





Abstract
Asthma remains an important disease worldwide, causing high burden to patients and healthcare systems and presenting a need for better management and ultimately prevention and cure. Asthma is a very heterogeneous condition, with many different pathophysiological processes. Better measurement of those pathophysiological processes are needed to better phenotype disease, and to go beyond the current, highly limited measurements that are currently used: spirometry and symptoms. Sophisticated three-dimensional lung imaging using computed tomography and ventilation imaging (single photon emission computed tomography and positron emission tomography) and magnetic resonance imaging and methods of lung imaging applicable to asthma research are now highly developed. The body of current evidence suggests that abnormalities in structure and ventilatory function measured by imaging are clinically relevant, given their associations with disease severity, exacerbation risk and airflow obstruction. Therefore, lung imaging is ready for more widespread use in clinical trials and to become part of routine clinical assessment of asthma.
Abstract
“A picture says a thousand words”: three-dimensional imaging has shown the varied and complex nature of the derangement in structure and function in asthma. As such, imaging is crucial to developing new asthma treatments and improving asthma management. http://ow.ly/KEqH30nY4Yc
Introduction
Asthma remains a big challenge to the international research and clinical community. We still don't know what causes asthma; we cannot cure it; we do not understand fully the basis of treatment response; and some asthma sufferers still die of their condition. Asthma treatment has improved markedly in the past 10–20 years, which is based on greater appreciation of the importance of inhaled corticosteroids as the basis of asthma treatment, particularly when combined with a long-acting β-agonist. The main “breakthroughs” in asthma management have been based on these two drug types. The more recent breakthrough studies involve targeted anti-inflammatory treatments. These include monoclonal antibodies directed against specific molecules in the allergic inflammatory pathways [1–4], as well as macrolide antibiotics in treatment-resistant asthma [5]. However, prevention and cure of asthma require an understanding of the causes of asthma, which remain obscure.
Another challenge to researchers is understanding the diversity of the condition called asthma. It is commonly described as a heterogeneous disorder, or alternatively a collection of separate conditions which lead to a common clinical picture. The heterogeneity of pathophysiology and clinical expression is becoming increasingly important in the era of “precision” or “personalised” medicine, where there is now strong evidence that treatment should not be a “one size fits all” approach [6–8]. The concept of “treatable traits” is increasingly recognised as an approach to managing airways disease that potentially leads to large clinical benefits, including improving asthma control [9]. Currently, we recognise several inflammatory phenotypes that are predictive of response to inhaled corticosteroids [10–12] and monoclonal antibody treatment against IgE [13] and interleukin-5 [14]. In addition, asthma severity varies widely, from episodic disease to persistent, steroid-unresponsive symptoms; recurrent exacerbations that may be fatal; and some patients suffer accelerated loss of forced expiratory volume in 1 s (FEV1). Inflammation is important, but is not the sole important process in asthma. Remodelling of the lung parenchyma [15–18] and airways [19] is a fundamental process, but it is challenging to measure. Imaging of both lung and airway structure as well as ventilation can potentially provide a means to measure change and to examine the clinical significance of these structural changes.
Asthma is thought of as an inflammatory condition, with chronic inflammation driving airway remodelling and causing intermittent airway narrowing due to the release of bronchoconstrictive chemicals such as histamine, leukotrienes and prostaglandins. However, the underlying mechanism of airway hyperresponsiveness in asthma is likely to be a complex interaction between factors that drive remodelling and inflammation, and, potentially, other pathways that remain undiscovered [20, 21]. This would reflect the clinical heterogeneity that is currently increasingly well recognised in asthma. It is important to assess the type II high inflammatory phenotype in asthma, since this represents a treatment target for corticosteroids and for targeted therapies, e.g. biologics and anti-prostaglandins [22]. Apart from the type II high phenotype, the pauci-granulocytic and neutrophilic inflammatory phenotypes are less likely to respond to corticosteroid treatment, and addressing corticosteroid nonresponsiveness in type II low phenotypes remains a major clinical and research problem.
As clearly described in the recent Lancet commission on asthma [23], we still have much to do to understand and treat asthma better (although targeted monoclonal antibody treatment has been a breakthrough in severe, eosinophilic asthma) and we (clinicians and researchers) may need to dramatically change the way that we think about and understand asthma. The idea of asthma as a single entity is changing rapidly. The authors state that we need to develop new drugs, use better biomarkers to predict disease progression and treatment response and classify airways diseases differently in future research. We argue that imaging forms a crucial part of that call for a new way of thinking of airways disease, of new diagnostic labelling and classification, and hence better research towards prevention, cure and disease modification.
There has been a large increase in imaging research in asthma in the past decade, which takes advantage of rapidly improving imaging methods and computing power, which is necessary to process the large volume of data associated with imaging. Imaging of the lung is currently exclusively three-dimensional and includes methods such as high-resolution computed tomography (HRCT), single photon emission computed tomography (SPECT), positron emission tomography (PET), ventilation magnetic resonance imaging (MRI) and ultrahigh resolution techniques such as micro-computed tomography and synchrotron imaging. In addition, there are invasive techniques such as optical coherence tomography. This review describes the authors' viewpoints on the information gained from imaging in asthma, which has led to the current understanding of the pathophysiology of asthma and its potential use in future research and as a biomarker. Each of the many techniques has its own characteristics and hence can provide its own unique information about the lungs and airways (table 1). HRCT scanning predominantly provides measurements of airway and lung structure, as well as small airway function from the difference between inspiratory and expiratory images. Imaging using SPECT, PET and MRI provide information on the distribution of ventilation. There is a large body of imaging work in asthma, which demonstrates dramatic derangements in structure and function. However, there is still much research needed to bring imaging into use in clinical trials and clinical practice.
Characteristics of computed tomography (CT) and three-dimensional ventilation imaging
The physiological information derived from imaging will complement what is contained in spirometry, rather than demonstrating strong correlations to it. Hence, imaging data will potentially characterise patients, to show differences in responses to new and current treatments, prognosis, loss of lung function and other clinically important outcomes beyond what we currently know and how we use type II high biomarkers in clinical practice [24]. For example, ventilation patterns may provide mechanistic insights into treatment responsiveness regardless of inflammatory phenotype; this may be particularly relevant in type II low disease where strategies such as macrolides [5], high fine particle fraction aerosols [25] and bronchial thermoplasty [26–28] are used. What is still needed in imaging research is, primarily, better quantification of structure and function, for example better defining ventilation and ventilation defect patterns, or distributions of wall thickness on CT. With better measurement outcomes, longitudinal studies to determine clinical correlates will be more meaningful.
How do we understand asthma better from CT imaging?
Computed tomography has provided mainly structural information on the lungs and airways in asthma, while other expiratory CT studies have provided functional data on small airways function that have confirmed their importance in pathophysiology. Whole-body CT scans provide imaging down to the small conducting airways (∼1 mm internal diameter; approximate generations 6–8). The ability to see airways clearly is based on the contrast difference between airway and soft tissue, and, unsurprisingly, the accuracy of airway measurements decreases with decreasing airway size [29].
CT image resolution is most limited in the z-direction, i.e. longitudinal axis. Modern high-resolution scans often use the “helical” or “spiral” mode (they are synonymous terms) [30]. During helical or spiral mode scanning, the X-ray tube rotates while the patient is moved through the tube, hence any single image capture element (X-ray detector) effectively makes a helical motion along the chest wall. The advantage is speed, which allows imaging the entire lung in “one hit” and during a single breath-hold. Hence, the anatomical localisation of all structures in the chest, in the resultant three-dimensional image is accurate (no misregistration). The disadvantage is loss of information: reduced resolution, depending on how fast the subject is moved through the scanner (pitch).
Conventional or axial HRCT is performed using a static subject. A single image is taken; the thickness being determined by the “width” of the detector array, typically ≥64 in modern scanners. However, the z-axis coverage of the detectors is still not enough to cover the length of the lung. To image the lung in toto, the subject is moved to the next position and the next image is taken. The images must then be “joined” to create a single, three-dimensional image of the lungs, which may lead to registration errors (overlap, subject movement, etc.).
Airway wall thickness measurements tend to be overestimated in CT images due to multiple factors, including the blurring discussed earlier [29, 31, 32]. Nevertheless, a landmark study by Nakano et al. [31] showed that dimensions measured in multiple airways relate sufficiently strongly to small airway dimensions measured histologically, to allow estimation of small airway wall dimensions. The index Pi10 is an interpolated measurement of airway wall thickness, calculated for an airway of internal perimeter 10 mm. This validation was done in explanted lungs of smokers, and whether the relationship between medium-sized airway dimensions measurable on CT also relates to the small airways dimensions in asthma has never been proven.
Increased airway wall thickness measured using CT is consistent with histological studies of explanted asthmatic lungs. Furthermore, wall thickness measurements from CT scans have been correlated with endobronchial biopsy measurements of remodelling [19, 33]. That increased airway wall thickness is correlated with asthma severity and lung function impairment has significant implications in terms of the pathophysiology of asthma. Thicker airway walls are associated with lower FEV1 [34–37] and increased risk of asthma exacerbations [38–40]. However, airway walls may appear thicker on CT due to increased airway smooth muscle and matrix, i.e. structural remodelling [33], as well as oedema, inflammatory cell infiltration, increased mucus and bronchial perfusion due to acute inflammation, which is probably the case in asthma exacerbations. However, mucus in airways may be occlusive and their measurement in CT correlates with spirometric airflow obstruction, suggesting that this is a mechanism and target for treating airflow obstruction in asthma [41].
Theoretically, thickening of airway walls should alter their mechanical properties, which may explain airway narrowing and airway hyperresponsiveness in asthma. However, the nature of the mechanical alteration is uncertain. An increase in airway smooth muscle, matrix proteins, fibrin and collagen might make airways stiffer, which means that they would not stretch and dilate as much during a deep breath; therefore, airway resistance at high lung volume would increase and FEV1 would decrease. Even small degrees of airway wall thickening that reduced the airway lumen could potentially have a large effect on resistance due to the fact that airway resistance is inversely proportional to the fourth power of lumen radius. Furthermore, airway wall thickening dramatically magnifies the effects of airway smooth muscle contraction [42]. Therefore, this model of airway narrowing to explain airway narrowing and airway hyperresponsiveness in asthma has a strong theoretical basis [43] and makes intuitive sense.
The evidence that airway wall thickening at least partly explains spirometric impairment in asthma (as mentioned earlier) is strong, whereas there is almost no experimental support for airway wall thickening as an explanation for airway hyperresponsiveness. Boulet et al. [44] reported an association between airway wall thickening and airway hyperresponsiveness, but only in subjects who had airflow obstruction on spirometry, not in the group that had normal spirometry. In contrast, Niimi et al. [35] reported that increased airway wall thickness was negatively associated with airway hyperresponsiveness, which contradicted predictions that thickening would increase airway narrowing [42, 43]. They suggested that thicker walls would be more resistant to collapse, thereby offering protection against excessive airway narrowing and airway hyperresponsiveness. Therefore, the mechanistic and pathophysiological significance of wall thickening in asthma remains poorly understood. Perhaps the distribution of remodelling seen on CT may be relevant, although this would be difficult to quantify using objective techniques and there are very few published data. Clinical differences were reported from one study in which the distribution of airway wall thickening was assessed subjectively [45].
Bronchial thermoplasty has become established as a potential therapy for severe treatment-resistant asthma. Treatment has been associated with reduced airway smooth muscle mass and reticular basement membrane thickness [46, 47], and this has been confirmed by CT scans taken before and after treatment, where airway wall thickness was less after treatment [28]. There was a reduction in CT-measured gas trapping as well [28], which was consistent with that observed from a lung function study [48]. Gas trapping occurs due to severe narrowing and closure of the small airways and along with an observation that airway smooth muscle mass was reduced in the untreated (in most) middle lobe [47], it is possible that the effects of thermal insult are more widespread than in the treated areas in large airways and may become extensive, affecting most of the tracheobronchial tree. At present, there is very little to guide clinicians as to which patients should be put forward for bronchial thermoplasty. Objective measurements will probably be useful; these may include imaging alone or in combination with lung function measurements of remodelling, bronchodilator responsiveness, airway hyperreactivity, variability of function and airway or lung mechanics.
Although most of the CT research in asthma is focused on airways, there is a small amount of literature on changes in the lung parenchyma in asthma. There is a significant body of evidence that suggests that a large part of the obstructive impairment is due to the lung parenchyma. The reasoning behind this is that the lung parenchyma exerts a distending force on the airways, so that a reduction in elasticity would result in reduced airway calibre. That is, that the same mechanisms that cause airway narrowing in chronic obstructive pulmonary disease (COPD) probably also act in asthma.
Lung density on CT imaging at full lung inflation (i.e. at total lung capacity), reflects alveolar size and elasticity. Hence, lung density is reduced in emphysema, which reflects the lung being “overdistended” in emphysema because of the characteristic reduction in lung elastic recoil. Conversely, lungs are “underdistended” in lung fibrosis due to an increase in lung elastic recoil, i.e. decreased lung compliance. Multiple CT studies in asthmatics have shown that lung density is reduced, indicating increased lung tissue distensibility and compliance [15, 16, 18]. The physiological consequence of this is that airways will be narrowed at any given lung volume due to a reduction in radial distending forces from the lung. Airway walls will also appear thicker when airways are narrowed, since wall thickness is expressed relative to airway calibre, i.e. not all of the measured wall thickening measured by CT is due to remodelling. The increase in lung distensibility and loss of recoil have been confirmed in physiological studies [17, 49] and in histological studies of post mortem lungs from asthmatic individuals [16]. The mechanisms and causes of this altered lung structure are unknown, but if loss of lung function is to be successfully treated, then investigation of causes of lung tissue remodelling has to occur. There has been some progress in understanding the mechanisms of airway wall remodelling, but almost nothing on the lung tissue. Arguably, the problem of loss of lung function cannot be addressed without extensive study of the causes of structural change in both airways and lungs together.
The upper airway, including the nose and paranasal sinuses, is important both clinically and mechanistically in asthma. The “united airway” hypothesis is that common mechanisms link rhinosinusitis and asthma. It has been reviewed frequently, but there have been few advances in understanding the mechanisms of the associations between rhinosinusitis and asthma. Nevertheless, it needs to be considered in research on asthma mechanisms, when developing new treatment and when managing asthma patients [50–53]. Rhinosinusitis is highly prevalent in asthmatic subjects and vice versa. Between 30% and 80% of asthmatic subjects have allergic rhinitis and 20–40% of allergic rhinitis sufferers have asthma, and there are similar inflammatory processes occurring in the nose, paranasal sinuses and airways of asthmatic subjects [51, 54]. Sinusitis seen on CT is associated with aspirin sensitivity [55] and increased blood markers of inflammation and poorer lung function [56]. CT imaging is a highly sensitive way to detect sinus disease, showing mucosal thickening of the sinuses, with worse sinus disease being associated with more severe asthma [57]. Nasal polyposis is also associated with severe allergic asthma, and in a retrospective analysis of the mepolizumab registration studies, nasal polyposis was also associated with eosinophilic inflammation and reduced acute bronchodilator reversibility [58]. However, nasal polyposis did not influence response to mepolizumab treatment. Future studies of the clinical relevance of nasal and sinus disease in asthma and severe asthma are needed, particularly the use of biological treatments for severe asthma.
Understanding asthma from functional CT imaging studies
Changes in ventilation distribution are a fundamental characteristic of many lung diseases, including asthma. Ventilation distribution measured using complex lung function tests, such as inert gas washout, has been shown to be highly heterogeneous [59, 60]; that is, some parts of the lung function well, while other parts function poorly, making ventilation highly variable within a lung. This concept is referred to as ventilation heterogeneity or ventilation inhomogeneity (synonymous terms) and has been shown to be strongly correlated with airway hyperresponsiveness [59], asthma symptoms [61], medication requirements [62] and asthma severity [63]. Ventilation imaging complements these lung function tests of ventilation distribution, by providing information on three-dimensional location and organisation. However, much of the clinical and physiological significance of parameters that quantify three-dimensional ventilation still needs to be determined.
CT scanning has been used to measure the distribution of ventilation by sophisticated image processing techniques including parametric response mapping (PRM) [64]. This method takes two CT images, one at full lung inflation and the other at lower volume (residual volume or functional residual capacity). Using deformable registration techniques, i.e. morphing the lung structures, inferences can be made on changes in regional lung volume between the two CT volumes, from which regional ventilation can be estimated. Furthermore, this also (reasonably) assumes that the site of flow limitation is in the small airways, and by implication, alterations and regional ventilation determined by PRM reflect abnormalities and regional function of the small airways. Clearly, there are many assumptions in interpreting the final results in this way. Although many studies using PRM have been performed in COPD, there are none in asthma.
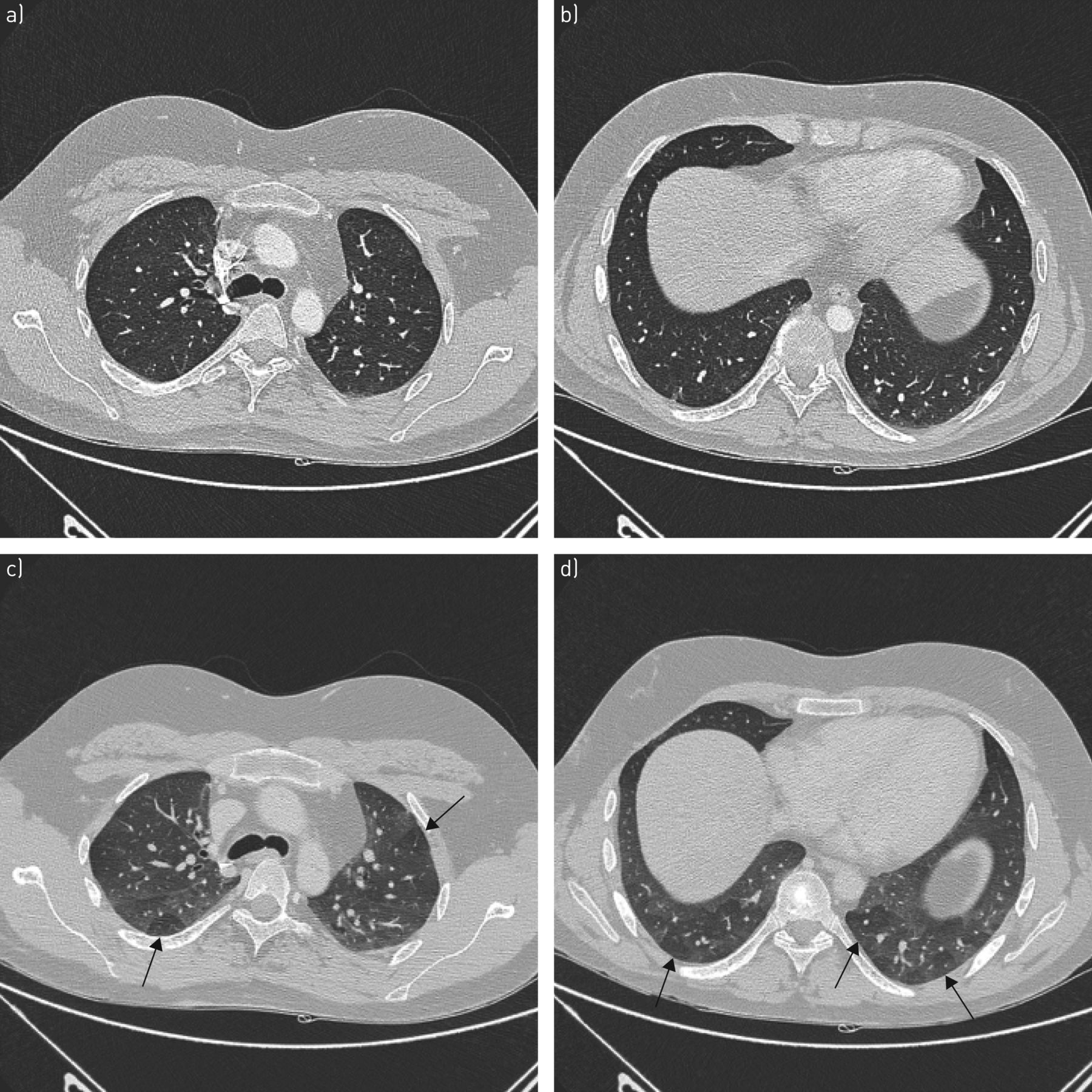
A simpler way of measuring function is to look at regions affected by gas trapping where lung tissue fails to deflate on the expiratory scan when compared to the inflation scan; this is recognised as a marker of small airway function because terminal bronchioles are recognised as the site of airway closure. There are no direct CT–structure correlations between expiratory gas trapping and histopathological measures of small airways. However, these low-density regions on the expiratory scan, which can be easily measured (figure 1) and correlations with systemic markers of presumably small airway function [65] support the concept that expiratory gas trapping represents small airway function. In addition, gas trapping has been investigated using complex lung function tests (single-breath nitrogen washout). Increased airway closure has been associated with risk of severe asthma exacerbations [66]. Similarly, gas trapping measured using expiratory CT was associated with severe asthma attacks, longer duration of asthma, airflow obstruction and airway neutrophilia [67]. The effect of corticosteroid treatment on gas trapping measured by CT has also been studied [25, 68]. Gas trapping (assumed to be due to small airway closure) was reduced by small-particle inhaled corticosteroid aerosol treatment, which suggest that the function of the small airways can be modified using small-particle aerosols. These results, together with similar results of studies involving forced oscillation technique and nitrogen washout [69, 70] suggest that small-particle aerosols are beneficial for treating the small airways. However, these studies are difficult to conduct and the benefits of using small-particle aerosols over larger particle formulations on small airway function remain to be definitively studied.

a, b) Inspiratory and c, d) expiratory computed tomography scans from the same subject, at two levels. The image in a) is at approximately the same anatomical location as c) and b) is at approximately the same location as d). The arrows on the expiratory images indicate regions of gas trapping due to severe narrowing and airway closure.
Another way of measuring function is to examine changes in the airway dimensions at different lung inflations, which gives an indication of the mechanical properties of the airways, i.e. are the airways stiffer or more distensible? Such studies suggest that the physiological consequences of airway wall thickening may be more complex than just stiffening the airways and not allowing them to dilate on inspiration [71–73]. In these studies, the investigators suggest that airways can distend fully, but they do so at higher pressure, and that the lack of stretch at the lower distending pressures encountered during tidal breathing adversely affects airway smooth muscle contractile function, leading to enhanced airway narrowing in the presence of increased airway smooth muscle tone [71–73]. The importance of changes in airway mechanics in relation to airway hyperresponsiveness and airway narrowing remains incompletely understood.
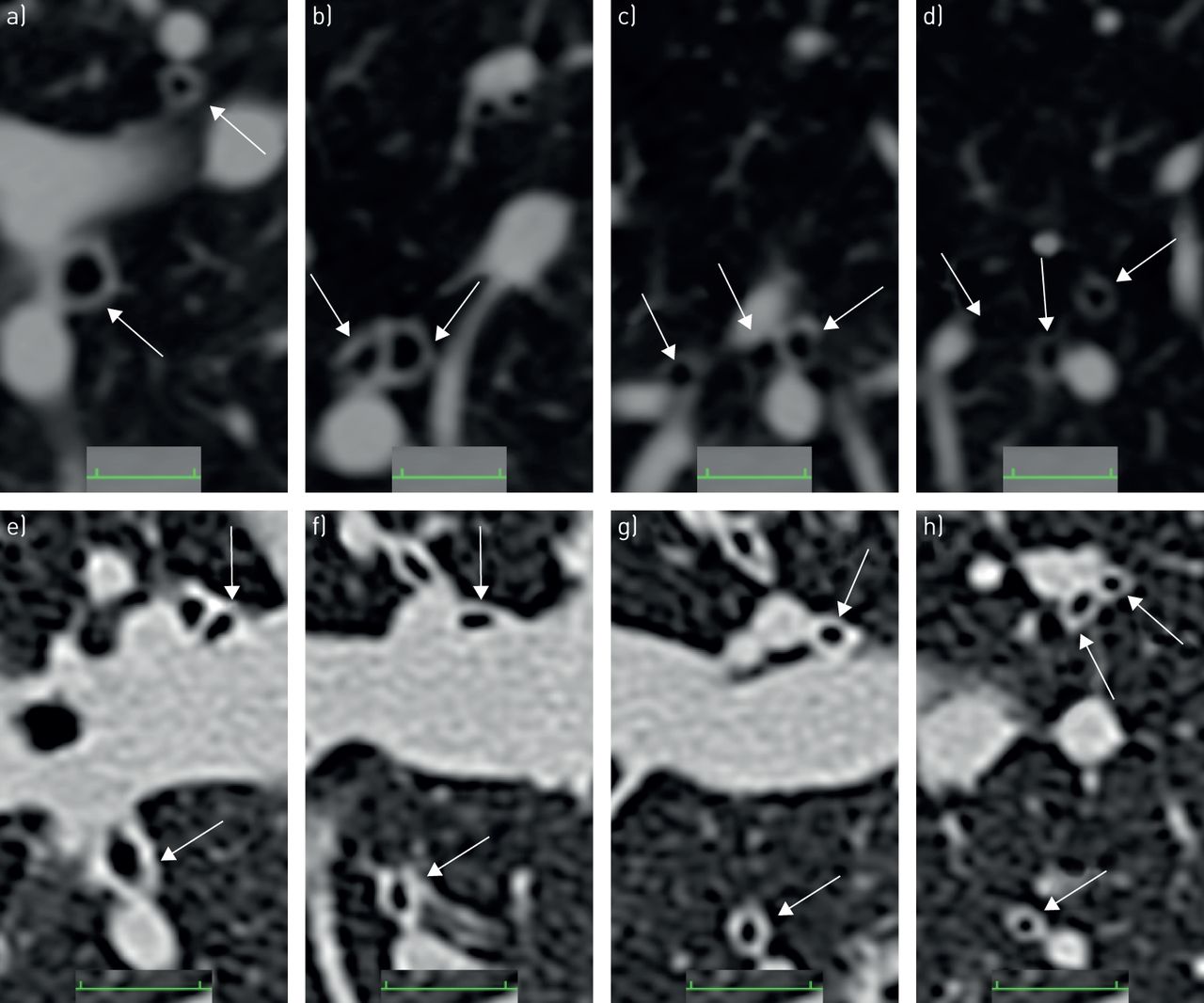
Changes in airway dimensions have been studied during induced bronchoconstriction. Okazawa et al. [74] performed one of the first studies of objective measurement of changes in airway calibre and wall thickness, before and after methacholine challenge, in asthmatic and non-asthmatic subjects, albeit using two-dimensional CT slices. Two subsequent similar CT studies, again in asthmatic and non-asthmatic subjects, but using automated computerised techniques, also showed that airway narrowing measured directly by CT was heterogeneous. Heterogeneity was estimated by comparing narrowing in “sister” airways (adjacent airways arising from the same parent airway), which was found to be uneven. Furthermore, airway closure at baseline and closure induced by methacholine were greater in asthmatic compared with non-asthmatic subjects [75, 76]. Results of both studies suggested that because asthmatic airway walls were thicker to start with, less airway narrowing was required to achieve a drop in FEV1, compared with the narrowing that was required to induce the same drop in FEV1 in non-asthmatic subjects (figure 2).

Magnified computed tomography images of airways in the right lower lobe from a–d) a healthy male subject and e–h) an asthmatic male subject. The arrows indicate airways cut in approximate cross-section, which can be seen to bifurcate caudally (from a–d and e–h). When the airways bifurcate to ∼2-mm diameter airways, the challenges of measuring the thin airway walls and small lumen diameters is apparent, whereas in comparison, regions of gas trapping as shown in figure 1 are much easier to measure. Determining localised wall thickening for a single airway is difficult. However, heterogeneity between sister airways (i.e. bifurcating from the same parent airway) and closure of airways have been shown to be greater in asthmatic compared with non-asthmatic airways [42, 75], albeit in medium- to small-sized airways. The functional consequences of heterogeneous narrowing and closure have been extensively examined in modelling [77] and inert gas washout studies [59, 61, 62], as well as the ventilation imaging studies described in this review. Scale bars=10 mm.
The mechanical and physiological consequences of thickened airways walls in asthma is uncertain; whether thickened asthmatic airways are stiffer or more compliant is unknown. Perhaps it depends on the severity of inflammation versus the extent of alterations (volume and organisation) in the intercellular matrix, collagen and elastin. However, there are two studies that suggest that asthmatic airway walls are stiffer, at least in terms of distension and stretch. Measurements of the changes in airway diameter with lung inflation using optical coherence tomography [78] and with forced oscillation technique [49] both suggest that airways are stiffer, i.e. asthmatic airways expand less with lung inflation compared with non-asthmatic airways.
Summary of understanding of asthma derived from CT studies
CT imaging is available in many centres and has been used extensively to look at airway and lung parenchymal structure. In addition, it has been used to look at the function of airways. Because of its nature, being three-dimensional digital data, it lends itself to sophisticated three-dimensional image analysis techniques. However, there are limitations to the CT technique: the difficulties in imaging small airways given the thinness of the airway walls in relation to CT resolution; the assumptions that are made in modelling such as in PRM; and the limited imaging available due to radiation considerations. Results of CT studies have supported the presence of heterogeneous ventilation in asthma, which may be due to both heterogeneous airway narrowing, inflammation and remodelling and heterogeneous changes in lung parenchyma. In addition, these studies confirm the increase in airway closure in asthma, and that bronchoconstriction leads to greater airway closure in asthmatic, compared with healthy airways. The topographical distributions of airway narrowing have not been comprehensively quantified from CT images. However, the three-dimensional distributions of airway narrowing and closure, which might represent patterns of inflammation and remodelling might be clinically relevant [24]. Hence, methods to measure the distribution of airway narrowing and closure need to be developed and then correlated with clinical parameters, e.g. exacerbation risk, asthma control and medication requirements. However, ventilation distribution might be better measured using ventilation contrast agents, rather than measuring it indirectly by CT.
Three-dimensional ventilation imaging
Three-dimensional ventilation imaging techniques include SPECT, PET and oxygen, xenon (Xe) or helium (He)-3 MRI. Ventilation can be seen in three-dimensional space of the lungs defined using structural images, by using a “ventilation agent” such as Technegas® for SPECT, Galligas® for PET, nitrogen-13 (13N) for PET, oxygen and hyperpolarised 129Xe or hyperpolarised 3He for MRI. Each of the methods have their own characteristics; therefore, the information provided by such imaging between techniques needs to be interpreted according to those methodological differences. Spatial resolution with these techniques is less than the spatial resolution of CT scans. However, heterogeneity of the distributions of ventilation measured in SPECT, PET and MRI are very readily apparent. Therefore, their respective spatial resolutions are adequate, relative to the length scales at which heterogeneities in ventilation occur in asthma. This does not exclude either similar or different patterns of heterogeneity at smaller length scales that are below the imaging resolution.
Technegas® and Galligas® ventilation agents have one characteristic that makes imaging with these agents unique. It is that once these ultra-fine (<1 µm) carbon particles are inhaled, they adhere to the lung structures without appreciable movement for ≥20 min, which allows upright inhalation followed by supine or prone imaging [79–81]. The use of hyperpolarised noble gas [82] or oxygen [83] requires imaging at the same time as the inhaled gas is delivered, which means the image data reflect supine ventilation. 13N imaging with PET reflects both perfusion and ventilation because the 13N isotope is delivered by venous injection and it is delivered by the pulmonary vasculature to the lungs, where it then diffuses into the alveoli and is cleared by regional ventilation [84]. Hyperpolarised 129Xe [85] or 3He [82] are delivered by a single deep breath with a breath-hold during imaging, while oxygen-enhanced MRI is performed during tidal breathing [83]. Each of these differences in imaging technique will dictate significant differences in quantification of regional ventilation and its distribution.
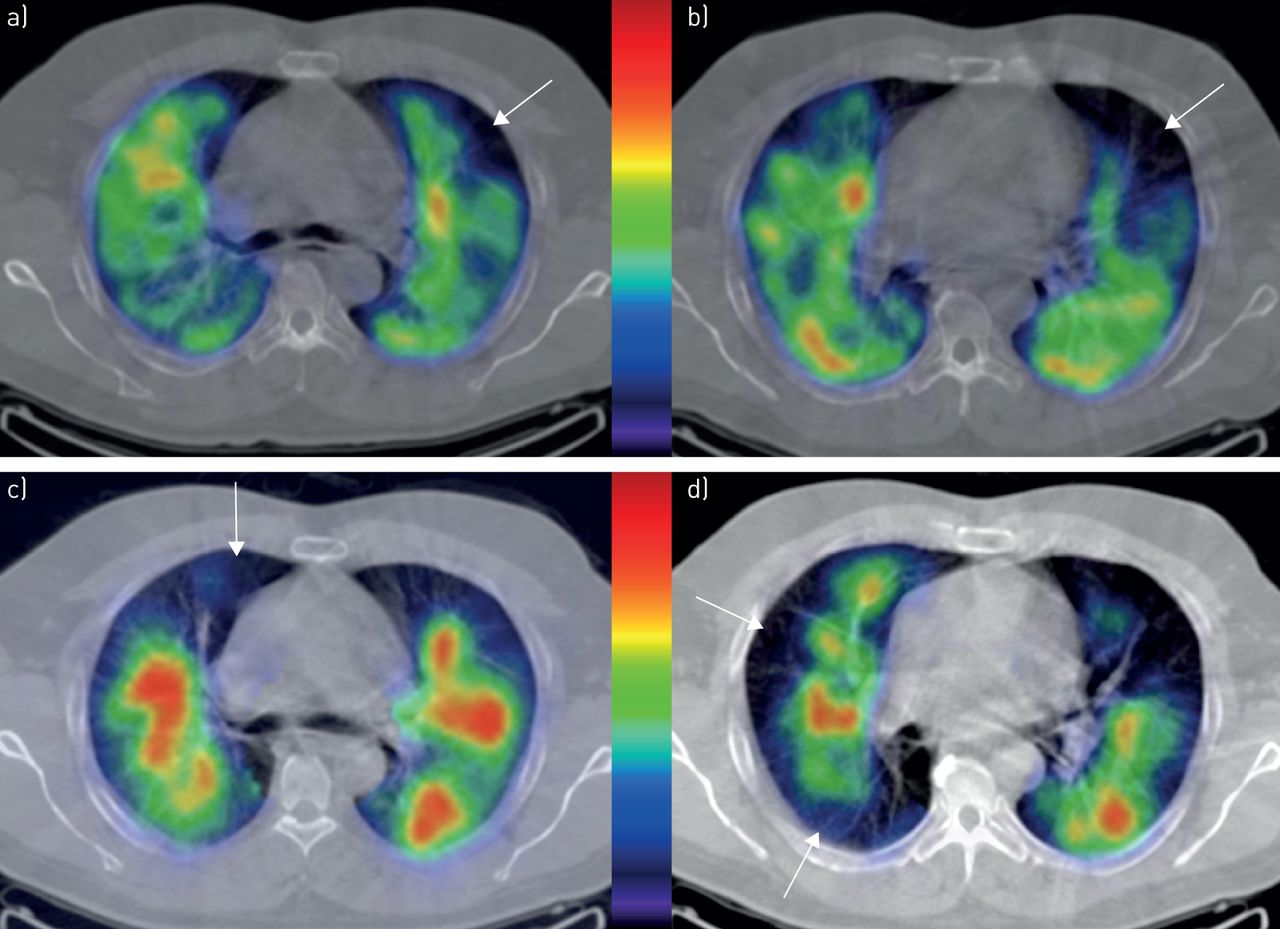
SPECT imaging with Technegas® in asthma shows that ventilation can become significantly heterogeneous during bronchoconstriction [80, 81]. Areas of closure as well as reduced ventilation occur (figures 3 and 4). The fact that regions of the lung stop ventilating has been known for a long time from past imaging studies [86–91]. The contribution of the more recent studies with Technegas® [80, 81] were in relating them to small airway function and airway hyperresponsiveness. The link provided experimental evidence for the long held view, supported by computational modelling [77, 92, 93], that the small airways were an important determinant of airway narrowing and airway hyperresponsiveness in asthma. The Technegas® studies showed that airway closure was induced by bronchoconstriction and the severity of the closure (how much lung it affected) was predicted by small airway function and severity of airway hyperresponsiveness at baseline [81]. Similarly, the development of airway narrowing (reduced ventilation as represented by change in Technegas® activity) was predicted by small airways that were even more peripheral than those that determined closure [81]. The possibility that the topographical pattern of bronchoconstriction is determined by small airway function is intriguing, the mechanistic and clinical implications of this however, are at present uncertain. Figures 3 and 4 show dramatically different patterns of change during bronchoconstriction, despite similar falls of ∼20% in FEV1. There may be important information contained in the different patterns of bronchoconstriction. However, methods of quantifying topographical distributions and patterns need to be developed for ventilation imaging, so that its pathophysiological and clinical implications can be determined.

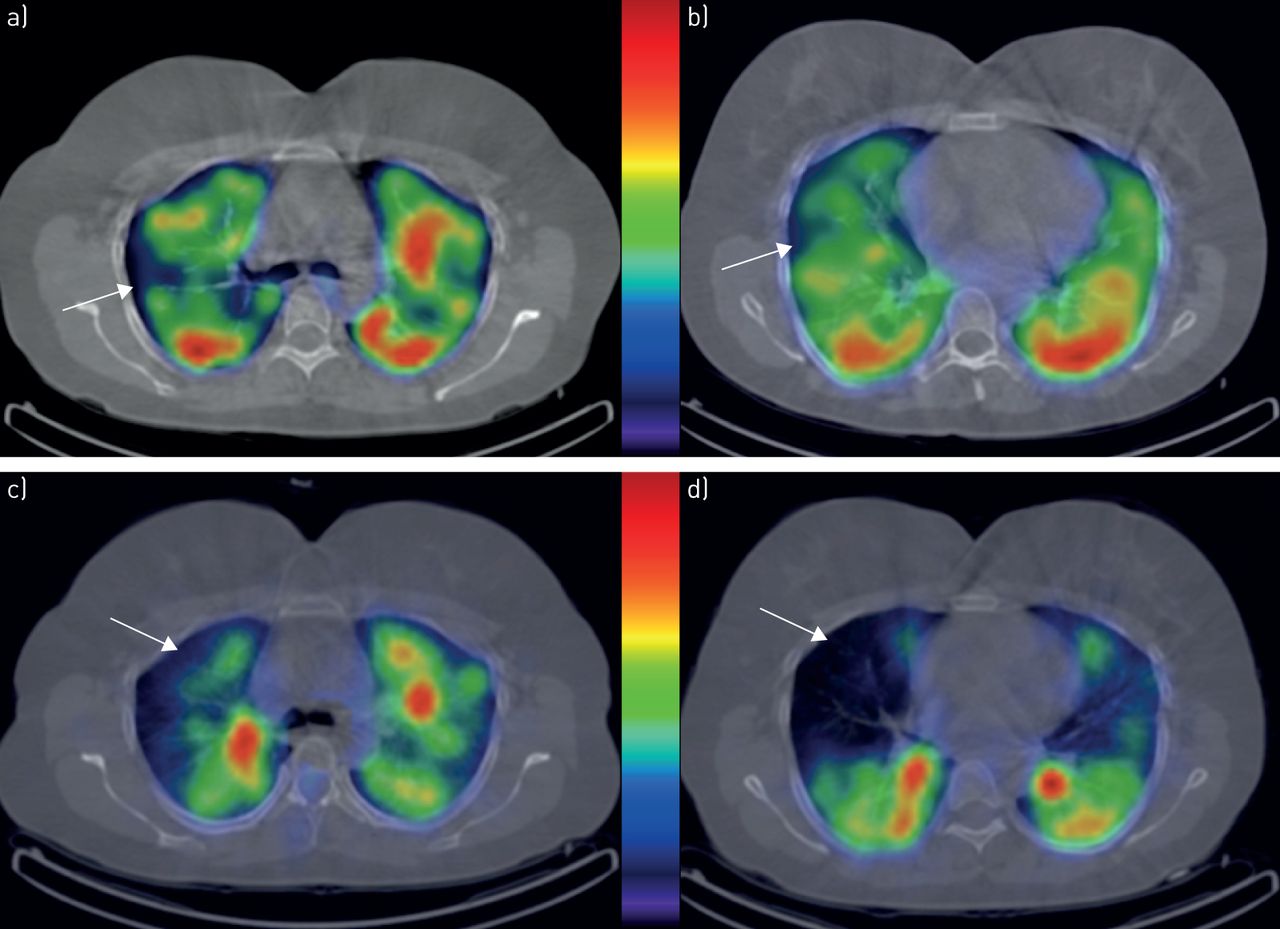
Single photon emission computed tomography ventilation images of a female asthmatic at a, b) baseline and c, d) post-methacholine challenge, at approximately corresponding anatomical locations. The centre colour bar indicates relative activity of Technegas® (highest relative activity being red). The white arrows indicate ventilation defects at baseline (a and b) and new defects post-methacholine challenge (c and d), after a ∼20% fall in forced expiratory volume in 1 s. As well as the development of new ventilation defects, the ventilation patterns have also changed. The challenge currently is to quantify the changes in ventilation patterns, which will require complex statistical methods, and to relate these to clinically relevant parameters.

Single photon emission computed tomography ventilation images of a male asthmatic subject at a, b) baseline and c, d) post-methacholine challenge, at approximately corresponding anatomical locations. The baseline scans show ventilation defects and a different pattern of ventilation anatomically. The new ventilation defects induced after methacholine challenge are subjectively apparent (arrows in c and d), as well as the changed ventilation patterns. Developing measurements that capture this topographical information that allows comparisons between ventilation patterns in figures 3 and 4 will be potentially useful to define different pathophysiological phenotypes of asthma.
13N PET imaging also demonstrated bronchoconstriction-induced regional airway closure [94]. Perhaps the most interesting observations relevant to what determines bronchoconstriction have come from the finding that posture dramatically affects airway closure [95]. Unlike SPECT imaging, where Technegas® can be inhaled in upright posture, PET imaging, like magnetic resonance ventilation imaging, is acquired at the time the ventilation “contrast agent” is administered. Therefore, 13N PET shows the pattern of ventilation in supine, decubitus or prone posture. Regional airway closure was shown to be gravitationally dependent, i.e. when changing from supine to prone posture, airway closure shifted to the most dependent regions during bronchoconstriction [95]. This suggests that parenchymal distending forces are a strong determinant of airway narrowing and closure since the dependent lung is less distended and thus exerts less distending forces on the airways to resist airway narrowing and closure. These findings are also consistent with the Technegas® SPECT findings where airway closure was found to be greatest in the gravitationally dependent regions [96].
The observations from imaging that clear-cut, highly localised regions of nonventilation were induced by airway smooth muscle contraction led to computational modelling studies to find a physiological explanation for this. One hypothesis that has been popularised is that bronchoconstriction in asthmatic airways is widespread, affects small and large airways and is unstable. This instability then leads to a self-organised, new stable state, where regions of airway closure have developed. The proposed mechanisms rely on a highly integrated interconnectivity between small airways [77], which are joined together by the lung parenchyma. An alternative hypothesis is that remodelling and inflammation are distributed unevenly throughout the lung, which allows the worst-affected airways to form ventilation defects.
There has been a large body of work on ventilation imaging using hyperpolarised 3He MRI in asthma [38, 82, 85, 97–99]. The presence of ventilation defects due to airway closure during bronchoconstriction is a consistent finding and recently has been correlated with thickening of the airways measured from CT [99] scans, airway hyperresponsiveness [99] and with eosinophilic inflammation measured in sputum [98] and neutrophilic inflammation [100] measured from bronchoscopic washes. These associations suggest that there are local mechanisms that determine airway closure in large and medium-sized airways. This is not necessarily contradictory to the hypothesis that small airways function is critical in asthma. Nor does it necessarily contradict the “instability and self-organised closure” hypothesis above. Hypothetically, when there is widespread small airway narrowing, the mechanical state of the lungs is then “set up” for regionalised closure to develop. Then when some localised “spots” in the larger airways narrow, the subtending distal airways then close, forming the well-recognised patterns of airway closure.
Moreover, there is good evidence from MRI studies that the severity of airway closure, measured by how much lung is not ventilated, is associated with clinical markers of asthma severity [97] and risk of asthma exacerbations [101]. In subjects with severe asthma, ventilation defect volumes reduce with acute bronchodilator inhalation [98], but less so when there is sputum eosinophilia. Therefore, airway closure on ventilation imaging appears to be associated with asthma severity and poor control of type II inflammation and as such, there is a strong argument that ventilation imaging is a clinically relevant physiological measurement for characterising asthma.
Finally, airway closure has been the characteristic physiological abnormality that has been almost the sole focus of research attention in three-dimensional imaging studies. This might be understandable because ventilation defects are dramatic and represent excessive airway narrowing, arguably the most important mechanical abnormality of asthmatic airways which probably represents airway hyperresponsiveness (figures 3–5). However, there is much more that can be measured from those three-dimensional images (figure 5). Although the number and volume of those ventilation defects have been the focus of measurement in MRI ventilation imaging studies, complex regional analyses are possible to quantify the variance in ventilation regionally, i.e. ventilation heterogeneity in a topographical context [102]. Textural properties might provide mechanistic insights, which may also be relevant clinically. In particular, patterns of airway narrowing (reduced ventilation) may provide additional information, e.g. where low ventilation occurs, are they connected as one major zone or separated and scattered around the lungs, the statistical distribution of ventilation etc. However, although quantitative methods for measuring ventilation distribution exist, the studies relating them to clinical outcomes are lacking.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
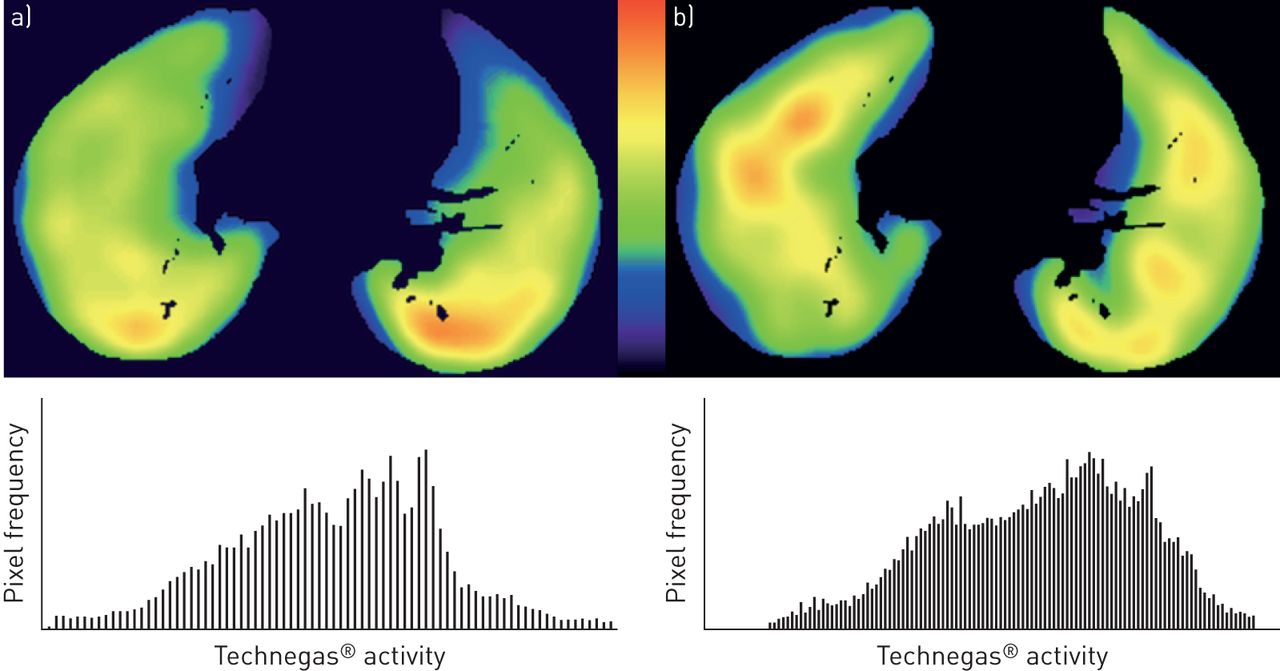
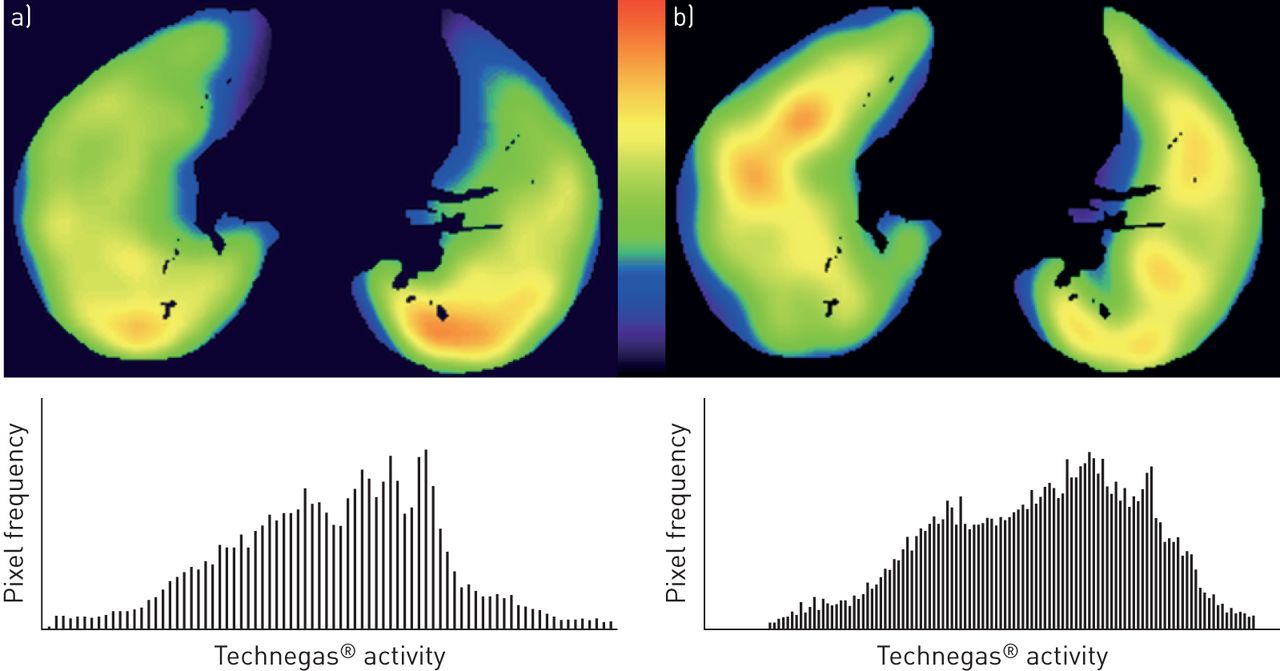
Technegas® ventilation single photon emission computed tomography images of an asthmatic subject (axial slices) at a) baseline and b) post-methacholine after 20% fall in forced expiratory volume in 1 s. The graphs below are the correspondence frequency distributions of Technegas® intensity, which are estimates of relative ventilation. The colour bar between images a) and b) indicates Technegas® activity, with red being highest and purple being the lowest. The pattern of ventilation clearly changes, post-bronchoconstriction with ventilation moving ventrally in both lungs. A number of statistical indices could be derived from the frequency distribution, as part of future research in characterising patterns of ventilation and their change with interventions.
Summary of understanding of asthma from ventilation imaging studies
Ventilation imaging shows airway closure and ventilation distribution in a topographical sense, and within the confines of spatial resolution of the techniques. Inert gas washout measurement of ventilation distribution and of airway closure are of the same physiological phenomenon, but there are significant methodological differences that mean that the information is complementary rather than interchangeable. This may explain the relatively few correlations between imaging and washout studies. Nevertheless, there are important insights into the pathophysiology of asthma provided by imaging's topographical content. Airway closure can be widespread and is distributed in a patchy, “clustered” manner; whether it is due to airway remodelling, parenchymal remodelling, mucus plugs or local inflammation is unknown. Studies looking at the distribution of closure as a potential phenotyping tool, as a marker of asthma severity or as a treatment target would be important in the future. This is because the intersubject variability in topographical patterns of ventilation and airway closure is very high, which might translate to variation in symptoms, control or responses to treatment. Ventilation defects are inducible by inhalation of bronchoconstrictors, and at least some of the defects are removed by bronchodilator inhalation. This means that reversing excessive narrowing should improve airway hyperresponsiveness, but this will require more than just bronchodilator treatment. The effects of anti-inflammatory treatment on closure still needs study.
Conclusion
Results of studies with CT and ventilation imaging in asthma have shown that structural changes in airways and lung tissue are present in asthma and are associated with more severe asthma and more widespread airway closure. Greater structural abnormality seen on CT and greater functional derangement seen on ventilation imaging, are associated with greater asthma severity and exacerbation risk as well. These associations provide convincing evidence that characterisation of pathophysiology is important and clinically relevant in asthma, and will be a necessary element of comprehensive phenotyping of asthma in the future.
However, imaging research has raised many more questions that still need answering. The topographical analysis of ventilation defects and of ventilation distribution have not been thoroughly explored. Ventilation defects can be distributed throughout the lung in different ways, e.g. a single large defect or many separate, small defects. Similarly, ventilation, as opposed to ventilation defects, is likely to be distributed in different patterns. Determining the clinical correlates of these topographical patterns will provide both mechanistic insights and potentially useful research tools to develop new treatments. The mechanical basis of airway closure and narrowing in asthma remains incompletely understood. There is probably a complex interaction involving functional and structural changes in airway smooth muscle, mucosa, airway surface liquid and mucus, extracellular matrix, peribronchiolar and lung tissues and inflammation. Detailed structural and functional studies of these localised regions of excessive airway narrowing, and comparison with nonreactive regions in the same individual might provide important insights into the causes of asthmatic airway narrowing, i.e. explaining the cause of heterogeneous ventilation.
In summary, better characterisation of asthma with sophisticated tools such as imaging is going to be critical in progressing towards newer treatments, strategies, prevention and cure, which have so far been elusive [4].
Footnotes
Number 2 in the Series “Dismantling Airway Disease” Edited by Sinthia Bosnic-Anticevich and Marc Humbert
Previous article in this Series: No. 1: Zimmermann SC, Tonga KO, Thamrin C. Dismantling airway disease with the use of new pulmonary function indices. Eur Respir Rev 2019; 28: 180122.
Provenance: Submitted article, peer reviewed.
Conflict of interest: G.G. King reports grants from CycloMedica and MundiPharma during the conduct of the study; grants, personal fees and other funding from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Menarini and MundiPharma; grants from the National Health and Medical Research Council and Asthma Foundation; other funding from the ATS and ERS; and non-financial support and other funding from Restech, outside the submitted work.
Conflict of interest: C. Farrow reports grants from CycloMedica Australia, outside the submitted work.
Conflict of interest: D. Chapman reports grants from Cyclomedica during the conduct of the study.
- Received December 11, 2018.
- Accepted March 1, 2019.
- Copyright ©ERS 2019.
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










