





Figures
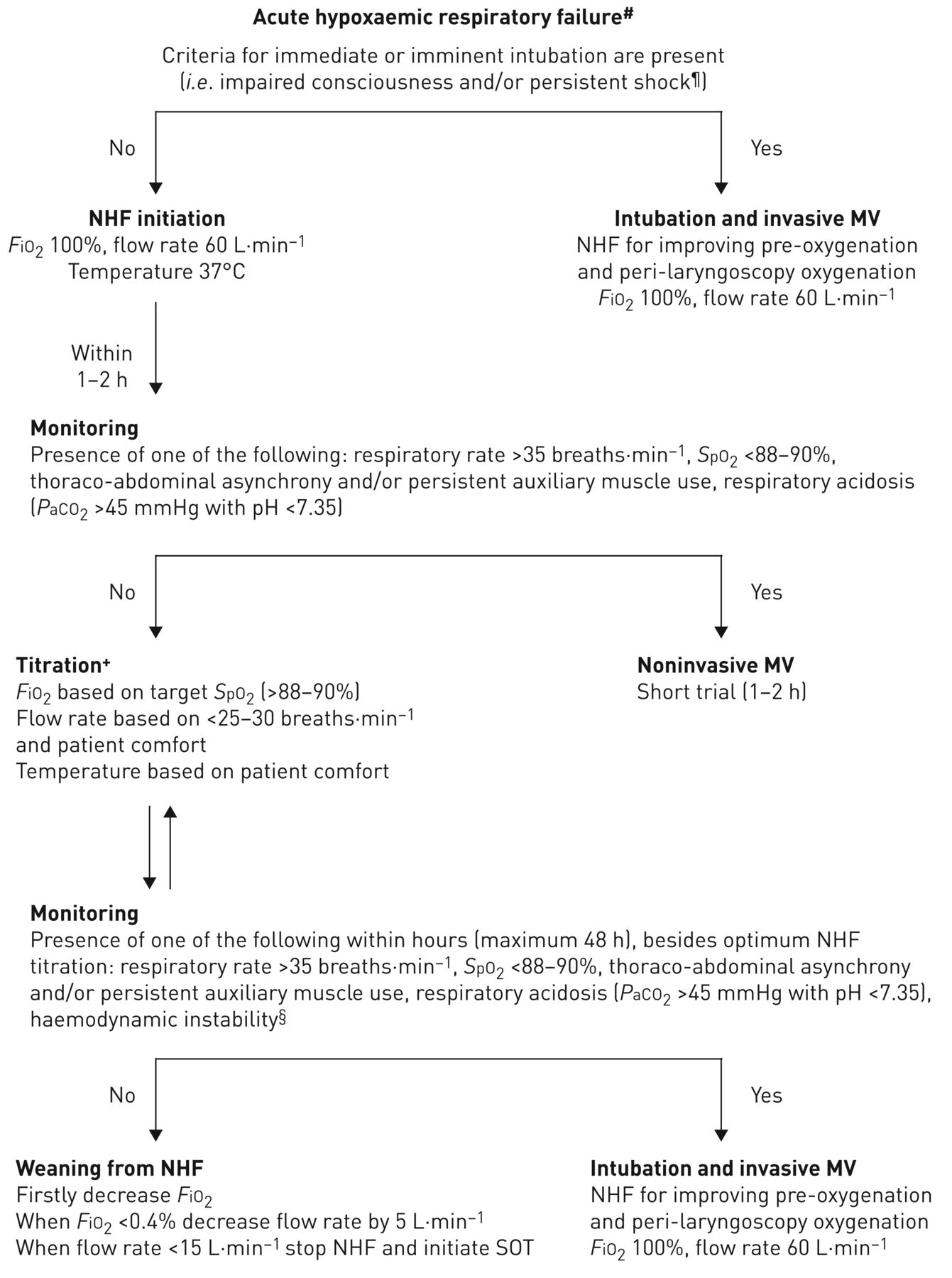
- FIGURE 1
Recommended algorithm for high-flow nasal cannula use in acute hypoxaemic respiratory failure in immunocompetent or immunocompromised patients. #: arterial oxygen tension (PaO2)/inspiratory oxygen fraction (FiO2) <300 (patients with arterial carbon dioxide tension (PaCO2) >45 mmHg and pH <7.35 are excluded); ¶: systolic arterial blood pressure <90 mmHg despite adequate fluid administration; +: the rationale for change in nasal high flow (NHF) settings are as follows. 1) Flow rate could be adjusted downwards by 5–10 L·min−1 per 1–2 h if none of the negative prognostic factors are present. However, if targets of arterial oxygen saturation measured by pulse oximetry (SpO2) and respiratory rate are not achieved, while the flow rate is <60 L·min−1, increase of flow rate by 5–10 L·min−1 is preferred to raising FiO2; 2) increase in FiO2 causes increases in PaO2 and SpO2; 3) temperature can be set at 37°C or lower (31–34°C), based on the patient's comfort; §: haemodynamic instability is defined by heart rate >140 beats·min−1 or change >20% from baseline and/or systolic arterial blood pressure >180 mmHg, <90 mmHg or decrease >40 mmHg from baseline. MV: mechanical ventilation; SOT: standard oxygen treatment.

{kind=link}
Tables
- TABLE 1
Relevant studies for nasal high flow (NHF) in patients with acute respiratory failure
Design Patients Results Benefit Lenglet et al. [19] Prospective, observational study 17 ARF patients on oxygen with a non-rebreathing face mask who switched to NHF NHF was associated with a significant decrease in dyspnoea, respiratory rate and a significant increase in SpO2 within the first 15 min of its application Roca et al. [22] Prospective, comparative study of sequential interventions 20 patients with hypoxaemic ARF received oxygen via face mask and NHF for 30 min each NHF was associated with less dyspnoea and mouth dryness and more comfort than face mask; it was also associated with higher PaO2 and lower respiratory rate, with no differences in PaCO2 Sztrymf et al. [23] Prospective observational study 38 ICU patients with ARF who received oxygen through NHF NHF was associated with a significant reduction in respiratory rate, heart rate, dyspnoea score, supraclavicular retraction and thoraco-abdominal asynchrony and a significant improvement in SpO2 Sztrymf et al. [24] Prospective observational study 20 patients with persistent ARF who received oxygen through NHF Use of NHF enabled a significant reduction of respiratory rate and a significant increase in oxygen saturation and PaO2 Frat et al. [26] Multicentre, open-label RCT 310 ARF patients admitted to ICU, randomly assigned to NHF, SOT or NIV ICU and 90-day mortality were significantly lower with NHF compared with SOT or NIV, although no significant difference in intubation rate was found between the three study groups. In the subgroup of patients with PaO2/FiO2 ≤200 the intubation rate was significantly lower with NHF Messika et al. [27] Prospective observational study Effectiveness and frequency of NHF use in patients with ARDS 29% of patients requiring noninvasive ventilatory support were treated via NHF as first-line treatment. Among them, the intubation rate was 40%. Haemodynamic failure was associated with NHF failure and intubation No benefit Jones et al. [31] Pragmatic open randomised controlled trial 303 ARF patients at emergency departments randomised to NHF or SOT There was no difference between the groups in NIV or intubation rate during the emergency department stay in mortality, on emergency department and hospital length of stay ARF: acute respiratory failure; SpO2: arterial oxygen saturation measured by pulse oximetry; PaO2: arterial oxygen tension; PaCO2: arterial carbon dioxide tension; ICU: intensive care unit; SOT: standard oxygen treatment; NIV: noninvasive ventilation; FiO2: inspiratory oxygen fraction; ARDS: acute respiratory distress syndrome.
- TABLE 2
Relevant studies for nasal high flow (NHF) use in intensive care unit (ICU) post-extubated patients
Design Patients Results Benefit Rittayamai et al. [34] Randomised, non-blinded, crossover study 17 successfully weaned patients received NHF for 30 min followed by SOT for another 30 min and vice versa Use of NHF was associated with significant reductions in dyspnoea, heart rate and breathing frequency compared with a non-rebreathing mask Maggiore et al. [35] Randomised, controlled, open-label trial 105 extubated patients with PaO2/FiO2 ≤300 randomised to either NHF or Venturi mask NHF in the post-extubation period resulted in better oxygenation for the same set FiO2, decreased respiratory rate, improved patient comfort, reduced episodes of oxygen desaturations and frequency of need for ventilator support of any kind Hernández et al. [38] Multicentre, randomised clinical trial 527 patients at low risk of post-extubation respiratory failure randomised to NHF or SOT after extubation NHF in comparison with SOT resulted in less post-extubation respiratory failure (8.3% versus 14.4%) and lower re-intubation rate (4.9% versus 12.2%) No benefit Tiruvoipati et al. [39] Randomised crossover study 50 extubated patients received either NHF followed by high-flow face mask for 30 min each or vice versa No significant difference in gas exchange, respiratory rate or haemodynamics was observed between groups. Tolerance was significantly better with NHF Hernández et al. [40] Multicentre, prospective cohort study 604 patients at high risk of post-extubation respiratory failure randomised to NHF or NIV after extubation NHF had similar re-intubation rates and median time to re-intubation with NIV. ICU length of stay was lower in the NHF group SOT: standard oxygen treatment; PaO2: arterial oxygen tension; FiO2: inspiratory oxygen fraction; NIV: noninvasive ventilation.
- TABLE 3
Relevant studies for nasal high flow (NHF) use in post-extubated patients following surgery
Design Patients Results Benefit Corley et al. [5] Prospective interventional study 20 patients post-cardiac surgery with ARF under SOT and then NHF Compared with SOT, NHF increased mean Paw by 3.0 cmH2O, expiratory lung volume by 25.6% and tidal volume by 10.5%. Patients with higher BMI had larger increases in end-expiratory lung volume Parke et al. [25] Prospective randomised comparative study 56 postoperative patients with ARF, randomised to NHF or to high-flow face mask Significantly more NHF patients succeeded with their allocated therapy. Patients in the NHF group tended to need NIV less frequently than the high-flow face mask group and had significantly fewer desaturations Parke et al. [45] Pragmatic, open-label randomised controlled trial 340 post-cardiac surgery patients randomised to NHF or SOT after extubation No differences in SpO2/FiO2 ratio at day 3 or in-hospital and ICU length of stay and mortality at day 28 were observed between the two study groups. NHF reduced the requirement for escalation of respiratory support No benefit Corley et al. [46] Randomised controlled trial 155 patients post-cardiac surgery with BMI ≥30 kg·m−2 randomised to NHF or SOT No difference was seen between groups in atelectasis scores on day 1 or 5, in mean PaO2/FiO2 ratio or respiratory rate in the first 24 h post-extubation and the length of ICU stay Stéphan et al. [52] Multicentre, randomised, unblinded noninferiority trial BiPAP or NHF in 830 cardiothoracic patients who developed ARF after extubation or with pre-existing risk factors for post-extubation ARF NHF was non-inferior to BiPAP in treatment failure, defined as re-intubation for mechanical ventilation, switch to the other study treatment or premature study treatment discontinuation. No significant differences were found in ICU mortality Ansari et al. [53] Randomised, controlled, blinded study 59 post-elective lung resection surgery patients randomised to NHF or SOT Similar results were observed in the difference between pre-operative and postoperative 6-min walk test and spirometry between the two study groups. Length of hospital stay was significantly lower in the NHF group Futier et al. [54] Multicentre, randomised controlled trial 220 post-abdominal surgery patients randomised to NHF or SOT No differences for postoperative hypoxaemia, pulmonary complications or length of hospital stay were found between the two groups studied ARF: acute respiratory failure; SOT: standard oxygen treatment; Paw: airway pressure; BMI: body mass index; NIV: noninvasive ventilation; SpO2: arterial oxygen saturation measured by pulse oximetry; FiO2: inspiratory oxygen fraction; ICU: intensive care unit; BiPAP: bi-level positive airway pressure.
- TABLE 4
Relevant studies for nasal high flow (NHF) use in immunocompromised patients with acute respiratory failure (ARF)
Design Patients Results Benefit Coudroy et al. [69] Retrospective observational study 115 immunocompromised patients with ARF treated with NIV or NHF The NHF group had significantly lower rates of intubation and mortality in the ICU and at day 28 than the NIV group Frat et al. [70] Post hoc analysis 82 immunocompromised patients with ARF treated with NIV, NHF or SOT The NHF group had significantly lower rates of intubation and mortality than the NIV group. No significant difference in intubation and mortality rates was noted between SOT and NHF Mokart et al. [71] Retrospective propensity-score analysis 178 cancer patients with severe ARF received oxygen through SOT, NHF or through the combinations NHF–NIV or SOT–NIV Compared to the other patients, patients who received NHF–NIV combination presented a lower day-28 mortality rate, a longer time from ICU admission to intubation and a higher, but not significant number of ventilator-free days. NHF–NIV was independently associated with improved survival Epstein et al. [72] Retrospective 183 cancer patients with hypoxia treated with NHF 41% improved while on the device, 44% remained stable and 15% declined. The device was well tolerated with few complaints Lee et al. [73] Retrospective 45 patients with haematological malignancies who developed ARF 20% of the patients showed a good response to NHF therapy while the remaining 80% of patients failed to respond to the initial NHF therapy requiring intubation with mechanical ventilation, NIV or narcotic palliation alone Roca et al. [74] Retrospective 37 lung transplant recipients with ARF who received NHF or SOT Absolute risk reduction for mechanical ventilation with NHF therapy was 29.8% and the NNT to prevent one intubation with NHF was 3. NHF therapy was associated with a decreased risk of mechanical ventilation No benefit Lemiale et al. [75] Prospective, multicentre, parallel-group RCT 100 immunocompromised patients with ARF, randomised to NHF or SOT No significant difference regarding the need for invasive ventilation/NIV during the 2-h study period. Additionally, no significant difference reported regarding dyspnoea score, respiratory rate and heart rate Harada et al. [76] Retrospective 56 patients with haematological malignancies with ARF under NHF treatment 20% responded well to NHF therapy, while 80% failed, and they underwent a second-line therapy with invasive mechanical ventilation, NIV or narcotic palliation NIV: noninvasive ventilation; ICU: intensive care unit; SOT: standard oxygen treatment; NNT: number needed to treat; RCT: randomised controlled trial.










