





Figures
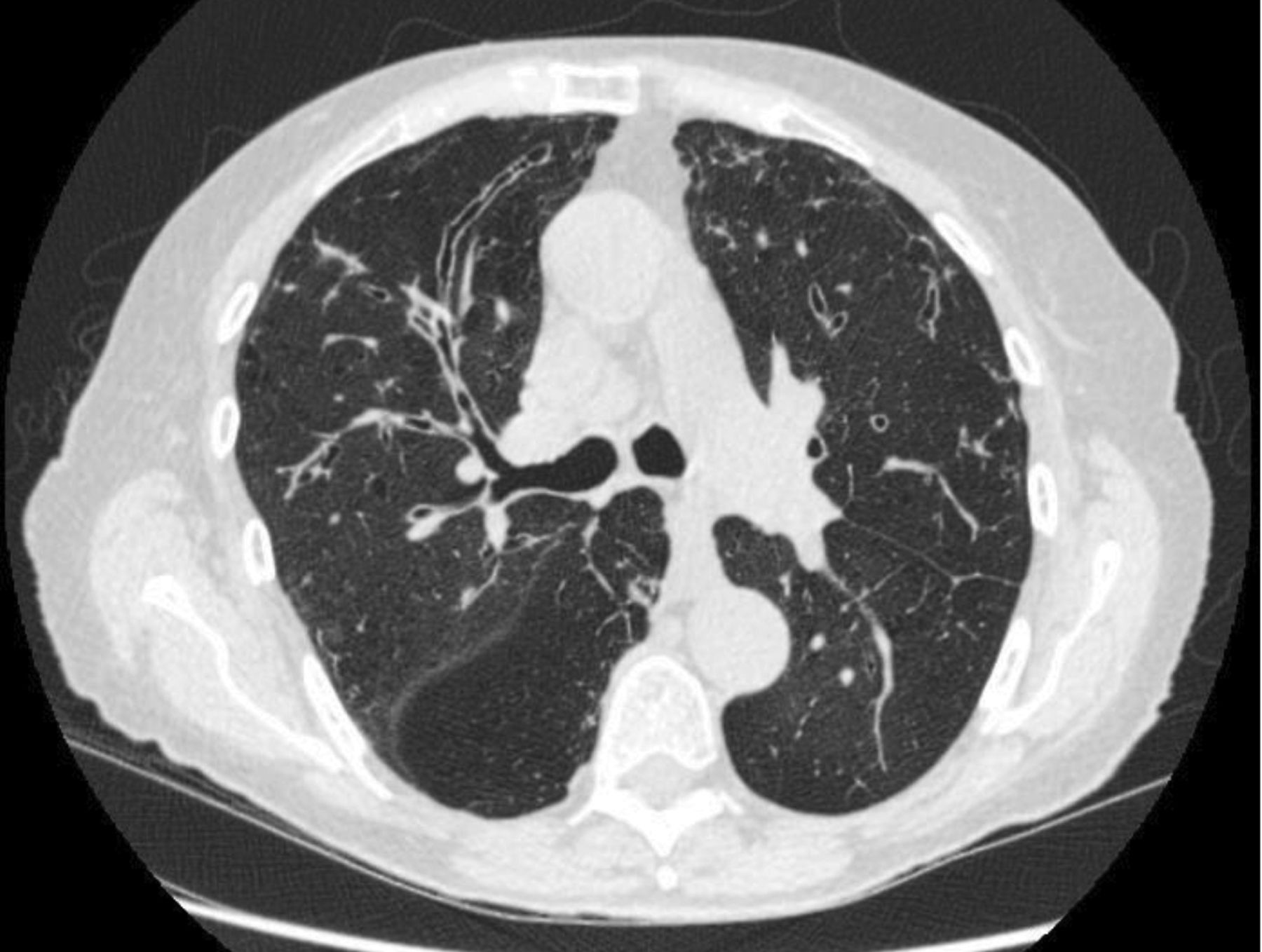
- FIGURE 1
Varicose and cystic bronchiectasis with mucus plugging in upper lobes.
- FIGURE 2
Central tubular bronchiectasis in upper lobes.
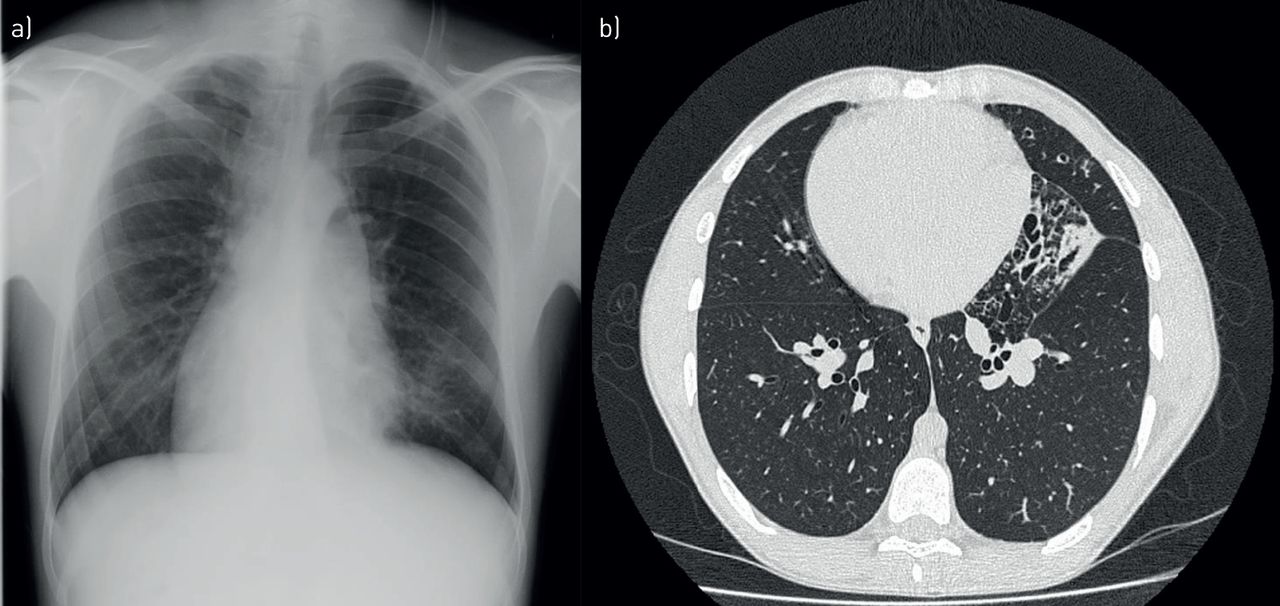
- FIGURE 3
a) Chest radiograph showing dextrocardia. b) High-resolution computed tomography showing cylindrical bronchiectasis in the lingula.
- FIGURE 4
Cylindrical bronchiectasis and tree-in-bud pattern in lower lobes and middle lobe.
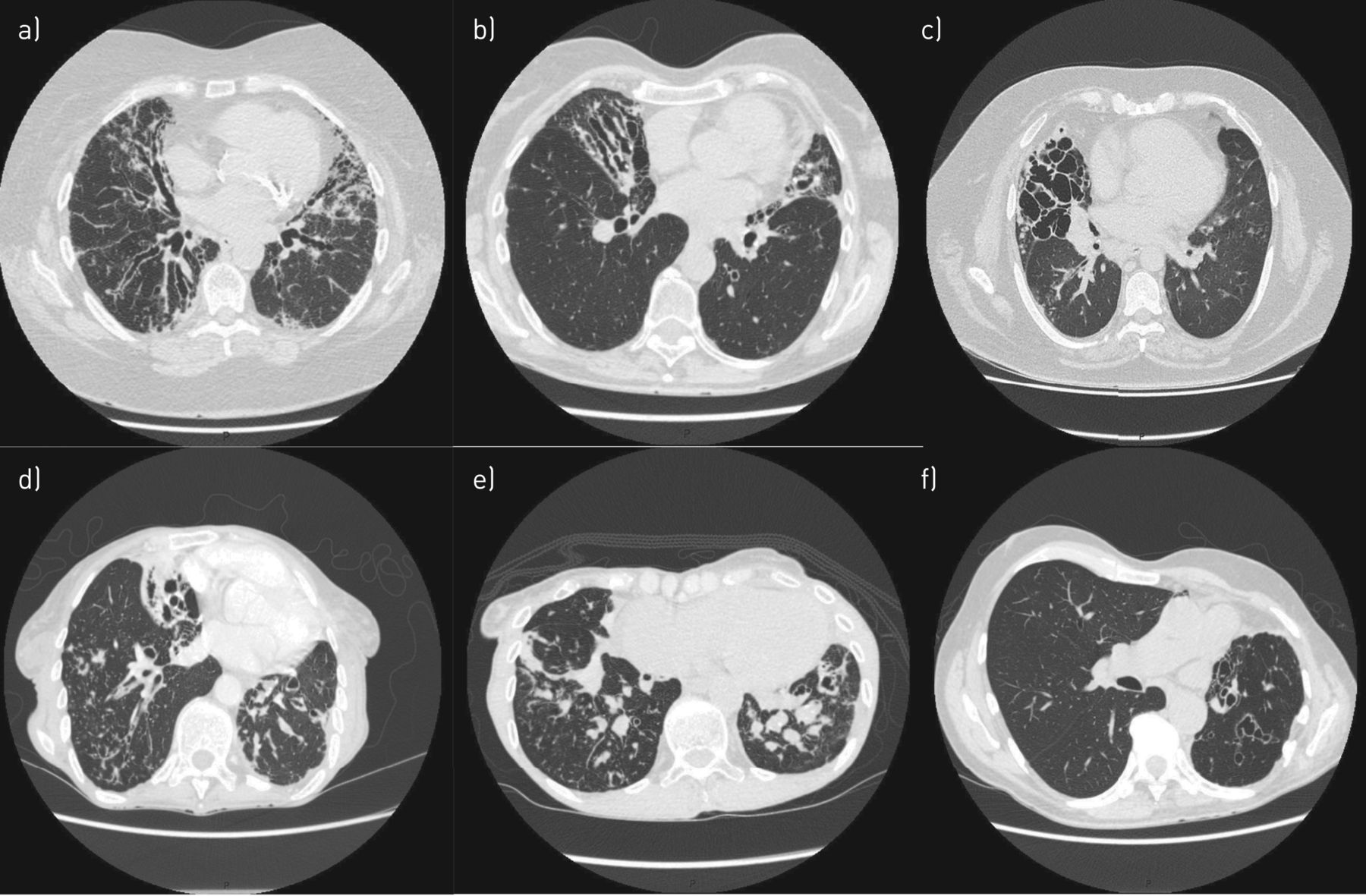
- FIGURE 5
Different radiological “phenotypes” of bronchiectasis. a) Tubular bronchiectasis in lower lobes, b) varicose bronchiectasis in lower lobes, c) cystic bronchiectasis in right lower lobe, d) cystic bronchiectasis with tree-in-bud pattern and mucus plugging in lower lobes (cavitation in right lower lobe), e) mucus plugging and tree-in-bud pattern in lower lobes, f) varicose bronchiectasis in upper lobes and lingula.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Aetiologies of bronchiectasis
Category Cause/notes Clinical phenotype Specific treatment Post-infection Viral, bacterial, fungal, mycobacteria (usually classified separately) Past history of severe infection; classically unilobar bronchiectasis No specific treatment NTM M. avium and M. abscessus most frequent Middle-aged or elderly; females with low BMI; middle lobe and lingual nodular bronchiectasis; cavitation; tree-in-bud Antibiotic treatment Post-TB M. tuberculosis Upper lobe most frequently No specific therapy ABPA Hypersensitivity to A. fumigatus History of asthma (not universal); thick sputum; S. aureus in sputum; central bronchiectasis; fleeting infiltrates Steroids±antifungals COPD Smoking, biomass exposure Fixed airflow obstruction; smoking history; bilateral lower lobe; tubular bronchiectasis No specific therapy Asthma Not universally accepted as a cause of bronchiectasis Long history of asthma; frequent exacerbations; neutrophilic airway inflammation Inhaled corticosteroids, biologics e.g. anti-IgE and anti-IL5 Aspiration/inhalation Foreign body aspiration, gastric contents aspiration, inhalation of corrosive substances Lower lobe bronchiectasis Speech and language therapy, fundoplication, removal of exacerbating drugs Obstruction Benign tumours, enlarged lymph nodes Single lobe bronchiectasis Removal of obstruction via bronchoscopy or thoracic surgery Congenital defects of large airways Marfan syndrome, Mounier-Kuhn syndrome (tracheobronchomegaly), Williams–Campbell syndrome (bronchial cartilage deficiency) Specific features depending on the congenital defect Dependant on the underlying disorder AATD Unopposed protease activity Combined emphysema and bronchiectasis Augmentation therapy is available in some countries Yellow nail syndrome Lymphatic obstruction Dystrophic nails, pleural effusions, rhinosinusitis Local treatment for nails e.g. vitamin-E, management of lymphoedema Immunological defects Primary: common variable immune deficiency, agammaglobulinemia, hyper-IgE syndrome; secondary: chemotherapy, immunosuppressant therapy, malignancy, HIV/AIDS Varied clinical pattern depending on the underlying cause; patient may give a history of non-respiratory infections Ig replacement, prophylactic antibiotics, treatment of underlying disorder, removal of iatrogenic immunosuppression Young's syndrome Cause not known Bronchiectasis, rhinosinusitis and reduced fertility See ciliary disorders below PCD Genetic Middle lobe and lower lobe bronchiectasis; rhinosinusitis; middle ear infections; situs inversus in some cases Recognition and treatment of associated problems (including rhinosinusitis, middle ear disease, infertility, ectopic pregnancy), genetic counselling, intensive airway clearance Systemic inflammatory disease Rheumatoid arthritis, sarcoidosis, systemic lupus erythematosus, Sjögren syndrome Varied clinical pattern, often rapidly progressive No specific treatment Inflammatory bowel disease Ulcerative colitis, Crohn's syndrome, coeliac disease Varied clinical pattern often high sputum volumes and steroid responsive Inhaled and systematic corticosteroids, treatment of the underlying condition Adult CF CFTR mutations Upper lobe bronchiectasis; P. aeruginosa or S. aureus in sputum; non-respiratory manifestations Specialist multidisciplinary care in adult CF centres, recognition and treatment of non-respiratory manifestations, CFTR modulator/corrector therapy Diffuse panbronchiolitis Idiopathic inflammatory disease Mostly patients of Far Eastern ethnic origin Macrolide antibiotics NTM: nontuberculous mycobacteria; TB: tuberculosis; ABPA: allergic bronchopulmonary aspergillosis; COPD: chronic obstructive pulmonary disease; AATD: α1-antitrypsin deficiency; PCD: primary ciliary dyskinesia; CF: cystic fibrosis; M. avium: Mycobacterium avium; M. abscessus: Mycobacterium abscessus; M. tuberculosis: Mycobacterium tuberculosis; A. fumigatus: Aspergillus fumigatus; S. aureus: Staphylococcus aureus; BMI: body mass index; Ig: immunoglobulin; IL: interleukin; CFTR: cystic fibrosis transmembrane conductance regulator; P. aeruginosa: Pseudomonas aeruginosa.










