





Abstract
Anatomical segmentectomy has been developed to offer better pulmonary function preservation than lobectomy, in stage IA lung cancer. Despite the retrospective nature of most of the studies and the lack of randomised studies, a substantial body of literature today allows us to evaluate to what extent lung function decreases after segmentectomy and whether segmentectomy offers a real functional benefit over lobectomy. From the available series, it emerges that the mean decrease in forced expiratory volume in 1 s (FEV1) is low, ranging from −9% to −24% of the initial value within 2 months and −3 to −13% 12 months after segmentectomy. This reduction in lung function is significantly lower than that induced by lobectomy, but saves only a few per cent of pre-operative FEV1. Moreover, the published results do not firmly establish the functional benefit of segmentectomy over lobectomy in patients with poor lung function. Some issues remain to be addressed, including whether video-assisted thoracic surgery (VATS) segmentectomy may preserve lung function better than VATS lobectomy in patients with poor lung function, especially within the early days after surgery, and whether this may translate to lowering the functional limit for surgery. Eventually, trials comparing stereotactic ablative body radiotherapy, radiofrequency ablation and segmentectomy functional consequences are warranted.
Abstract
Lung segmentectomy offers mild post-operative to small long-term functional benefits over lobectomy http://ow.ly/dcPQ30fuCU9
Introduction
Anatomical segmentectomy has been implemented to offer better pulmonary function preservation than lobectomy. The rapid integration of this procedure as routine is explained first by the development of computed tomography (CT) screening for lung cancer, which allows the diagnosis of lung cancer at a very early stage (IA). Second, the assumption that reducing the resected lung volume may enhance the possibility of further resections in the case of a second primary lung cancer has provided an additional substantial incentive to perform segmentectomy. The third factor contributing to the development of this procedure was the intent to propose surgical treatment to patients with impaired lung function. Indeed, based on early published studies, the use of segmentectomy in these patients was recommended as an alternative to lobectomy by several task forces, the European Respiratory Society/European Society of Thoracic Surgeons in 2009 [1], the British Thoracic Society in 2010 [2] and the American College of Chest Physicians in 2013 [3]. In addition to survival analysis comparing segmentectomy to lobectomy, several recent studies have focused on the functional consequences of lung segmentectomy. In light of these latest results, it is worth reconsidering to what extent lung function decreases after segmentectomy compared to lobectomy and whether segmentectomy offers a real functional benefit over lobectomy. Also, the recent development of stereotactic irradiation or even radiofrequency ablation for early-stage (stage IA) lung cancer deemed inoperable, as an alternative to surgery, further justifies having strong data regarding the advantages and inconveniences of those treatments.
In this article we review all the published articles providing pulmonary function tests (PFTs) performed before and after segmentectomy, and focus on those comparing lobectomy and segmentectomy. We extracted data to examine to what extent pulmonary function is impaired after segmentectomy, if segmentectomy better preserves lung function than lobectomy, if video-assisted thoracic surgery (VATS) segmentectomy further increases the functional benefit attributed to open segmentectomy, and if segmentectomy provides a real functional benefit to patients with poor lung function.
Methods
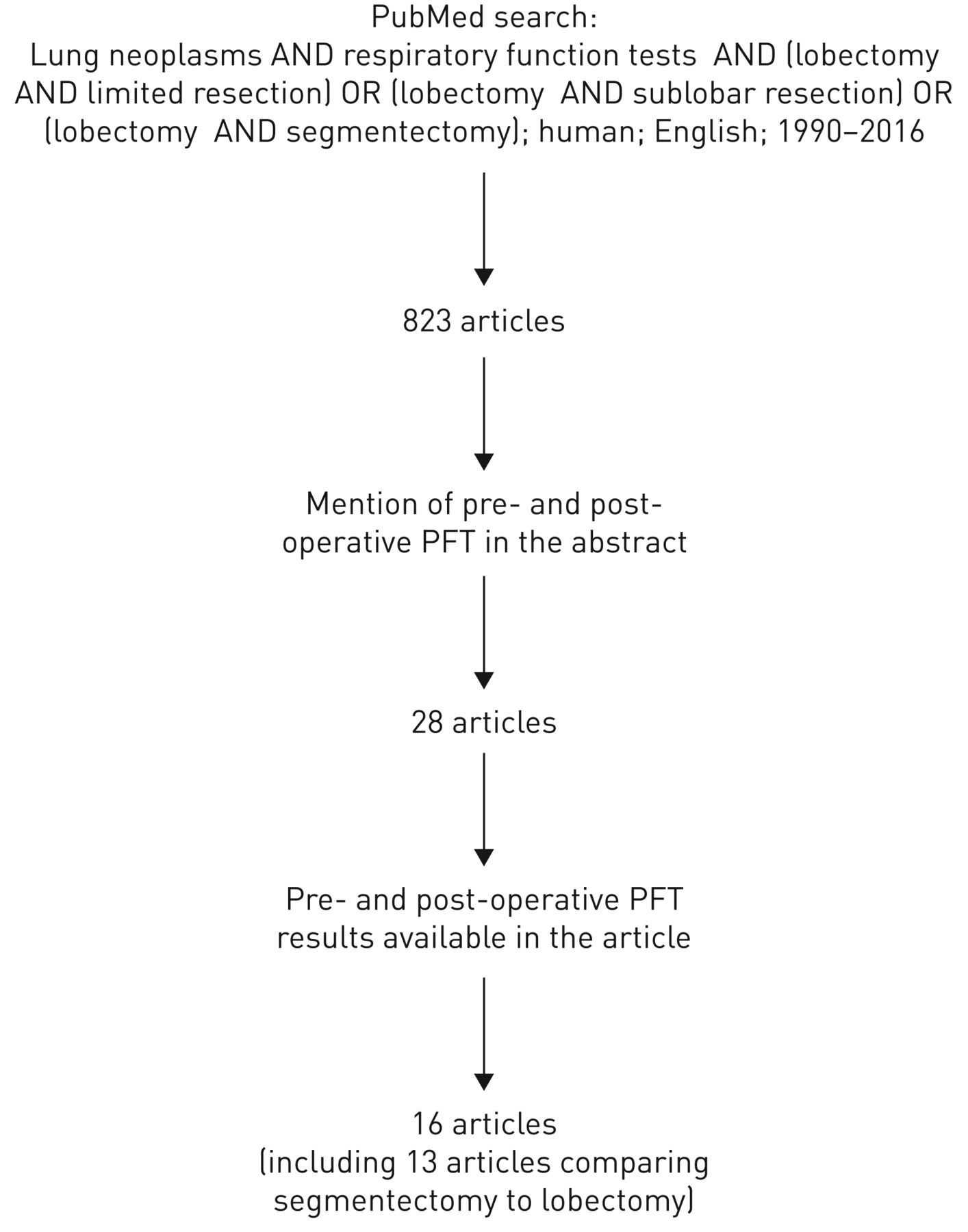
We performed a search in the PubMed database using the following strategy: lung neoplasms (MeSH term) AND respiratory function tests (MeSH term) AND (lobectomy AND limited resection) OR (lobectomy AND sublobar resection) OR (lobectomy AND segmentectomy). Only English-language articles and human studies published between January 1, 1990 and December 31, 2016 were included. References of relevant articles were also manually searched to identify potentially eligible articles. We selected the articles providing pre-operative and post-operative lung function studies, or post-operative variations in pulmonary function (figure 1).

Flow chart showing the results of the bibliographic search. PFT: pulmonary function test.
Results
Functional changes after segmentectomy
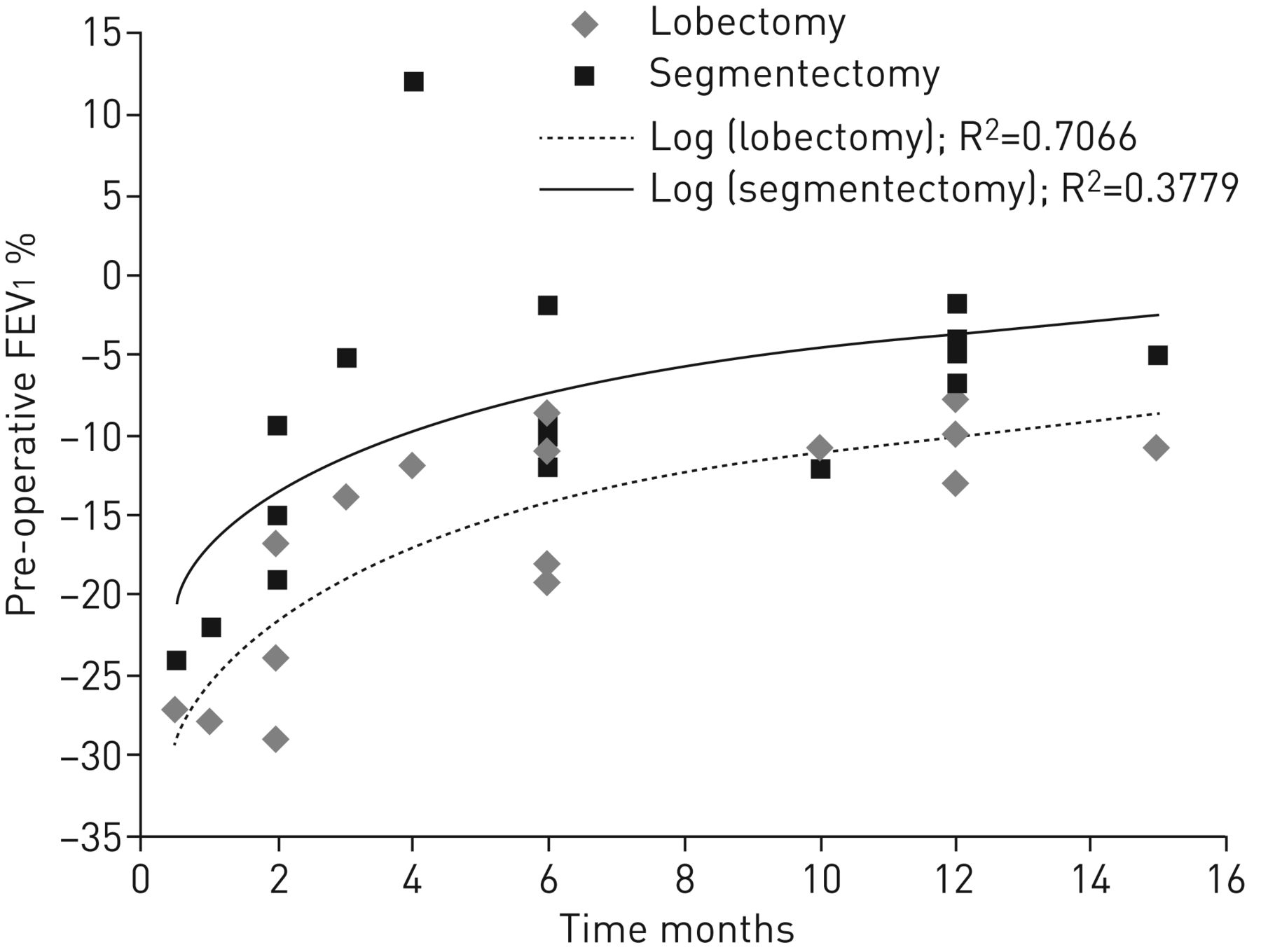
A total of 16 studies, including 1137 patients [4–19], provided pre- and post-operative functional values (table 1). Forced expiratory volume in 1 s (FEV1) was the most frequently reported functional value, so we focused on this parameter. The mean variation in FEV1 varied widely from one study to another, ranging from −24% to +12% of the initial value. Only one study reported a gain in FEV1 (+12%). This study included patients with impaired lung function and with predicted post-operative FEV1 <40% [11]. The loss of lung function decreases over time after surgery and a more intelligible picture emerges from figure 2, which shows the time-course of FEV1 after segmentectomy [4–6, 8–11, 13–16]. Within 2 months after surgery, the loss of FEV1 (mean value of the study) ranged from −9% to −24% of the initial value in five series (mean of the studies −18%) [5, 13–16], whereas after 12 months the loss ranged from −3% to −13% (mean −7%) [4, 8, 9, 16, 18].
Studies providing pre- and post-segmentectomy pulmonary function tests (PFTs)

{kind=link}
{kind=link}
Four studies examined the relationship between the number of resected segments and the loss of pulmonary function. Harada et al. [5] found a significant relationship using logistic regression. Hwang et al. [6] compared the loss of FEV1 linked to the resection of one, two or three segments and found no statistical difference, but the power of the analysis was not specified. Yoshimoto et al. [19], combining lung function measurement and imaging techniques, showed that the resection of one and two segments preserved 49% and 35% of pre-operative FEV1 of each lobe, respectively, whereas the resection of three or four segments preserved a significantly lower fraction (17% of FEV1). Finally, Nomori et al. [12] compared the functional impact of the resection of <2 segments, ≥2 segments and of the left upper division, the volume of resected lung increasing from the first to the last group. The differences in loss of FEV1 between groups were statistically significant.
Does segmentectomy preserve lung function better than lobectomy?
13 studies compared the functional consequences of these two procedures, with a total of 1093 lobectomies and 911 segmentectomies. The results are summarised in table 2 and figure 2. Four studies matched the patients' characteristics [11, 13, 16, 17]. Five studies were prospective [4, 5, 12, 13, 16] and only one was a randomised study [4]. Two studies included wedge resections and not only anatomical segmentectomies [4, 9]. Only two studies found that reductions in FEV1 did not differ significantly after segmentectomy or lobectomy [6, 15]. Again, when evaluating the difference between lobectomy and segmentectomy, the delay after surgery should be considered. Within 2 months after surgery, the mean loss of FEV1 ranged from −17% to −29% of initial value after lobectomy (mean −25%) and from −9% to −24% after segmentectomy (mean −18%) [5, 13–16]. Beyond 12 months, the mean FEV1 loss ranged from −8% to −13% of initial value after lobectomy (mean −11%) and from −2% to −7% after segmentectomy (mean −5%) [4, 8, 9, 16]. Within 2 months after surgery, the difference between lobectomy and segmentectomy was 3–10% of initial FEV1, whereas after 12 months, this difference ranged from 4% to 7% of initial FEV1. Kim et al. [9] performed a multivariate analysis on a series of 351 VATS lobectomies and segmentectomies and showed that preservation of FEV1 and diffusing capacity of the lung for carbon monoxide (DLCO) values was associated with sublobar resection. Altogether, these studies support the assumption that sublobar resection preserves more lung function than lobectomy, but to a small extent.
Studies comparing lobectomy and segmentectomy functional consequences
It is well known that the largest reduction in lung function occurs during the first days after surgery. Because the earliest functional data were collected 2 weeks after segmentectomy [16], whether the degradation of lung function is reduced very early after segmentectomy compared to lobectomy cannot be evaluated.
Does VATS segmentectomy further increase the functional benefit attributed to open segmentectomy?
Three series reported functional results after VATS segmentectomy, and six after open segmentectomy [4, 8, 13, 14, 16, 18], while the others included both procedures. The average loss of FEV1 in these studies was 5% (3–9%) with the VATS procedure (four measurements) and 9% (2–19%) with the open procedure (10 measurements), PFTs being performed with at least 1 month delay. Drawing firm conclusions from these studies is difficult. Indeed, no study compared VATS and open segmentectomy. In addition, studies of the early post-operative days, during which the functional benefit of VATS may be of importance, are lacking.
Does segmentectomy provide a real functional benefit to patients with poor lung function?
13 studies provided pre-operative FEV1 values (table 1) [5, 7–18]. In nine studies, the mean value of FEV1 was >70% of predicted. Some included patients with poor lung function but did not individualise this subgroup. Two studies focused on patients with impaired FEV1, with a mean pre-operative FEV1 of 55% [8] and 45% [11], respectively. One author compared patients with decreased FEV1 (<70%) to those with normal FEV1 [7]. In these three last studies open surgery [7, 8] or open surgery and VATS [11] were performed.
The two studies including only patients with impaired lung function showed that segmentectomy spared lung function compared to lobectomy (total number of studied patients: 65). The loss of FEV1 was 5% versus 10%, respectively, in the study by Keenan et al. [8]. Martin-Ucar et al. [11], who matched segmentectomy with lobectomy patients, showed a gain in lung function after segmentectomy (+12% FEV1, versus −12% after lobectomy). However, Kashiwabara et al. [7] found that segmentectomy had a functional benefit over lobectomy only in patients with FEV1 >70% (50 patients). In addition, in patients with emphysema, the variation of FEV1 was inversely correlated with predicted post-operative FEV1 in the lobectomy group (i.e. the higher the predicted post-operative FEV1, the stronger the loss in FEV1), but not in the segmentectomy group [7].
Comments
The design, as well as the surgical procedures (number of resected segments, tumour location, VATS or open surgery), varied widely from one study to another, and may explain part of the heterogeneity of the results. The main methodological issues are the retrospective nature of most of the studies and the lack of randomised studies, the lung cancer study group study being the only randomised study [4]. This last point may have led to underestimating of the real benefit of segmentectomy, because patients with the poorest condition may have been included in the segmentectomy group rather than in the lobectomy group.
From the published series, it emerged that the mean decrease in FEV1 ranged from −9% to −24% of the initial value (mean −18%) within 2 months and from −3% to −13% (mean −7%) 12 months after segmentectomy. In 11 out of 13 studies, this reduction in lung function was significantly lower than that induced by lobectomy. Within 2 months after surgery, segmentectomy spared 3–10% of initial FEV1, and after 12 months, 4–7% (difference between the loss induced by lobectomy and the loss induced by segmentectomy). Interestingly, results from a few studies suggest that this functional benefit may not translate into lower rates of post-operative complications, regardless of the procedure used, open [4, 8, 11, 14] or VATS [6, 20–22].
The magnitude of the difference in functional loss between segmentectomy and lobectomy, which might be regarded as mild to moderate and may be disappointing, leads us to consider two points. First, the term segmentectomy encompasses the resection of one or more segments, and, as previously highlighted, three studies found a relationship between the decrease in lung function and the number of resected segments. In some series, the number of segments resected during sublobar resections may have been close to that resected during lobectomies. Interestingly, Nomori et al. [12] compared the functional impact of the resection of <2 segments, ≥2 segments, the left upper division or the left upper lobe. The differences in loss of FEV1 between groups were significant, except between the left upper division and left upper lobectomy groups. Second, differences in compensatory adaption of the remaining lung after lobectomy and segmentectomy could explain differences between lung volume resection and lung function preservation [23, 24]. A better compensatory adaption of the remaining lung after lobectomy than after segmentectomy could reduce the functional benefit of segmentectomy. Ueda et al. [24] calculated CT-defined functional lung volume before and after lung resection. Lobectomy removed more functional lung volume than segmentectomy (24.5% versus 11.6%). However, the loss of functional lung volume after segmentectomy was not significantly different from that after lobectomy (8.3% versus 9.2%). Interestingly, the increase in both the ipsilateral and contralateral functional lung volume was more marked after lobectomy than after segmentectomy. The “function” of the segments rescued by segmentectomy decreased by 23% after surgery. Eventually, compensatory lung growth has also been discussed to explain the rather good compensatory adaptation after lobectomy [25, 26].
A low FEV1 is an independent predictive factor of complications, not only after major lung resection, but also after segmentectomy [27]. Surprisingly, while sublobar resections are recommended in patients with poor lung function, only three studies conducted specific functional studies in this high-risk population, including a total of 115 patients. Two of these studies showed that segmentectomy had better functional results than lobectomy [8, 11], whereas the third found no difference between the two procedures [7]. A mean gain in FEV1 of 12%, or 0.12 L, was described at 6 months in one series, the mechanism underlying this gain being unclear [11]. Interestingly, in a subgroup of patients with emphysema, an inverse relationship between the loss of FEV1 and the predicted post-operative FEV1 has been detected for lobectomy but not for segmentectomy [7]. The gain or at least the reduced loss in lung function induced by lobectomy in patients with severe emphysema may be attributable to a lung volume reduction effect [28]. The resection of an emphysematous segment, compared to that of a lobe, may not allow enough lung to expand after surgery to limit the functional loss. Taken as a whole, the results of these three studies do not firmly establish the functional benefit of segmentectomy over lobectomy in patients with poor lung function. Additional studies with a complete initial evaluation of lung function combined with lung imaging assessment may identify potential subgroups of patients who would benefit from either segmentectomy or lobectomy.
Eventually, the functional impact of open and VATS procedures should be discussed. In a recent series of 351 VATS lobectomies and segmentectomies, the decrease in pulmonary function at 12 months was low, the mean±sd loss of FEV1 being 6.9±10.3% and that of DLCO 6.9±14.8%. However, the results associated with segmentectomy were not individualised [29]. A multivariate analysis performed in a consecutive series of 228 segmentectomies showed that open surgery, versus thoracoscopy, was an independent predictive factor of post-operative complications [27]. VATS reduces the loss of lung function after lobectomy [30, 31], especially within the initial post-operative days, through decreased post-operative pain, improved chest wall mechanics and reduced inflammatory processes. These early days are regarded as critical determinants of post-operative morbidity and mortality [32, 33]. Large data-based series have indeed shown that VATS lobectomy can be performed with acceptable rates of morbidity and mortality in patients with predicted post-operative FEV1 or DLCO <40% or 60% [32, 34]. As suggested by three studies showing low functional loss after VATS segmentectomy [6, 9, 17], the functional benefit of segmentectomy may add to that of VATS. This needs to be confirmed in large series of patients, especially of patients with impaired lung function, and then may lead to a reconsideration of the lower functional limits for surgery.
Future prospects
Besides surgery, other treatment modalities such as stereotactic ablative body radiotherapy (SABR) and radiofrequency ablation (RFA) can be offered to patients with stage I lung cancer. No proper comparison of SABR and segmentectomy functional consequences can be performed because of the lack of randomised trials. Several studies report PFT measured before and after SABR, but a comparison with surgical series is hazardous because of strong differences in patient characteristics (patients in SABR studies are older and have more degraded lung function) and study design [35–54]. The SABR PFT results suggest that the mean loss of lung function may be lower after SABR than after segmentectomy, but this needs to be confirmed. In fact, SABR patients show a small decrease in FEV1 and DLCO during the first weeks, but a marked functional loss at 2 years. This contrasts with surgery, which is characterised by a maximal decrease in FEV1 and DLCO during the first weeks and a reduction of the loss several months after treatment [50, 54]. Another difference between surgery and SABR may be dispersion of the functional changes, which may be larger after SABR, a significant proportion of patients having improving lung function and another showing functional degradation. The occurrence rate of severe pulmonary toxicity after SABR, according to Common Terminology Criteria for Adverse Events (CTCAE) scoring, is low. Altogether, these data suggest that the functional tolerance of SABR, at least within the first months following radiotherapy, is quite good. However, whether SABR yields similar survival compared with surgical resection still remains to be established [55]. A potential flaw of SABR is indeed the lack of nodal dissection and sampling, which may lead to underestimation of the extent of disease.
A few PFT data from 135 lung cancer patients can be extracted from the RFA literature. Three studies found no significant change in mean forced vital capacity, FEV1 or DLCO until 12 months after RFA, but showed some dispersion of PFT values, like in SABR studies [56–58]. A fourth study found a significant but tiny reduction of PFT, the mean vital capacity 1 month and 3 months after RFA being at 93% and 95% of the baseline value [59]. Comparison of RFA with sublobar resection and SABR has been performed in two nonrandomised trials [40, 60], but patient characteristics, including baseline PFT, differed significantly and none of the studies reported post-RFA PFT. Positioning of the treatment modalities for stage I lung cancer will partly rely on their functional cost, which needs to be carefully evaluated.
Conclusions
The published studies show that the long-term reduction (≥12 months) in lung function induced by segmentectomy is very small, and a little smaller than that induced by lobectomy. However, this tiny difference may benefit lung cancer patients who may need subsequent lung resections. Within the 2 months after surgery, lung function reduction is mild to moderate, but also a little smaller than that induced by lobectomy. However, PFT monitoring within the early days after VATS segmentectomy, days that are critical determinants of post-operative morbidity, needs to be assessed. Two issues remain to be addressed: whether VATS segmentectomy may preserve lung function better than VATS lobectomy in patients with poor lung function, and whether this may translate into a lowering of the functional limit for surgery. In addition, the balance between benefits and risks related to sublobar resections and alternative therapeutic options such as SABR and RFA should be performed. One of the main problems is that implementation of randomised studies is quite impossible, the only few attempted having been prematurely closed due to poor recruitment [61, 62].
Footnotes
Conflict of interest: None declared.
Provenance: Submitted article, peer reviewed.
- Received July 7, 2017.
- Accepted August 3, 2017.
- Copyright ©ERS 2017.
ERR articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










