





Abstract
Very old (aged ≥80 years) adults constitute an increasing proportion of the global population. Currently, this subgroup of patients represents an important percentage of patients admitted to the intensive care unit. Community-acquired pneumonia (CAP) frequently affects very old adults. However, there are no specific recommendations for the management of critically ill very old CAP patients. Multiple morbidities, polypharmacy, immunosenescence and frailty contribute to an increased risk of pneumonia in this population. CAP in critically ill very old patients is associated with higher short- and long-term mortality; however, because of its uncommon presentation, diagnosis can be very difficult. Management of critically ill very old CAP patients should be guided by their baseline characteristics, clinical presentation and risk factors for multidrug-resistant pathogens. Hospitalisation in intermediate care may be a good option for critical ill very old CAP patients who do not require invasive procedures and for whom intensive care is questionable in terms of benefit.
Abstract
There is currently no international recommendation for the management of critically ill older patients over 80 years of age with CAP. We report and discuss recent literature in order to help physicians in the decision-making process of these patients. http://bit.ly/2ql0mIz
What is the role of community-acquired pneumonia in critically ill very old patients?
Community-acquired pneumonia (CAP) is a major public health problem with high morbidity, mortality and short- and long-term sequelae [1–4]. Very old (aged ≥80 years) patients are at increased risk of complications and death by most causes [5]. The incidence of CAP in very old patients continues to rise [6]. The immunosenescence [7], multicomorbidities [8] and frailty [9] of these patients increases their susceptibility to infectious diseases [10, 11]. Moreover, it is reported that CAP is associated with a 16% reduction in quality of life during the post-discharge year among elderly patients (mean age 76 years in cases and controls) who survive to hospitalisation for CAP, compared to non-diseased persons [12].
Currently, due to their increased life expectation, over the past two decades the proportion of very old patients admitted to intensive care units (ICUs) has grown significantly worldwide [6, 13, 14], increasing healthcare costs [15–17]. The percentage of very old patients admitted to ICUs ranges from 9–20% in several countries [13, 18–24]. A recent French study reported the 10-year (2006 to 2015) trends in ICU admissions for respiratory infections in the elderly population. The authors found that the absolute number and the percentage of elderly patients admitted to ICUs increased, with the greatest rise in patients aged ≥85 years (11% in 2006 versus 16% in 2015) [6]. Moreover, a recent Spanish study [25] investigated risk factors for mortality in critically ill elderly and very old patients with sepsis in 77 ICUs. Pneumonia was the main cause of sepsis, affecting 62% of very old patients; mortality for sepsis in very old patients was 54%. Similarly, the study by Cilloniz et al. [26] on the topic of sepsis secondary to CAP in very old patients reported that 11% of these patients required ICU admission and 14% developed sepsis with an ICU mortality of 17%.
In this review, we discuss important findings and gaps in knowledge concerning the management of critically ill very old patients with CAP, and propose a series of recommendations to guide basic principles of CAP management in these patients while further evidence is gathered (figure 1).

General recommendations for the management of critically ill very old community-acquired pneumonia (CAP) patients. PSI: pneumonia severity index; ATS: American Thoracic Society; ICU: intensive care unit. #: in addition to the antibiotics recommended in guidelines, ceftaroline+macrolide/ceftobiprole+macrolide could be a good option for this population.
Clinical presentation of pneumonia in very old patients
Immunosenescence reduces the ability of very old patients to respond to an infection [27]. Some specific symptoms of lower respiratory infection such as cough, fever and chest pain may be atypical in very old patients with pneumonia [28], thus increasing the risk of misdiagnosis and delaying the initiation of the empiric antimicrobial therapy [29, 30]. For these reasons, pneumonia may be associated with high morbidity and mortality and poor long-term outcomes in this subgroup of patients [29, 31]. Falls, altered mental status (e.g. delirium), fatigue, lethargy, anorexia, tachypnoea and tachycardia are the most frequent symptoms associated with pneumonia in very old patients [32, 33]. Pneumonia may also be associated with an exacerbation or decompensation of previous chronic comorbidities (diabetes mellitus, cardiac disease, chronic pulmonary disease). Radiographic findings are inconclusive or difficult to interpret in approximately 30% of cases [34]. The inadequate inflammatory response to an infection due to immunosenescence [35, 36] may also lead to an underestimation of pneumonia severity. However, data regarding the role of biomarkers (leukocyte count, C-reactive protein, procalcitonin) in the early diagnosis and prognosis of pneumonia in critically ill very old patients are limited [37].
What parameters might help guide the management of CAP in critically ill very old patients?
Since the short- and long-term prognosis of critically ill very old patients with CAP mostly depends on previous functional status rather than on the severity of pneumonia at ICU admission, improved tools for patient prognosis in this particular subgroup would be extremely helpful [31, 38].
Age-related changes: immunosenescence and sarcopenia
It is expected that in 2080, the current proportion of people aged ≥80 years will have more than doubled, from 6% to 13% of the European population [39].
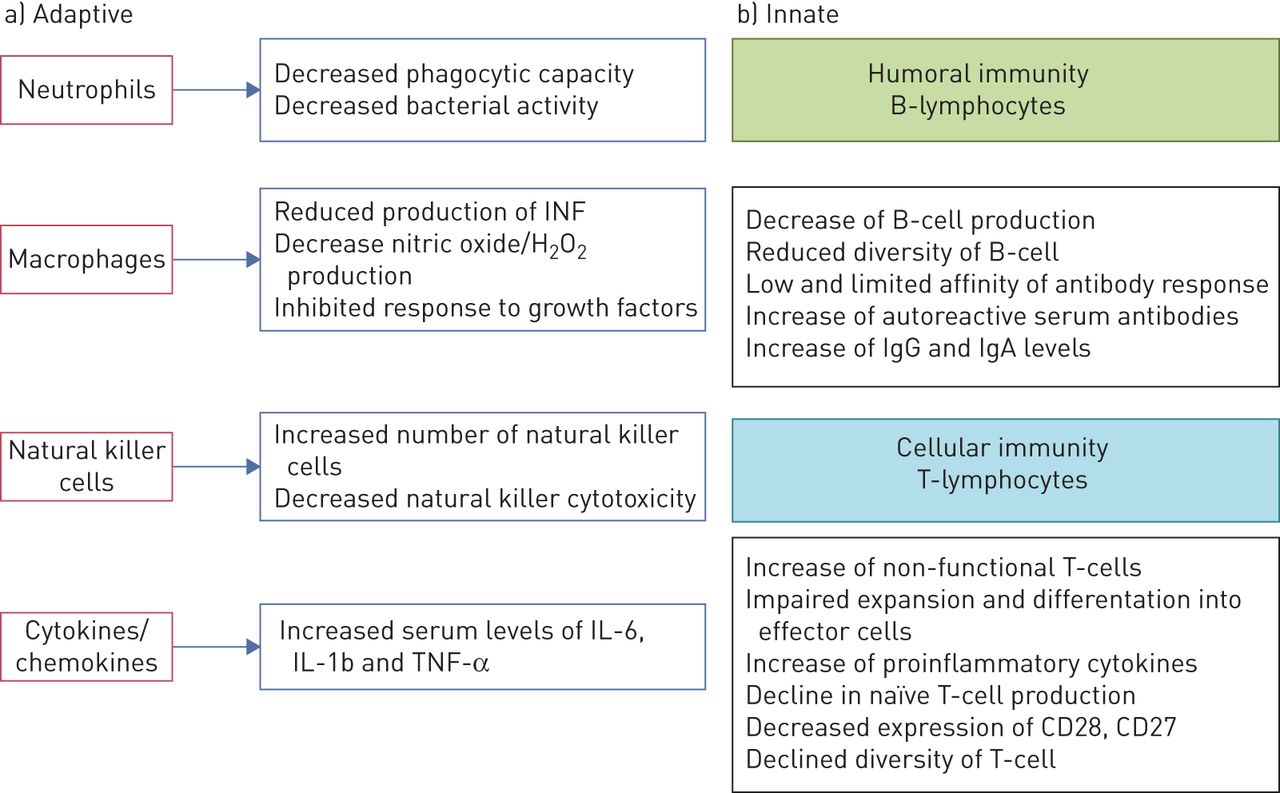
Immunological age-related changes (immunosenescence) gradually reduce the efficiency of the innate and adaptive immune systems [7]. Few naïve cells, increased dysfunctional memory cells and primary lymphoid organ involution may explain the susceptibility of very old patients to infectious diseases, especially those caused by Streptococcus pneumoniae and respiratory viruses [35]. Important barriers to infection, such as the cough reflex and fever, are also affected by immunosenescence. Figure 2 shows age-related changes in the innate and adaptive immune systems.

Changes in the adaptive and innate immune system. INF: interferon; IL: interleukin; TNF: tumour necrosis factor; Ig: immunoglobulin.
Sarcopenia is a geriatric syndrome characterised by a loss of skeletal muscle mass and a decrease of muscle strength or physical performance. Some studies have reported that sarcopenia is an independent risk factor for CAP and for some adverse outcomes (length of hospital stay, readmission or death) [40–43]. Martinez et al. [41] studied the frequency of sarcopenia in 110 hospitalised elderly patients. The prevalence of sarcopenia in very old patients was 12%. Recently, a study from Peru [43] determined the incidence and risk factors of CAP in older adults with sarcopenia. CAP affected 15% of sarcopenic patients, with a mean age of 82 years. The authors reported that sarcopenia and smoking habits were risk factors for CAP. Unfortunately, data regarding the prevalence and impact of sarcopenia in critically ill very old patients with CAP are limited.
Comorbidities
Very old patients suffer from a variety of chronic diseases that affect the integrity of resistance to an infection. Chronic respiratory diseases, diabetes mellitus, chronic heart disease, COPD and chronic neurological diseases are the most frequent comorbidities reported in critically ill very old patients with CAP [6, 11, 44]. They are associated with longer hospital stays, ICU admission, sepsis [45–47], hospital readmission [48, 49] and mortality [11]. In a Spanish study assessing the impact of age and comorbidities on the aetiology of pneumonia, 80% of CAP patients had at least one comorbidity (chronic respiratory disease, diabetes mellitus, chronic cardiovascular disease, neurological disease, chronic liver disease or chronic renal disease) with rates varying according to age group, being 81% in patients aged >75 years. The most frequent comorbidity in all the age groups was chronic pulmonary disease (54%). COPD was the most frequent respiratory comorbidity, decreasing in frequency with age. The percentage of comorbidities in critically ill very old patients and very old patients hospitalised on a general ward was similar (81% versus 78%, p=0.26). However, diabetes mellitus was more frequent in critically ill very old patients compared to very old patients hospitalised on general wards (22% versus 31%, p=0.012), whereas neurological diseases were less frequent in critically ill very old patients than in very old patients hospitalised on general wards (30% versus 17%, p=0.001) (data not published) [44].
Similarly, Luna et al. [11] investigated the effect of age and comorbidities on CAP mortality in 6205 patients, reporting mortality rates of 14% in very old patients. Moreover, in patients with no or only one comorbidity, age ≥80 years was associated with increased mortality.
Recently, chronic renal disease and diabetes mellitus have been described as independent risk factors for sepsis secondary to CAP in very old patients, while antibiotic therapy before admission was independently associated with a lower risk of sepsis [26]. Chronic renal disease and neurological disease were reported as independent risk factors for 30-day mortality in very old patients with sepsis secondary to CAP.
Malnutrition
Malnutrition is strongly related to the ageing of the immune system. In 2008, Riquelme et al. [32] studied the clinical and nutritional features of 109 elderly patients with CAP. They reported that 77% of patients presented with malnutrition. In their multivariate analysis, malnutrition (OR 2.7), an albumin level ≤3.4 g·dL−1 (OR 2.7) and brachial muscle perimeter ≤24 cm (OR 4.0) were related to an increased risk of in-hospital mortality.
Two recent papers confirmed the important role of malnutrition in the outcomes of CAP patients. The first study evaluated risk factors associated with hospitalisation in 199 home-healthcare patients with CAP from Taiwan; the mean age of the study population was 82±11 years [50]. The authors reported that 83% of patients presented with anaemia and 34% with hypoalbuminaemia. In their multivariate analysis, anaemia (OR 2.37) and hypoalbuminaemia (OR 1.57) significantly increased the risk of hospitalisation for CAP. The second study evaluated the prevalence and prognostic value of malnutrition in two groups of CAP patients (aged ≥65 and <65 years) from Korea [51]. The authors found that the prevalence of malnutrition in the entire cohort was 39%, and it was higher in the elderly group (53% versus 12%, p=0.001). Malnutrition (OR 2.52) and Charlson comorbidity index score (OR 1.30) were associated with 2-year mortality.
There are no data about malnutrition and critically ill very old patients with CAP. Since malnutrition is associated with worse short- and long-term outcomes in very old patients with CAP, continual assessment of patient nutritional status is recommended in order not to underestimate, underdiagnose or undertreat it.
Frailty
Frailty is associated with adverse clinical outcomes in older hospitalised patients. It is characterised by a loss of biological reserves, a failure of homeostatic mechanisms and an increased vulnerability to adversities such as falls, disability, hospitalisation, cognitive decline and loss of independence. The prevalence of frailty rises steadily with age: from 4% in the 65–69-year-old group to 7% at 70–74 years, 9% at 75–79 years, 16% at 80–84 years and 26% in the those aged ≥85 years [52, 53]. A transnational prospective study set up by the European Society of Intensive Care Medicine, with the participation of 311 ICUs from 21 European countries, investigated the impact of frailty on the outcomes of 5021 critically ill very old patients. Frailty (values ≥5 in the Clinical Frailty Scale (CFS)) was present in 43% of patients and was independently related to 30-day survival [54].
Frailty should be measured in routine clinical practice in order to improve the management of elderly patients with CAP. However, there is no international standard for its assessment. The CFS derived from the Frailty Index (FI) proposed by Rockwood et al. [55] is the most frequently used: FI=number of deficits in an individual/total number of deficits measured. It includes variables that represent a range of states, conditions and physiological systems such as mobility, disability, self-rated general health, eyesight, hearing and chronic diseases. The CFS established nine categories for older people: 1) very fit; 2) well, 3) managing well; 4) vulnerable; 5) mildly frail; 6) moderately frail; 7) severely frail; 8) very severely frail; and 9) terminally ill (figure 3).
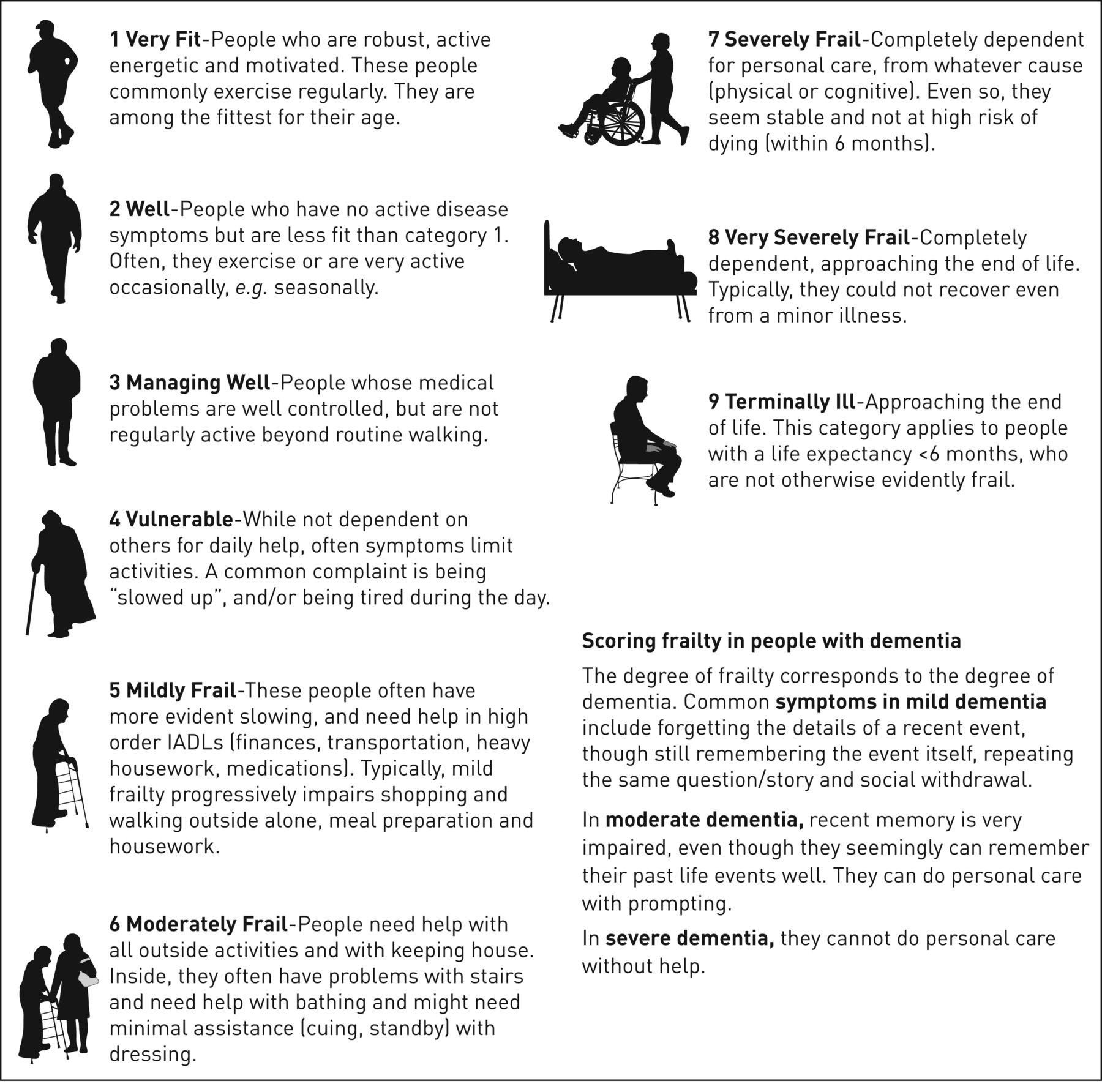
Clinical Frailty Scale. IADLs: instrumental activities of daily living.
In 2018, Gilbert et al. [56] proposed the Hospital Frailty Risk Score, which is based on 109 diagnostic field codes from the National Health Service Hospital Episode Statistics database. The score was developed and validated in three UK populations, with high prognostic performance. The score is divided into three categories: low frailty risk (score <5); intermediate frailty risk (5–15); and high frailty risk (>15). The score was further validated in a tertiary care hospital in Switzerland [57]. The study population comprised 4957 patients: 64% were classified as low frailty risk, 34% as intermediate and 3% as high frailty risk. Patients at intermediate and high frailty risk showed an increased risk of 30-day mortality (OR 2.53 and OR 4.40, respectively, p<0.001) compared with patients in the low frailty risk group. The authors also found that patients with higher frailty risk have longer hospital stay, more severe functional impairment and a lower quality of life. The study confirmed the prognostic value of the Hospital Frailty Risk Score.
Polypharmacy
Because of their chronic conditions, older patients are at increased risk of polypharmacy [58], side-effects and drug–drug interactions [59, 60].
In a study from Canada [61], including 2105 older CAP patients, 45% of patients used four or five medications at baseline. Cardiovascular (63%), alimentary tract and metabolism (49%), nervous system (47%), respiratory (38%), blood and blood-forming and general anti-infective for systemic use (21%) drugs were the most frequently used. The authors also observed that in the 90-day period following a CAP episode, the rate of patients with polypharmacy increased from 45% to 74%.
Because of their multiple comorbidities and polypharmacy, choosing empiric antimicrobial therapy may be challenging in very old patients with infections such as pneumonia [60].
ICU benefit in very old patients: role of severity scores
Currently, 10–20% of all ICU admissions involve very old patients [18, 20–23, 44]. However, the effectiveness of ICU management in this subgroup of patients remains controversial. Since not all very old patients are fragile, advanced age per se should not be a limitation to receive critical care therapy.
Disease severity in CAP is used to assess the prognosis and to guide patient management [4]. In critically ill very old patients with pneumonia, the lack of validated criteria and severity scores that accurately identify those patients that would benefit from ICU admission represents a major issue [62]. The most frequently used severity scores in CAP (pneumonia severity index (PSI) [63], CURB65 (confusion, (urea >7 mmol·L−1), respiratory rate ≥30 breaths·min−1, blood pressure < 90mmHg (systolic) ≤60 mmHg (diastolic), age ≥65 years) and CRB65 [64]) have some limitations for elderly patients: in the PSI, age and comorbidities score more highly, whereas in CRB65 and CURB65, the low number of variables affects the inclusion of all patients with severe CAP.
The Eldicus study [65] investigated the effect of ICU triage decisions on mortality. Refusal benefited overall mortality according to increasing age, where the group of patients aged >84 years had the highest rate of mortality (36%).
More recently, in a Norwegian multicentre observational study [66], 30% of very old patients were refused ICU treatment. Factors increasing the likelihood of ICU refusal in patients considered too ill/old were advanced age, male sex, university hospital admission, comorbidity and low functional status.
Recently, a US study on pneumonia hospitalisation in adults [67] including 119 537 patients, found that approximately 19% required ICU admission and 13% required mechanical ventilation. The rate of pneumonia hospitalisation with ICU admission was 76 per 100 000 persons per year in the overall population. In adults aged ≥85 years, the rates of hospitalisation and ICU admission were 53 times higher (4368 per 100 000) and 46 times higher (695 per 100 000) than in the younger group (18–49 years; 83 per 100 000 persons per year for hospitalisation and 15 per 100 000 persons per year for ICU admission).
A European study [6] of ICU admission due to respiratory infections in the elderly population (<75, 75–79, 80–84, 85–89 and ≥90 years) over 10 years (2006 to 2015) was also published. The authors reported that 3% of all hospitalisations (n=3 856 785 cases) were due to an acute respiratory infection (n=98 381 cases) and that 15% of those cases required ICU admission (n=15 267 cases). The authors found that there was an overall increase in the number of ICU admissions for all age groups, but with the greatest increases in patients aged 85–89 years (3.3-fold) and ≥90 years (5.8-fold). Interestingly, the authors also reported that the higher rate of ICU admission was not associated with significant changes in ICU mortality for patients with an acute respiratory infection; rates were 19.7%±3.0%, 24.0%±3.6% and 25.0%±4.0% for the 75–79, 80–84 and 85–89 age groups, respectively. Indeed, the authors reported a significant drop in ICU mortality from 41% in 2006 to 22% in 2015 (p=0.03) for patients aged ≥90 years. Hospitalisations for CAP and acute exacerbations of COPD increased significantly for all age groups over the 10-year study period.
Meanwhile, a multicentre, prospective study from Canada [68] including 1671 critically ill very old patients who were admitted to 22 ICUs, reported that ICU mortality was 22%, with a median time from ICU admission to death of 10 days. 49% of patients who died were still receiving mechanical ventilation, vasopressors or dialysis.
A retrospective cohort analysis including 328 404 elderly (>64 years) patients with pneumonia admitted to ICUs in the USA [69] found potential benefit provided by ICU admission for older patients with low-risk pneumonia. Compared to patients admitted to a general hospital ward, patients admitted to an ICU had significantly lower adjusted 30-day mortality (15% versus 21, p=0.02) with no significant differences in health costs associated with ICU admission.
A study by Chen et al. [70] evaluated the performance of two scores (PSI and CURB65) in three groups of CAP patients according to age: 18–64 years, 65–84 years and ≥85 years. The authors found the worst scores, mainly the PSI, in the group of patients aged 65–84 years and ≥85 years. This may be due to an overestimated weight of age. The authors therefore proposed a modified score excluding age for this specific population.
Recently, Sanz et al. [71] proposed a composite score to predict mortality by combining PSI score and Barthel index. In a study that included 1919 patients aged ≥65 years, 61% had severe pneumonia (PSI IV–V) and 40% had Barthel index ≤90. The combination of PSI IV–V and Barthel index ≤90 constituted the greatest risk factor for mortality (OR 4.17).
Among the scores that predict ICU admission, the need for vasoactive drugs, or the need for mechanical ventilation, the most commonly used are the SMART-COP tool [72], and the American Thoracic Society (ATS)/Infectious Disease Society of America (IDSA) severity criteria score [73]. Age or comorbidities are not included in the ATS/IDSA criteria since patient selection is based on acute physiologic parameters. In the SMART-COP, the cut-off for age is 50 years.
Recently, de Lange et al. [74] proposed a Cumulative Prognostic Score (CPS) to predict 30-day mortality in very old patients admitted to an ICU. Overall, 306 ICUs from 24 European countries participated in the study; 3730 very old patients with a median age of 84 years were included. The 30-day mortality rate was 42% (1562 deaths), with age, sex, ICU admission diagnosis, CFS, Sequential Organ Failure Assessment, invasive mechanical ventilation and renal replacement therapy being predictors for mortality. The area under the curve for a CPS of ≥10 points was 0.80. The model predicted 30-day mortality in 91% of all patients who died at a cut-off point of ≥10 (75% of all patients). Although CPS seems to be a useful tool to guide physicians, several factors relevant to very old patient populations (e.g. nutritional status, functional status, dementia and comorbidities) have not been incorporated into the score.
In conclusion, clinical evaluation is the cornerstone when considering ICU admission of very old patients. Age should not be the only factor guiding ICU admission. Delayed ICU admission is associated with a higher risk of death. Patients who may benefit from ICU admission are those who have failed to benefit from therapy during general hospitalisation, and patients requiring organ support or specific monitoring [75, 76].
What is the importance of intermediate care in critically ill very old patients?
In a study from 2014 including data from 167 ICUs in 17 European countries, Capuzzo et al. [77] evaluated whether adults admitted to hospitals with both ICUs and intermediate care units (IMCUs) had lower in-hospital mortality than patients with no IMCU option. The study included 5834 patients: 1397 (24%) died in the hospital and 19% in the ICU. Overall, 5031 (86%) patients were admitted to hospitals with IMCUs and 803 (14%) to those without IMCUs. After adjustments for patient characteristics (illness severity, ICU) and hospital characteristics (number of hospital beds, ICU beds, teaching hospital, for-profit hospital, possibility of extra beds in the ICU, patient ratio in daytime for ICU nurses), the authors reported that the presence of an IMCU in the hospital significantly reduced mortality for adult patients (OR 0.63 (95% CI 0.45–0.88); p=0.007) compared to centres without IMCUs.
Few prospective studies compared mortality in IMCUs and ICUs in very old patients with CAP. IMCUs require less human and technical resources, thus potentially providing a practical alternative for critically ill very old patients who do not require invasive procedures and whose ICU admission is questionable in terms of benefit. IMCUs offer the option of stepping up to ICU care or stepping down to general hospitalisation [78]. Notwithstanding this, evidence supporting the use of IMCUs in critically ill very old patients is scanty and further studies are needed in order to provide specific recommendations for the use of intermediate care in these patients.
Is microbial aetiology in very old patients different from that of the general population?
Overall, CAP causative agents in the elderly differ from those of other age groups because of a higher rate of pneumococcal and influenza infections as well as a lower rate of atypical microorganisms [79].
In 2003, the study by Fernandez-Sabe et al. [80] that investigated the aetiology and outcomes of CAP in very old patients, reported that S. pneumoniae was the main pathogen that caused CAP in very old patients. Legionella and atypical microorganism were very rarely found in very old patients with CAP.
In 2013, a study by our research group, investigated the effect of age and comorbidities on the microbial aetiology of CAP [44]. Our results showed that microbiological diagnosis in CAP decreased with each increasing age group (65–74 years: 43.7%; 75–84 years: 40.7%; and ≥85 years: 31.4% (p<0.001)), and age did not influence microbial aetiology by itself. S. pneumoniae was the pathogen most frequently reported in all age groups (40.7%, 39.4% and 48.9%, respectively), followed by mixed aetiology (16.0%, 13.1% and 10.6%, respectively), atypical pathogens (16.0%, 13.1% and 9.9%, respectively) and respiratory viruses (8.4%, 14.6% and 11.3%, respectively). In patients with at least one comorbidity Haemophilus influenzae was the most common pathogen; multidrug-resistant (MDR) pathogens were frequent in patients with one or more comorbidities. Gross et al. [81] found that independent predictors of MDR pathogens in CAP were similar to those identified for other infections (i.e. Pseudomonas aeruginosa) colonisation/infection in the previous year, antimicrobial use in the previous 90 days, admission from a nursing home and duration of hospitalisation in the previous 90 or 180 days.
In 2015, another Spanish study [82] proposed the acronym PES for a group of pathogens (P. aeruginosa, Enterobacteriaceae extended-spectrum β-lactamase positive (ESBL+) and methicillin-resistant Staphylococcus aureus (MRSA)) that cause CAP in approximately 6% of cases with a microbiological diagnosis. The authors proposed the “PES score” to identify patients at higher risk of CAP caused by PES. However, the PES score (table 1) lacks a specific age threshold for very old patients and this and other scores need further validation before being systematically recommended in the assessment of MDR microorganisms in CAP occurring in very old patients.
Pseudomonas aeruginosa, extended-spectrum β-lactamase-positive Enterobacteriaceae and methicillin-resistant Staphylococcus aureus (PES) score
More recently, a study from China [83] evaluated the impact of adherence to current antimicrobial guidelines on the mortality of 3131 hospitalised elderly CAP patients. The authors reported that the rate of patients admitted to ICUs increased by age group: 6% in the age group 65–74 years; 9% in the age group 75–84 years; and 14% in the age group >85 years. Microbial aetiology was defined in 14% of patients. P. aeruginosa was the most common pathogen (20%), followed by Klebsiella pneumoniae (15%), respiratory viruses (14%), Escherichia coli (10%), Acinetobacter spp., (8%), S. aureus (7%), S. pneumoniae (3%) and atypical pathogens (0.6%).
Ferrer et al. [84] analysed prognostic factors for severe CAP in 664 immunocompetent patients, 154 (23%) of whom were ventilated and 510 (77%) who were non-ventilated; the mean age was 72 years in the nonventilated group and 66 in the ventilated group. Microbial aetiology was established in 51% of patients. S. pneumoniae was the main pathogen in both groups, polymicrobial aetiology was more frequent in patients invasively ventilated and Legionella pneumophila was less frequent.
In a recent study about sepsis in very old patients with CAP, we observed that an aetiologic diagnosis was achieved more often in very old patients with sepsis compared to very old patients without sepsis (34% versus 27%; p=0.01) [26]. Although these data were not published, we found that the microbial aetiology was similar in very old patients admitted to general wards and those admitted to ICU. S. pneumoniae was the most frequent pathogen detected in both groups (43% versus 53%, p=0.094). Interestingly, polymicrobial aetiology was the second most frequent aetiology in very old patients admitted to ICU (10% versus 12%, p=0.44), whereas respiratory viruses were the second more frequent aetiology in very old patients hospitalised in general wards (18% versus 9%, p=0.0043).
An international study [85] recently found that risk factors independently associated with CAP due to Enterobacteriaceae were male sex, severe CAP, underweight (body mass index <18.5 kg·m−2) and previous ESBL infection. In addition, previous ESBL infection, being underweight, cardiovascular diseases and hospitalisation in the last 12 months were independently associated with MDR Enterobacteriaceae CAP.
In addition to MDR pathogens, microorganisms associated with aspiration pneumonia should be taken into account when approaching microbiologic diagnosis of CAP in very old patients. Aspiration pneumonia, frailty and dementia are tightly intertwined. Findings of pathogens potentially associated with aspiration in CAP occurring in the elderly widely vary and are probably underestimated overall [86].
In brief, CAP in very old patients is caused by the same microorganisms than other age groups. However, increasing age is a risk factor for Enterobacteriaceae and MDR pathogens. Other risk factors for MDR CAP, such as residence in nursing homes, previous colonisation or use of antibiotics, as well as the risk of aspiration pneumonia due to swallowing difficulties should be carefully assessed before instauration of empirical treatment and for deciding preventive contact isolation at admission among other measures. Risk scores, such as PES score, might be of utility but are not adapted to the very old patient population.
Principles for guiding empiric antimicrobial therapy of CAP in very old patients
Antibiotic therapy in critically ill very old patients should take into account age-related changes in the tolerance, metabolism and excretion of antimicrobials, as well as drug–drug interactions [87].
Current international guidelines for the management of CAP patients [4, 88] do not provide a specific recommendation for critically ill very old patients. Table 2 summarises the antibiotic therapy recommended in patients with CAP requiring ICU admission.
Guidelines for the management and treatment for community-acquired pneumonia
As stated, the risk of aspiration should be assessed to decide whether an anaerobicidal agent might be included and risk factors for MRSA, P. aeruginosa and other Gram-negative bacilli should also be assessed when selecting antibiotic treatment. Furthermore, apart from the recommendations included in current guidelines, there are other options that might be advantageous for treating CAP in critically ill very old patients. For instance, new generation cephalosporines might play an important role in this setting. Ceftaroline is a fifth-generation cephalosporine. Compared to ceftriaxone, it provides better coverage against S. pneumoniae and S. aureus (both MRSA and methicillin-sensitive Staphylococcus aureus) in patients with CAP. Results from the Focus studies [89, 90] and the CAPTURE study [91] demonstrated its efficacy in older patients with CAP caused by one of these microorganisms. Ceftobiprole is also a new cephalosporin active against S. pneumoniae, S. aureus (MRSA and methicillin-sensitive Staphylococcus aureus) and a substantial proportion of P. aeruginosa. It is indicated in CAP [92] and hospital-acquired pneumonia but not ventilator-associated pneumonia. Ceftobiprole may be a reasonable option to cover P. aeruginosa in addition to S. pneumoniae and S. aureus. None of these cephalosporines is effective against ESBL Enterobacteriaceae.
There are other new antibiotics in the pipeline that due to their pharmacokinetic/pharmacodynamic properties, spectrum or tolerability might end up being added to the armamentarium for treating CAP in very old patients. Amalakuhan et al. [93] analysed solithromycin, pristinamycin, nemonoxacin, lefamulin, omadacycline, ceftobiprole and delafloxacin by applying to them the San Antonio NIPS Model (N: novelty of mechanism; I: avoidance of interactions and intolerance; P: favourable pharmacokinetic/pharmacodynamic profile; S: simplicity of dosing). Nemonoxacin and delafloxacin both had a high NIPS index.
Corticosteroids as adjunctive therapy
A randomised study that investigated the effect of corticosteroids on treatment failure among patients with severe CAP (according to ATS/IDSA criteria) with high inflammatory response (initial levels of CRP>15 mg·dL−1) reported that treatment failure was less frequent in patients in the corticosteroid group (13%) compared to patients in the placebo group (31%; p=0.02) and in-hospital mortality was similar between groups (10% versus 15%; p=0.37) [94].
Several studies and meta-analyses have shown a reduction in the risk of progression to respiratory distress, a shorter time to clinical stability and a shorter duration of hospital stay in patients with severe CAP receiving adjunctive therapy with corticosteroids [95–97]. The latest ATS/IDSA guidelines do not routinely recommend the use of corticosteroids in adults with severe CAP (conditional recommendation, moderate quality of evidence). However, corticosteroids are suggested in CAP patients with refractory septic shock [4]. Nonetheless, there is no specific evidence available on the use of adjunctive corticosteroids in very old patients with CAP.
Sepsis as a complication in critically ill very old patients with CAP
A 2012 study assessing the impact on outcome of severe sepsis in which the most frequent site of infection was the lung (46%) showed large differences in ICU mortality by age group (46%, 61% and 79% for <60 years, 60–80 years and very old patients, respectively). Moreover, age was the only variable independently associated with ICU mortality in the multivariate analysis (OR 1.038) [98].
A recent prospective multicentre study including 1490 patients from 77 ICUs in Spain investigated mortality risk factors in critically ill elderly (65–79 years) and very old patients with sepsis. The overall hospital mortality was 49% (n=727) and was significantly higher in very old patients compared to elderly patients (54% versus 47%; p=0.02). Predictors of hospital mortality in very old patients with sepsis were age, APACHE II score and prompt adherence to the resuscitation bundles. In 2016, Montull et al. [46] identified severe sepsis in 37% of 4070 CAP patients. The authors reported that severe sepsis CAP was independently associated with older age, alcohol abuse, COPD and renal disease, whereas previous antibiotic therapy was a protective factor. In another Spanish cohort study [26] that included 1238 very old patients with CAP, 71% presented with sepsis according to the Sepsis-3 definition. Male sex, chronic renal disease and diabetes mellitus were independent sepsis risk factors, while antibiotic therapy before admission was independently associated with a lower risk of sepsis. The authors also reported that in-hospital mortality was significantly higher in very old patients with sepsis than in nonseptic patients (15% versus 9%, p=0.006).
More recently, Cillóniz et al. [99] investigated pure viral sepsis in CAP patients and reported that viral sepsis, defined according to the Sepsis-3 criteria, affected 19% of patients with a diagnosis of viral pneumonia admitted to ICUs. Interestingly, male sex and age ≥65years were risk factors for pure viral sepsis; however, pure viral sepsis was not a risk factor for in-hospital mortality. In this study 9% of patients were critically ill very old patients and viral sepsis was present in 11% (data not published).
Critically ill very old patients presenting with CAP and sepsis must be quickly identified: the atypical presentation of pneumonia and sepsis in this subgroup of patients may alert physicians in order to reduce the complications associated with a delay in the start of the empiric antimicrobial therapy.
What is the relationship between hospital discharge and readmission?
The rate of 30-day readmission in very old patients varies from 8–27% [48, 100–102]. Unfortunately, there is limited information about readmission rates in critically ill very old patients with CAP. Readmission is related to preventable and nonpreventable factors. Two studies reported data on preventable factors, although were not specific for critically ill very old patients. In 2017, Dong et al. [100] investigated 2892 CAP patients, 15% of whom were readmitted; 40% were ≥65 years and 33% of them were readmitted. In this group of patients, the distribution of discharge was as follows: home without services (43%); home with healthcare (26%); skilled nursing or subacute rehabilitation facility (16%); and acute rehabilitation or long-term acute care facility (15%). 20% of patients discharged with healthcare and 12% of patients discharged without home services were readmitted. Surprisingly, being discharged with healthcare was associated with a markedly greater risk of readmission in the multivariate regression model (OR 1.58, 95% CI 1.21–2.07). Interestingly, in 2015, Flaatten et al. [68] reported that among 1671 critically ill very old patients, 20% were discharged to a long-term care facility, 46% went home and 3% went to a rehabilitation facility. Unfortunately, the authors did not report the rate of readmission.
Toledo et al. [48] included 1756 patients with CAP, whose readmission rates were 28%, 49% and 23%, for age groups 65–74 years, 75–84 years and >84 years, respectively. The overall rate of readmission among ICU patients was 6%; however, percentages by age group were not reported. In the multivariate analysis of factors related to readmission, the only preventable factor was discharge with home healthcare (OR 5.61, 95% CI 1.70–18.50). The authors suggested an inadequate evaluation of patient stability at the time of hospital discharge as a possible explanation.
Overall, these data reflect the importance of discharge disposition as a factor related to readmission in critically ill very old patients with CAP, as well as the need to systematically report these variables in clinical studies.
Long-term outcomes in critically ill very old patients with CAP
During the past decade, several studies reported data about long-term consequences of CAP [103–111]. Major adverse cardiac events have been described during pneumonia hospitalisation and up to 10 years after an episode of CAP, with a prevalence ranging between 10% and 30%, especially in case of pneumococcal pneumonia, elderly patients and severe pneumonia [109, 112–117]. New-onset or worsening heart failure, arrhythmias, stroke and acute coronary syndrome can be an expression of major adverse cardiac events in CAP patients. In a non-human primate model of severe pneumococcal pneumonia, Reyes et al. [112] showed that Pneumococcus invaded the myocardium and induced cardiac injury with necroptosis and apoptosis, followed by cardiac scarring after antibiotic therapy. Corrales-Medina et al. [114] investigated the risk of heart failure after hospitalisation for CAP in elderly patients (median age 77 years). The authors reported that the rate of new-onset heart failure increased following hospital discharge: 30–90 days: 3%; 91 days to 6 months: 6%; 6 months to 1 year: 9%; 1–5 years: 20%; and >5 years from hospital discharge: 31%.
Heyland et al. [118] evaluated 12-month outcomes in critically ill very old patients after ICU discharge. The study included 610 critically ill very old patients admitted to ICU for at least 24 h. ICU, hospital and 12 months after ICU admission mortality were 14%, 26% and 44%, respectively. 75% of critically ill very old patients admitted to ICU survived and returned to their basic levels of physical function at 1 year.
The study by Ferrante et al. [119] evaluated the relationship between frailty and post-ICU disability in 266 elderly and very old patients (mean age 84 years) admitted to ICU. The authors reported that frailty, prefrailty and nonfrailty were present in 45%, 43% and 12% of patients, respectively. In the multivariable analysis, frailty was associated with 41% greater disability over the 6 months following a critical illness compared to nonfrailty, whereas prefrailty conferred a 28% greater risk of post-ICU disability compared to nonfrailty. Mortality 6 months after ICU admission was twice as high among participants with frailty (55%) compared to those who were prefrail (25%) or nonfrail (26%).
Advanced age is known to be associated with high-risk of long-term mortality. In 2011, Roch et al. [20] evaluated factors influencing short- and long-term outcomes in 299 critically ill very old patients following ICU admission. The authors reported 46% of ICU mortality and 55% of hospital mortality. A higher SAPS II score at ICU admission, the existence of a fatal disease (as reflected by the McCabe score), and a cardiac diagnosis at admission were associated with hospital mortality. 1- and 2-year mortality rates were 72% and 79%, respectively.
A French study of 317 critically ill very old patients reported that 6-month and 1-year mortality after discharge were 56% and 70%, respectively [17]. Another study from Germany, including 372 critically ill very old patients [120], reported that in the overall population 3 months and 1 year after discharge survival was 53% and 35%, respectively. In patients aged ≥65 years with CAP, mortality at 6 months was reported to be 19% and mortality at 1 year was 41% [107, 121]. In a study published by our research group [26] we reported 22% of 1-year mortality in very old patients with sepsis secondary to CAP.
Vaccination and other prevention measures for CAP in very old patients
Current international guidelines recommend specific measures for preventing CAP [4, 73, 88, 122]. The use of pneumococcal vaccines (polysaccharide and conjugate) and influenza vaccines are the most important of these. Intervention in the lifestyle for modifiable risk factors for CAP will also help to reduce the risk of pneumonia in very old patients [123]. Figure 4 summarises the main prevention measures for CAP.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevention of community-acquired pneumonia.
Conclusion
The burden of CAP among critically ill very old patients is high, encompassing significant morbidity, mortality and health costs worldwide. The presence of multiple comorbidities, polypharmacy and frailty characterises these patients and increases the risk of infectious diseases, such as pneumonia. Early recognition and diagnosis of CAP and its complications, such as sepsis, allows for the prompt initiation of the antibiotic therapy. However, due to its atypical presentation in very old patients, the diagnosis of pneumonia may be difficult in some cases. Preventive interventions are of pivotal importance to improve outcomes and reduce the occurrence of adverse consequences.
Footnotes
This article has an editorial commentary: https://doi.org/16000617.0031-2020
Provenance: Submitted article, peer reviewed.
Author contributions: C. Cillóniz, C. Dominedò, J.M. Pericàs, D. Rodriguez-Hurtado and A. Torres conceived this review, provided their expertise for it, wrote the draft manuscript and contributed to its revision. All authors have read and approved the final manuscript.
Conflict of interest: C. Cillóniz has nothing to disclose.
Conflict of interest: C. Dominedò has nothing to disclose.
Conflict of interest: J.M. Pericàs has nothing to disclose.
Conflict of interest: D. Rodriguez-Hurtado has nothing to disclose.
Conflict of interest: A. Torres has nothing to disclose.
Support statement: Publication was funded by Ciber de Enfermedades Respiratorias (CibeRes CB06/06/0028) and the 2009 Support to Research Groups in Catalonia 911, IDIBAPS (CERCA Programme/Generalitat de Catalunya). C. Cillóniz is the recipient of a postdoctoral grant (Strategic Plan for Research and Innovation in Health-PERIS 2016–2020), SEPAR fellowship 2008 and the Fondo de Investigación Sanitaria (grant PI19/00207). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received September 24, 2019.
- Accepted November 1, 2019.
- Copyright ©ERS 2020.
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- What is the role of community-acquired pneumonia in critically ill very old patients?
- Clinical presentation of pneumonia in very old patients
- What parameters might help guide the management of CAP in critically ill very old patients?
- ICU benefit in very old patients: role of severity scores
- What is the importance of intermediate care in critically ill very old patients?
- Is microbial aetiology in very old patients different from that of the general population?
- Principles for guiding empiric antimicrobial therapy of CAP in very old patients
- Corticosteroids as adjunctive therapy
- Sepsis as a complication in critically ill very old patients with CAP
- What is the relationship between hospital discharge and readmission?
- Long-term outcomes in critically ill very old patients with CAP
- Vaccination and other prevention measures for CAP in very old patients
- Conclusion
- Footnotes
- References
- Figures & Data
- Info & Metrics