy, abnormal curvature or leftward bowing of the interventricular septum (IVS), right ventricular dilation (often defined as a right ventricle diameter : left ventricle diameter ratio >1:1 at the mid-ventricular level), pericardial effusion and, possibly, even tricuspid regurgitation [5]. A ratio of CT-measured main pulmonary artery transverse diameter : ascending aorta diameter >1 is also highly indicative of PH, with a 96% positive predictive value [29]. CT can help identify causes for PH, such as parenchymal abnormalities in patients with World Health Organization (WHO) group II disease. Furthermore, multiple significant ground-glass opacities may support the diagnosis of pulmonary capillary haemangiomatosis (PCH) [30]. The presence of oesophageal dilation may hint at scleroderma as the cause of PH and a computed tomography pulmonary angiogram (CTPA) allows for the assessment of patients with chronic thromboembolic pulmonary hypertension (CTEPH) being considered for surgical candidacy [31]. Although ventilation/perfusion (V/Q) scanning is considered as the initial imaging modality of choice, once the diagnosis of CTEPH is suggested, CTPA is commonly used to assess the extent of disease and the subsequent cardiopulmonary changes [32]. It should be noted, however, that CT has limitations, with its inability to provide detailed haemodynamic information being a major drawback. Due to significant radiation exposure, the use of CT in patients who need repeat examinations is also less desirable.
Use of cardiovascular magnetic resonance in management of pulmonary hypertension
Although PH is a disease primarily of the pulmonary vasculature, the most common cause of morbidity and mortality is right ventricular failure. Cardiovascular magnetic resonance (CMR) is a three dimensional (3-D) tomographic technique that is considered to be the gold standard for assessing right ventricular function, volume, mass and structure [20]. CMR, with its inherent properties of high spatial and temporal resolution combined with the fact that it does not rely on patients having favourable acoustic windows, provides the most comprehensive information on the right ventricle. Although the use of CMR in PH goes back more than two decades, it is still considered a novel imaging modality in comparison to the other noninvasive imaging modalities like transthoracic ECHO (figure 1). A common factor resulting in relatively low utilisation of CMR is the inability to provide a reliable estimation of PAP [33, 34], considered to be crucial in the assessment and management of PH. However, recent studies have demonstrated that elevated mean PAP can be predicted by CMR using regression models comprising simple and easy to obtain CMR metrics [35, 36]. A correlation between mean PAP and/or PVR, and multiple CMR-derived metrics has been also reported in many clinical research studies [37–41]. Nevertheless, it has been well established that, in PH, PAP in isolation provides no prognostic information whereas the condition of the right ventricle is what determines survival [42, 43].
Most of the studies on PH have focused on estimating PAP and other parameters derived from pressure without simultaneous emphasis on the right ventricle. This is an incomplete approach as both the right ventricle and pulmonary artery are affected in PH with a differential influence on outcomes. Therefore, CMR can bridge this gap by evaluating both the right ventricle and the pulmonary artery to provide a comprehensive picture [37, 38, 40, 44, 45]. This approach could be cost-effective as comprehensive CMR has the potential to replace other ancillary imaging modalities.
The presence or absence of specific CMR findings may provide clues as to the cause of PH. The presence of aberrant pulmonary veins or other intracardiac shunt lesions may be suggestive of an aetiology for PAH, whereas left ventricular hypertrophy or dysfunction, or left atrial dilation, may suggest PH due to left-sided congestive heart failure (table 1). Crawley et al. [46] have demonstrated that CMR-measured left atrial volume alone has a 97% sensitivity and 100% specificity in differentiating IPAH from PH due to heart failure with preserved ejection fraction (HFpEF). Similarly, magnetic resonance angiography (MRA) can be used to assess pulmonary vessel pruning seen in IPAH, as well as filling defects in the pulmonary vasculature suggestive of CTEPH [47]. Although MRA generally has lower spatial resolution than CTA, MRA techniques with resolution reasonably comparable to CTA may have the edge over the latter for evaluation of pulmonary vasculature, due to the lack of ionising radiation and nephrotoxic contrast agents [48].
A routine CMR study consists of various gradient-echo and phase contrast cine sequences, and the measurements derived from these provide a detailed assessment of the right ventricle and of right ventricle–pulmonary artery coupling that are essential for a thorough evaluation of PH stage (table 2). Cine CMR (see supplementary material) is a technique that displays cardiac motion in a cine loop after creating multiple sequential images of the heart throughout the cardiac cycle. Due to high tissue contrast between the myocardium and blood on gradient-echo imaging, particularly with steady state free procession (SSFP) imaging (see supplementary material), cyclic changes in cardiac structures (such as chambers and ventricular walls) can be displayed. This in turn allows the quantification of ventricular mass, volumes and wall motion, and thereby provides important information about cardiac function. Cine phase contrast imaging (see supplementary material) acquires a series of velocity-sensitive images within a cardiac cycle and can be used to measure blood flow or tissue motion velocity. In the typical display modes, stationary tissue appears gray on the phase contrast image, while the flowing blood would appear as white or black depending on the direction of the flow relative to the velocity-encoding gradients. The phase contrast technique can also be applied to measure flow velocity in 3-D. The data obtained can be analysed to generate virtual stream lines that represent blood flow within a vessel or cardiac chamber [49, 50]. Four-dimensional (4-D) flow analysis (3-D flow plus time) has been introduced recently for the assessment of pulmonary circulation and for PH diagnostics [51–53], and this may eventually become the preferred method for measuring all forms of vascular flow. Enhanced tissue signal intensity/contrast is achieved by adjusting scan pulse sequences in respect to parameters of myocardium/blood/fat/water T1 and T2 relaxation times, and strength of magnetic field. For a more comprehensive analysis of blood flow and differential properties of myocardial tissue, dynamic contrast is achieved by adding a contrast agent, usually a water-soluble gadolinium (Gd) chelate.
Sequential right-sided changes due to pulmonary hypertension (PH) detected by cardiovascular magnetic resonance (CMR) modalities
Determining prognosis and risk assessment
CMR provides information on a number of variables associated with prognostication and risk assessment. RVEF is an important CMR measurement for prognosis assessment. Van de Veerdonk et al. [8] have shown that RVEF at baseline is a more robust predictor of mortality than PVR. Right ventricular stroke volume (RVSV) is another indicator of right ventricular function and is a prognostic measure, with low RVSV shown to be strongly associated with mortality both at baseline and on treatment [54]. Van Wolferen et al. [55] have shown that RVSV measured by CMR correlates well with 6-min walk test (6 MWT) distances in patients with PAH (p<0.0001), with an increase in RVSV of >10 mL during treatment correlating with a significant improvement in 6 MWT distance of >41 m. Left ventricular end diastolic volume (LVEDV) and right ventricular end diastolic volume (RVEDV) are independent predictors of prognosis in IPAH, with increased mortality seen in patients with reduced values [56].
CMR can assess secondary cardiac changes associated with PH, such as right ventricular dilation (typically defined as a right ventricle : left ventricle diameter >1 in axial images) [57]. Right ventricular hypertrophy, an effect of increased and sustained afterload in PH (defined as right ventricular wall thickness (RVWT) >4 mm), results in higher right ventricular mass (RVM). A right ventricular mass index (RVMI) >59 g·m−2 (as measured by CMR) is associated with increased mortality in patients with IPAH [10]. A ventricular mass ratio (defined as RVM/left ventricular mass (LVM)) >0.6 has an 84% sensitivity and 71% specificity for the diagnosis of PH [28, 58].
In advanced PH, the conventional rightward-convex ventricular septum is either flattened or bowed during systole towards the left ventricle, resulting in the left ventricle becoming D-shaped and the right ventricle subsequently becoming concentric [59]. The resultant effect of this septal bowing is a reduction in RVEF that has a strong correlation with the measurement of the paradoxical curvature of the IVS and the severity of PH [60]. The presence of pericardial effusion also indicates poor prognosis [61].
Contrast agents can provide additional important diagnostic/prognostic value in a CMR study of PH. After intravenous injection of the contrast agent, it travels between the intravascular space and the interstitial space but does not enter the intracellular space and demonstrates different concentration–time curves in the normal and abnormal myocardium. Compared to healthy cardiac tissues, abnormal myocardium such as infarcted or scarred myocardium tend to retain more contrast on a per-unit-volume basis due to the loss of intact cardiomyocytes and expanded interstitial space [62]. In PH patients, injection of Gd-based contrast agents can produce late gadolinium enhancement (LGE) due to its higher volume of distribution and delayed washout in the regions of scarring or fibrosis, which is often seen at the right ventricular insertion point (RVIP) at the IVS between the right and left ventricles. The results of various studies have suggested a significant inverse correlation between the degree of RVIP LGE and RVEF and haemodynamics [63–66]. RVIP LGE may therefore be useful as a prognostic marker and an indicator of more advanced right ventricular changes, especially in patients with PAH and, as such, it may assist in risk stratification and enabling appropriate therapy to be administered promptly [67]. The volume of LGE, which correlates well with RVM, volume, remodelling and dysfunction, also has prognostic value [67]. A higher degree of enhancement suggests poorer right ventricular performance, which in turn is associated with poorer prognosis [65, 68]. A Gd-based contrast agent can also be used to assess myocardial perfusion reserve in response to pharmacologically-induced stress (e.g. by adenosine) or exercise. It has been reported that reduced right and left ventricular myocardial perfusion reserves are associated with elevated mean PAP in PAH patients and are closely correlated to increased right ventricular workload and right ventricular dysfunction [69].
The use of a Gd-based contrast agent is considered generally safe. The most common side effects are mild and include headaches, nausea, itchiness, dizziness, vomiting and inflammation. However, in very rare cases, Gd-chelate contrast agents can produce a rare disease known as nephrogenic systemic fibrosis (NSF) in the presence of severe kidney failure [70]. Some of the Gd-chelate contrast agents (group 2 agents, e.g. gadobenate dimeglumine and gadoteridol) are much less likely to cause NSF in patients with chronic kidney disease [71] and care should therefore be exercised in the choice of appropriate contrast agent in respect to patient renal function. Recently, native T1-mapping has been introduced as an alternative technique to LGE for characterisation of the myocardium without the use of contrast agents [72]. T1-mapping quantifies the T1 relaxation time per pixel of tissue and T1-values increase when the heart is affected by oedema and fibrosis [73, 74]. Spruijt et al. [75] have reported that native T1-values for the interventricular insertion regions are significantly increased in precapillary PH and are related to disease severity. In patients with postcapillary PH due to HFpEF, Nitsche et al. [76] have shown that interstitial expansion of the anterior right ventricular interventricular insertion, as detected by CMR T1-mapping, reflects haemodynamic alterations and is independently associated with long-term outcome.
Cardiac output in phase contrast CMR has been shown to be an independent predictor for prognosis, with the presence of slow flow in the main pulmonary artery associated with adverse prognosis and mortality [45]. A number of phase contrast CMR measured indices of pulmonary artery haemodynamics, including flow and flow velocity metrics, have been reported to correlate with mean PAP and PVR [37, 38, 77], and thus have important diagnostic/prognostic values in PH patient management. Interestingly, a study by Gan et al. [78] has shown that the degree of pulmonary artery relative area change (RAC) is the strongest predictor of death (more powerful than 6 MWT, PAP, cardiac output and right atrial pressure), with a value ≤16% being associated with poor prognosis. Pulmonary artery RAC (or pulsatility), a noninvasive measure of pulmonary artery stiffness, is defined as: (maximal pulmonary artery area – minimum pulmonary artery area)/minimum pulmonary artery area [40, 78–80]. Area change (AC) is defined as: maximal area – minimum area, with the maximal and minimal pulmonary artery cross-sectional areas traced from CMR cine images. Swift et al. [44] have subsequently demonstrated that both RAC and AC are good predictors of adverse outcome in PH. Pulmonary artery pulse-wave velocity (PWV), another noninvasive measure of pulmonary artery stiffness, is increased in PH patients and has an important prognostic value [81, 82]. CMR exercise stress offers great potential in clinical practice to noninvasively assess vascular function in the right ventricle and the pulmonary artery. Cardiac output and PWV increase in response to acute moderate exercise in healthy subjects and PH patients, while RAC decreases; however, PWV appears to increase more in PH patients [83, 84]. In PAH patients, stroke volume increased in WHO functional class I and decreased in WHO functional class II in response to exercise [85]. Thus, exercise CMR stratifies patients initially perceived as having a low risk of mortality into different degrees of right ventricular inotropic reserve, with a reduced stroke volume during exercise becoming a contributing factor to increased risk of decompensation [85]. However, the prognostic utility of these CMR-derived variables, including RVEF, needs to be validated in large prospective trials as their promise has been assessed primarily based on retrospective analysis.
Determining response to therapy
Although RHC will continue to be the gold standard test for initial diagnosis of PAH, the role of CMR in serial monitoring to determine treatment response is growing. CMR can be utilised during follow-up to estimate the measure of response to therapy and the degree of clinical worsening, as well as to assist with treatment decisions. Traditionally RHC has been favoured as the gold standard to assess the response to therapy. However, recent studies suggest that CMR may also have value, possibly even more so than RHC due to its noninvasive nature and ability to provide a comprehensive evaluation of both the right ventricle and the pulmonary artery (thus providing an accurate assessment of disease progression) [86–88]. For example, an increase in pulmonary artery RAC of >10% signifies a good response to pulmonary vasodilator therapy [44, 89].
A pilot study by Jardim et al. [89] has shown (in 19 patients with IPAH) that CMR evaluation of the RAC in the main pulmonary artery (immediately after a RHC procedure) correlates well with vasodilator response (p=0.01) and that an RAC cut-off value of 10% allows responders to be distinguished from nonresponders with 100% sensitivity and 56% specificity. The ability of CMR to reliably evaluate right ventricular function, mass and size has been used in endpoints in trials using sildenafil [90] and bosentan [11]. Furthermore, the large prospective EURO-MR study has shown that CMR measurements taken at baseline and at subsequent follow-up provide credible information about patient response to vasodilator therapy [91].
In a study by Roeleveld et al. [92], CMR has been performed to assess treatment response in 11 IPAH patients on continuous intravenous epoprostenol over 1 year. Patients showed significant improvement in RVSV during the first 4 months of treatment, with good correlation observed between the improvement in RVSV and increase in 6 MWT. In a study by Allanore et al. [93], involving 18 patients with PAH due to SSc who were treated with bosentan, CMR in combination with tissue Doppler ECHO showed improvement in myocardial perfusion and myocardial function after 4 weeks of treatment. CMR was also used in a study by Reesink et al. [94] to evaluate right and left ventricular remodelling in 17 patients with CTEPH at 4 months following pulmonary endarterectomy. Post-surgery CMR showed normalisation of right and left ventricular volume with leftward ventricular septal bowing.
Using cardiovascular magnetic resonance measurements as trial endpoints
The change in 6 MWT has been the most widely used primary endpoint in many PAH clinical trials, mainly due to its ease of use, noninvasive nature and low cost. It has also been used for regulatory approval of therapies for patients with PAH. However, the validation of 6 MWT is so far restricted to patients with IPAH and patients with PAH due to connective tissue disorder (CTD). 6 MWT is also affected by many variables, mainly comorbidities, age, muscular training, motivation and mood, and therefore may not provide a true reflection of cardiac condition. Furthermore, 6 MWT loses its sensitivity in patients with mild symptoms and a considerable baseline walking distance, but with a high burden of disease, as observed in a bosentan trial in WHO functional group 2 PH patients [95–97]. 6 MWT also loses its reliability in patients already on a background therapy, as shown in the Pulmonary Hypertension Response to Tadalafil (PHIRST) trial, where patients treated with tadalafil in combination with a background therapy showed only a modest improvement in 6 MWT when compared to treatment naïve patients who received tadalafil alone [98]. This aspect is essential to consider when utilising 6 MWT as a primary endpoint for studies involving an “add-on” therapy in addition to an existing background therapy. Here, it becomes paramount to use metrics other than 6 MWT with sufficient sensitivity to capture additional treatment effects due to the new agents.
In CMR studies of PH, 6 MWT or its change due to treatment correlate with both routine CMR metrics (including RVEF and LVEDV, RVEF and RVSV [11], and RVSV [55]) and more sophisticated metrics (such as percentage of myocardial fibrosis [99]). CMR has the best inter-study reproducibility of all imaging modalities for the measurement of right ventricular chamber volume and mass, making it a crucial tool for clinical trials in PAH [100]. Due to these factors, the focus for PAH trial endpoints has been shifting away from the traditional measurement of 6 MWT, which suffers from the inherent limitations mentioned above, to a more reliable, reproducible assessment of the right ventricle by CMR [101].
Studies showing good correlation between RHC-measured PVR and CMR derived parameters suggest the possibility of using CMR data as a surrogate for RHC, especially in serial follow-up in patients with PAH to assess progress or response to therapy [102]. Since the mortality associated with PH is due to progressive right ventricular dysfunction, it becomes essential to have a primary endpoint which provides a better physical characterisation of the right ventricle at baseline and with response to therapy. For instance, in the SERAPH (Sildenafil versus Endothelin Receptor Antagonist for Pulmonary Hypertension) study of patients with IPAH, change in RVM measured by CMR is considered as the primary endpoint [103]. Other complete and ongoing clinical studies/clinical trials utilising CMR endpoints are described in table 3.
Pulmonary arterial hypertension (PAH) studies, both complete and ongoing, utilising cardiovascular magnetic resonance (CMR) endpoints
Advantages and disadvantages of cardiovascular magnetic resonance in pulmonary hypertension
Whereas other imaging modalities have limited capabilities in assessing PH, CMR with its comprehensive measurements can become a “one-stop shop” for evaluation of PH and its therapeutic management. Since the condition of the right ventricle is what determines survival in PH, CMR with its robust assessment of right ventricular structure and function compares well to RHC. Although RHC is considered to be the gold standard for haemodynamic evaluation, CMR can potentially deliver a reliable and noninvasive estimation of PAP and pulmonary blood volume, thereby allowing examination of the right ventricle and pulmonary artery as one unit in order to provide a detailed understanding of disease process and progression, as well as to provide assistance with management (table 4). However, despite extensive research there are still limited data on the clinical use of pulmonary circulation imaging by CMR in PH. Therefore, it is difficult to compare the utility of CMR, ECHO and CT in this respect. However, CMR would avoid the limitations of ECHO (due to a poor echo window) in a substantial patient cohort with advanced lung disease [108]. Overall diagnostic and prognostic values of the major noninvasive imaging modalities in PH have not been comprehensively compared. In one single-centre retrospective study (n=81), CMR and ECHO had greater diagnostic utility than CT in assessment of PAH in patients with CTD, while CMR also provided prognostic value [109]. Recent studies have found that despite correlation between ECHO metrics for evaluation of right ventricular systolic function (e.g. TAPSE, right ventricular fractional area change (RAC) and the Tei index) and CMR-derived RVEF, ECHO metrics show limited accuracy in predicting improvement or deterioration of right ventricular systolic function during serial follow-up assessment in PAH patients [110, 111]. These studies indicate that CMR remains the gold standard for the serial assessment of right ventricular systolic function.
Comparative assessment of diagnostic modalities in pulmonary hypertension (PH)
In comparison to ECHO or CT, CMR has a number of advantages due to its overall excellent spatial resolution, lack of the need for geometric assumptions for ventricle assessment, reproducibility and lack of ionising radiation. With a single brief breath hold and using cardiac gating, multiple scans can be obtained without the problems of respiratory motion artifacts. Despite these obvious attractive features, CMR suffers from limited temporal resolution in comparison to ECHO, making it less suitable for dynamic measurements. Longer scan time (albeit getting shorter with advancement in technology) and incompatibility with magnetic objects (i.e. metallic hardware, implants, clips and pacemakers etc) also limit its use (table 4), although the latter is also becoming less problematic with the advent of magnetic resonance conditional implanted electronic devices. Furthermore, the accessibility of CMR for widespread utilisation is somewhat limited due to cost, the expertise required to perform scans and analyse images, and limited familiarity about its capabilities among non-imaging-specialist physicians. Further advances in technology and education may help to increase its use.
Conclusion
The mounting use of CMR in providing a comprehensive assessment of the right ventricle and pulmonary artery for the global management of PH is encouraging. Despite higher costs, limited availability and the requirement for trained expertise, CMR stands out distinctly in comparison to other conventional imaging tools like ECHO in providing not only detailed anatomic data but also additional vital information related to diagnosis, prognostication, disease progression and response to therapy. As the technology continues to evolve and access becomes more widespread, CMR has the potential to emerge as the noninvasive imaging modality of choice for comprehensive evaluation of PH. A profound acceptance of this significant but under-utilised technology requires a widespread understanding of its immense potential, the realisation of the importance of the right ventricle and not just PAP in the optimal management of PH, and development of standardised protocols and unitisation in multicenter PH trials. The implementation of standardised protocols could lead to shorter scan times with a reduction in cost and would ultimately make the imaging technology more realistic for broader use.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
ERR-0138-2019_Supplementary video ERR-0138-2019_Supplementary_video
Footnotes
This article has an editorial commentary: https://doi.org/10.1183/16000617.0139-2020
This article has supplementary material available from err.ersjournals.com
Provenance: Submitted article, peer reviewed
Conflict of interest: S.R. Aryal has nothing to disclose.
Conflict of interest: O.F. Sharifov has nothing to disclose.
Conflict of interest: S.G. Lloyd has nothing to disclose.
- Received October 16, 2019.
- Accepted December 31, 2019.
- Copyright ©ERS 2020.
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Epidemiology, classification and clinical manifestations of pulmonary hypertension
- Importance of evaluating the right ventricle
- Diagnosis of pulmonary hypertension with other existing modalities and their challenges
- Use of cardiovascular magnetic resonance in management of pulmonary hypertension
- Determining prognosis and risk assessment
- Determining response to therapy
- Using cardiovascular magnetic resonance measurements as trial endpoints
- Advantages and disadvantages of cardiovascular magnetic resonance in pulmonary hypertension
- Conclusion
- Supplementary material
- Footnotes
- References
- Figures & Data
- Info & Metrics