





Abstract
Bleeding is one of the most feared complications of flexible bronchoscopy. Although infrequent, it can be catastrophic and result in fatal outcomes. Compared to other endoscopic procedures, the risk of morbidity and mortality from the bleeding is increased, as even a small amount of blood can fill the tracheobronchial tree and lead to respiratory failure. Patients using antithrombotic agents (ATAs) have higher bleeding risk. A thorough understanding of the different ATAs is critical to manage patients during the peri-procedural period. A decision to stop an ATA before bronchoscopy should take into account a variety of factors, including indication for its use and the type of procedure. This article serves as a detailed review on the different ATAs, their pharmacokinetics and the pre- and post-bronchoscopy management of patients receiving these medications.
Abstract
A thorough understanding of antithrombotic agents is critical to manage patients in the peri-bronchoscopic period http://ow.ly/zcqn30bRCjf
Introduction
A bronchoscopist is often involved in the management of antithrombotic agents (ATAs) in the peri-procedural period. Patients are prescribed these medications for a variety of indications, and the decision to withhold them prior to bronchoscopy can be challenging. The increasing number of novel oral anticoagulants (also known as direct oral anticoagulants or target-specific oral anticoagulants), with different pharmacokinetics and safety profiles, has made these decisions more complex. The recent American College of Chest Physicians (ACCP) guidelines emphasising the use of direct thrombin or factor Xa inhibitors over vitamin K antagonists for atrial fibrillation, deep vein thrombosis (DVT) and pulmonary embolism (PE) in non-cancer patients [1] will certainly result in their increasing use. With more patients being prescribed newer ATAs, it is imperative for a bronchoscopist to have a thorough knowledge of these drugs. During the peri-procedural management of ATAs, one has to weigh up several clinical factors (table 1): the invasiveness of the procedure, patient-related risk factors, the indication for antithrombotic therapy and the need for bridging. The pharmacokinetics and other properties of the individual ATAs, which are broadly classified into antiplatelet agents and anticoagulants, will also influence the management of antithrombotic therapy. All these factors will be discussed in this review.
Factors influencing antithrombotic therapy during the peri-bronchoscopic period
Invasiveness of the procedure and patient-related risk factors
The data for bleeding risks associated with different types of bronchoscopic procedure are scant. Bleeding rates vary by the type of bronchoscopic procedure performed [2–5]. Cordasco et al. [2] noted that the rate of bleeding was related to the type of biopsy performed, with transbronchial biopsy carrying a much higher risk than endobronchial biopsy. The authors reported an overall bleeding rate of 0.83% with flexible bronchoscopy and 1.9% if either brushing or biopsy was performed. In a prospective multicentre study involving 20 986 bronchoscopies, Facciolongo et al. [3] reported different rates of bleeding with various bronchoscopic procedures. Transbronchial biopsy was associated with the highest rates of bleeding complications, followed by therapeutic bronchoscopy (which entails the use of Nd:YAG laser, argon-plasma, electrocautery and stent positioning), endobronchial biopsy, transbronchial needle aspiration (TBNA), bronchoalveolar lavage and explorative bronchoscopy, which had the lowest rates of bleeding complications. Thus, transbronchial biopsy and therapeutic bronchoscopy are considered to be relatively high-risk procedures, while explorative bronchoscopy with or without bronchoalveolar lavage and endobronchial needle aspiration are low-risk interventions (table 2). In the latter category, although discontinuation of ATAs is recommended in most instances, exceptions can be made depending on the skill and experience of the bronchoscopist, the capabilities of the centre in managing life-threatening bleeding and when the situation presents itself as emergent. It must, however, be noted that the decision should be individualised, and bleeding can ensue with any procedure, even those with minimal risk. Hence, the best clinical and procedural skills should be practised. Additionally, patient-related risk factors can independently increase the risk of bleeding. These risk factors include uraemia, thrombocytopenia, HIV/AIDS, solid-organ transplant, haematological disorders and thrombocytosis [2, 6]. Evidence is currently lacking on the effect of bleeding risk when multiple risk factors present in combination. In these situations, coagulation parameters, platelet counts and blood urea levels should be routinely monitored, and therapeutic intervention should be attempted to reverse coagulopathy in the form of fresh frozen plasma (FFP), platelet transfusions and desmopressin, if necessary [2].
Invasiveness of bronchoscopic procedures based on relative bleeding rates
Indication for the use of ATAs
The bronchoscopist must consider the rationale behind the use of ATAs prior to their discontinuation. In some instances, the risks of thromboembolic events can outweigh the risk of bleeding. The most common indications for their use are acute coronary syndrome (ACS), non-valvular atrial fibrillation, metallic heart valves, percutaneous coronary intervention (PCI), PE and DVT.
In patients with non-valvular atrial fibrillation, the risk of stroke can be determined using CHADS₂ [7] and CHA₂DS₂-VASc [8] scores (table 3). Patients with valvular atrial fibrillation are at much higher risk of thromboembolic events [9]. For patients with mechanical heart valves, the risk for thromboembolic events is based on their type, number and location. Metallic valves in the mitral position have the highest risk for arterial thromboembolic events [9, 10]. The decision to perform bronchoscopy with transbronchial biopsy in patients with recent ACS or coronary stent insertion should take into account the time since the most recent ACS, the type of stent (bare metal stent (BMS) versus drug-eluting stent (DES)) and the time since its insertion. In fact, the strongest predictor of stent thrombosis among patients receiving more than one ATA is premature discontinuation of dual-antiplatelet therapy (DAPT) (within 6 weeks of BMS insertion and 6 months of DES insertion) [11].
Comparison of CHADS2 versus CHA2DS2-VASc scoring systems
According to current guidelines, DAPT should be continued in patients with stable ischaemic heart disease for at least 1 month after a BMS is implanted and for at least 6 months after a DES is implanted (class of recommendation: I); a longer duration of DAPT is recommended in these patients if they are not at high risk of bleeding and able to tolerate DAPT without bleeding complications (class of recommendation: IIb) [12].
Need for bridging
When a long-acting ATA is withheld during the peri-procedural period, short-acting antiplatelet agents such as glycoprotein IIb/IIIa inhibitors or anticoagulants such as unfractionated heparin and low-molecular-weight heparin (LMWH) products may be recommended during the interruption period (bridging). At present, the recommendations regarding the need for bridging in patients with atrial fibrillation are inconsistent. Moreover, data on the short-term risk of thromboembolic events during the peri-procedural interruption period vary between published studies. Raunso et al. [13] found a significant increase in short-term (90-day) risk of thromboembolic events or death when warfarin was interrupted in patients with atrial fibrillation, while Douketis et al. [14], in the “bridge trial”, noted that no bridging was non-inferior to bridging in the prevention of arterial thromboembolism in patients with atrial fibrillation. Douketis et al. [14] also reported that bridging was associated with three times the risk for major bleeding. We recommend that bridging should be reserved for patients with high venous and arterial thromboembolic risk [14–16]. Additionally, current evidence does not recommend bridging for low- and moderate-risk patients, and the decision should be individualised based on the patient's risk factors and procedure-related factors (table 4) [17]. The bridging protocol is described in table 5.
Risk for thromboembolic events during the interruption period of antithrombotics
Bridging for warfarin and P2Y12 receptor blockers
Antiplatelet drugs
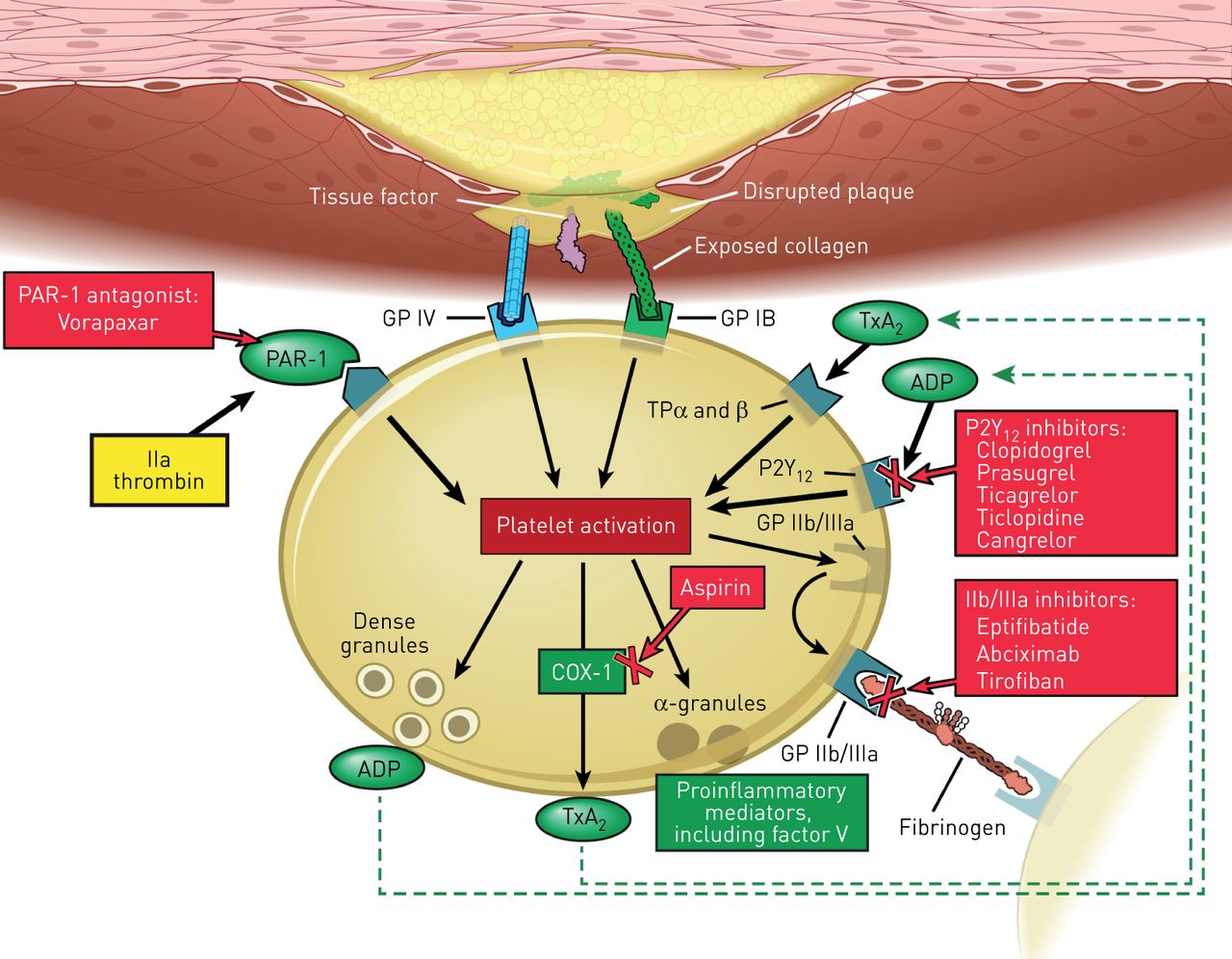
Antiplatelet drugs are grouped into various subclasses based on their mechanism of action. These are described in detail in the following sections and summarised in table 6 and figure 1.
Management of antiplatelet agents in the peri-bronchoscopic period
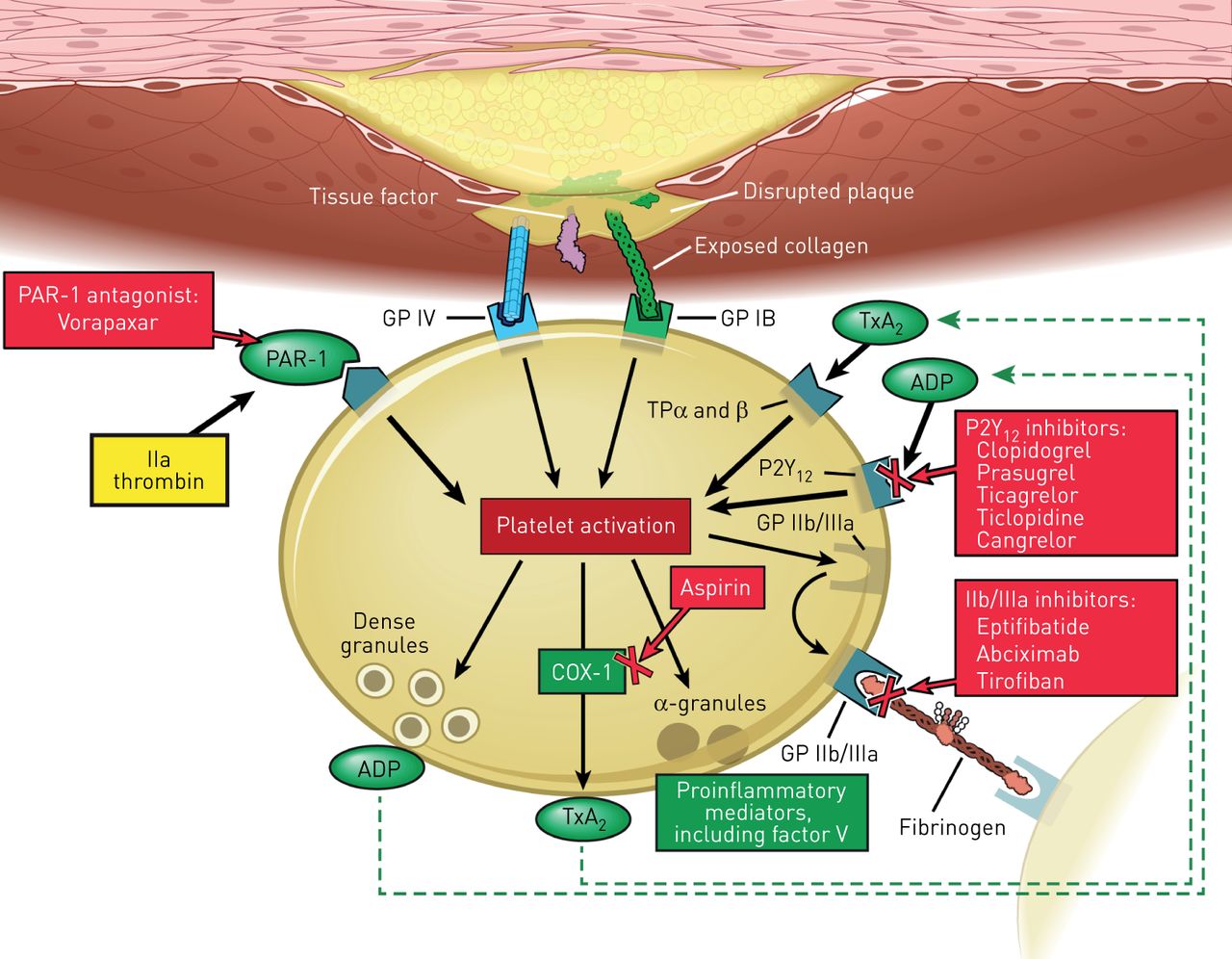
Mechanism and site of action of antiplatelet agents. COX-1: cyclooxygenase-1; GP: glycoprotein; PAR-1: protease-activated receptor 1; TP: thromboxane prostanoid; TxA2: thromboxane A2. Reprinted with permission, Cleveland Clinic © 2016–2017. All rights reserved.
Irreversible cyclooxygenase inhibitors
Aspirin (salicylate)
Aspirin is the most commonly used antiplatelet agent. Aspirin irreversibly blocks the enzyme cyclooxygenase-1 enzyme and interrupts the first step in the prostaglandin and thromboxane A2 synthesis pathway, thereby inhibiting platelet aggregation. Aspirin's maximal antiplatelet effect occurs within minutes and lasts through the life of the platelets (5–7 days) [18–20].
Current evidence does not suggest any increased risk of bleeding with singular use of aspirin. Zakaria and Abdel-Fattah [21] found no association between the use of aspirin and the increased bleeding risk after transbronchial biopsy. Herth et al. [22] concluded that the use of aspirin was not associated with increased risk of bleeding and the recommendation was to not stop aspirin prior to bronchoscopy.
Monitoring of the aspirin antiplatelet effect is generally not indicated. Additionally, blood testing for monitoring purposes has not been shown to correlate with clinical outcomes [23]. Due to its irreversible effect on platelets, bleeding complications can be controlled with platelet transfusions.
P2Y12 receptor blockers
Thienopyridines
Clopidogrel (Plavix)
Active metabolites of clopidogrel irreversibly bind to the platelet P2Y12 receptor, thereby inhibiting ADP-induced platelet activation and aggregation. The onset of action is dose dependent. Maximum platelet inhibition takes 5–10 days with a maintenance dose of 75 mg·day−1, as compared to 12–15 h after a loading dose of 300–600 mg [24–26]. Clopidogrel is commonly used as part of DAPT, in combination with aspirin in the management of ACS, recent myocardial infarction or stroke, or established peripheral arterial disease [27].
The decision to stop clopidogrel prior to the bronchoscopic procedure can be challenging, especially when there is an increased risk for thromboembolic events such as in-stent thrombosis and death. The 2012 ACCP guidelines recommend delaying surgical procedures for at least 6 weeks after BMS insertion and for at least 6 months after DES [17]. DAPT is associated with significant increase in bleeding, as evidenced by the CURE (Clopidogrel in Unstable Angina to Prevent Recurrent Events) trial [28]. The rate of spontaneous major bleeding over a 9-month follow-up period was 3.7% with DAPT versus 2.7% with aspirin monotherapy, and 5.1% versus 2.4% for spontaneous minor bleeding, respectively.
Ernst et al. [29] evaluated the safety of performing transbronchial biopsy in patients receiving clopidogrel. The study was stopped early because of the high bleeding rate in the clopidogrel-only group (89%; p<0.001). It also showed a 100% bleeding rate in the group receiving a combination of clopidogrel and aspirin (p<0.001). The authors suggested stopping clopidogrel 5–7 days prior to transbronchial biopsy. Stather et al. [30] evaluated the safety of endobronchial ultrasound-guided TBNA (EBUS-TBNA) in patients taking clopidogrel. They identified 12 cases with no significant bleeding and hence suggested that EBUS-TBNA can be performed safely in patients taking clopidogrel. However, due to the limitations of the retrospective nature of the study and the small study sample, they recommended continuing clopidogrel through the procedure only if the risk of short-term thrombosis outweighed the risk of bleeding.
Clopidogrel's antiplatelet effect is not routinely monitored and there are no standardised tests.
Prasugrel (Effient)
Prasugrel irreversibly inhibits platelet aggregation by blocking the P2Y12 receptor. In contrast to clopidogrel, prasugrel has more rapid absorption and onset of action, reaching its peak plasma concentration within 30 min. Its active metabolite has an average elimination half-life of 7 h and is mainly cleared by the kidneys [20, 31]. It is indicated for the reduction of thrombotic events in patients with ACS who are to be managed with PCI. Compared to clopidogrel, it has a significantly lower risk of stent thrombosis (1.1% versus 2.4%; p<0.001) but an increased risk of bleeding (major bleeding not related to coronary-artery bypass grafting 2.4% versus 1.8%; p=0.03) [32].
Recommendations for the peri-procedural management of prasugrel are identical to that for clopidogrel [20]. Due to its irreversible inhibitory effect on platelets, treatment of bleeding can be achieved by platelet transfusions.
Ticlopidine (Ticlid)
Ticlopidine is an oral irreversible inhibitor of ADP-induced platelet aggregation. It can reach its peak plasma concentration within 1–3 h after a single oral dose of 250 mg and has a half-life of 4–5 days after chronic usage [33]. Although studies on ticlopidine show benefit when used for stroke prevention and coronary stent occlusion, it is used rarely due to its potential serious side-effects, thrombocytopenia and neutropenia [34]. It can be continued throughout the peri-procedural period if the bronchoscopic procedure is considered a low risk and discontinuation of ticlopidine has a higher risk of thromboembolic events. It should be stopped 10–14 days prior to high-risk procedures in patients with low risk for thromboembolic events [35].
ADP receptor antagonists
Cangrelor (Kengreal)
Cangrelor is an intravenous rapidly acting reversible inhibitor of the P2Y12 receptor with a half-life of 3–6 min. Due to its reversible effect, normalisation of its antiplatelet effect occurs within 60 min of discontinuation. Its efficacy has been evaluated for use in the peri-procedural period during PCI [36].
Cangrelor can be stopped as early as 1–2 h prior to bronchoscopic procedures and can be used to bridge patients on the oral P2Y12 receptor blockers in whom prolonged discontinuation is needed prior to surgical intervention [37].
Ticagrelor (Brilinta)
Ticagrelor is a cyclopentyltriazolopyrimidine and an oral reversible P2Y12 ADP-receptor blocker. It is indicated for use in patients with ACS, it has a more potent antiplatelet activity than clopidogrel with a lower rate of stent thrombosis (1.3% versus 1.9%; p=0.009) and a nonsignificant difference in the rate of major bleeding [38, 39]. The drug has predictable pharmacokinetics with linear dose-related increases in plasma concentration, achieving its peak effect within 2–4 h after dosing [40, 41].
Similar to prasugrel, ticagrelor should be stopped 5–7 days prior to bronchoscopy and can be restarted within 24–48 h of the procedure [20, 25].
PAR-1 antagonists
Vorapaxar (Zontivity)
Vorapaxar is a potent orally active thrombin receptor (protease-activated receptor 1 (PAR-1)) antagonist. It is indicated for the reduction of thrombotic cardiovascular events in patients with a history of myocardial infarction or peripheral arterial disease [42]. It has a half-life of 5–13 days. After a single dose of vorapaxar, platelet function is not restored for 2–3 weeks [43]. Based on its prolonged half-life, it should be stopped at least 2 weeks prior to the bronchoscopic procedure.
Phosphodiesterase inhibitors: quinolone derivatives
Cilostazol (Pletal)
Cilostazol is a phosphodiesterase-3 inhibitor with vasodilatory, antiproliferative and reversible antiplatelet activity with a half-life of 11 h (longer in patients with renal impairment) [44]. It is approved for moderate to severe intermittent claudication for patients with peripheral arterial disease [45].
Having a relatively shorter half-life compared to the other antiplatelet drugs, it should be stopped 1–2 days prior to the bronchoscopic procedure.
Dipyridamole (Persantine)
Dipyridamole is phosphodiesterase inhibitor with vasodilatory and reversible antiplatelet effects. It produces sustained platelet inhibition via multiple mechanisms, including increasing cAMP inhibition of nucleotide phosphodiesterase and blockade of adenosine uptake, causing increase in the amount of adenosine at the platelet vascular interface. It can cause vasodilation at high doses [46]. It is used in conjunction with aspirin for the prevention of cerebral ischaemic events in patients with non-cardioembolic transient ischaemic attacks or strokes [47, 48].
The drug is excreted in bile and has a terminal half-life ranging between 10 h and 19 h [20, 25]. It should be stopped within 1–2 days prior to the bronchoscopic procedure.
Glycoprotein IIb/IIIa inhibitors
These intravenously administered antiplatelet agents include abciximab, eptifibatide and tirofiban. They inhibit platelet aggregation and thrombus formation and have proven of benefit in patients with ACS undergoing PCI [49–51]. Bleeding and thrombocytopenia are potential side-effects of these antiplatelet drugs [52, 53]. In addition, spontaneous alveolar haemorrhage has been reported as a rare side-effect (0.5–0.9%) [54–57]. Based on their pharmacokinetics and current guidelines, eptifibatide and tirofiban should be discontinued for at least 2–4 h before bronchoscopic procedures, whereas abciximab should be withheld for at least 12 h [58].
Abciximab (ReoPro)
Abciximab is a chimeric monoclonal antibody-binding fragment specific for platelet glycoprotein IIb/IIIa receptors. It has a rapid onset of action, with slow recovery of platelet function after discontinuation compared with the other glycoprotein IIb/IIIa inhibitors. It has a half-life of 10–30 min [25].
Eptifibatide (Integrilin)
Eptifibatide is a cyclic heptapeptide that binds to platelet glycoprotein IIb/IIIa receptors. It has a rapid onset of action and rapid reversal of platelet function with a half-life of 2.5 h, which can become prolonged in patients with renal disease [25, 59].
Tirofiban (Aggrastat)
Tirofiban is a non-peptide tyrosine derivative glycoprotein IIb/IIIa receptor inhibitor. Similar to eptifibatide, it has a rapid onset of action and rapid recovery of platelet function after discontinuation with a half-life of 2 h [60]. Dose adjustment is required in patients with impaired renal function [61].
Anticoagulant drugs
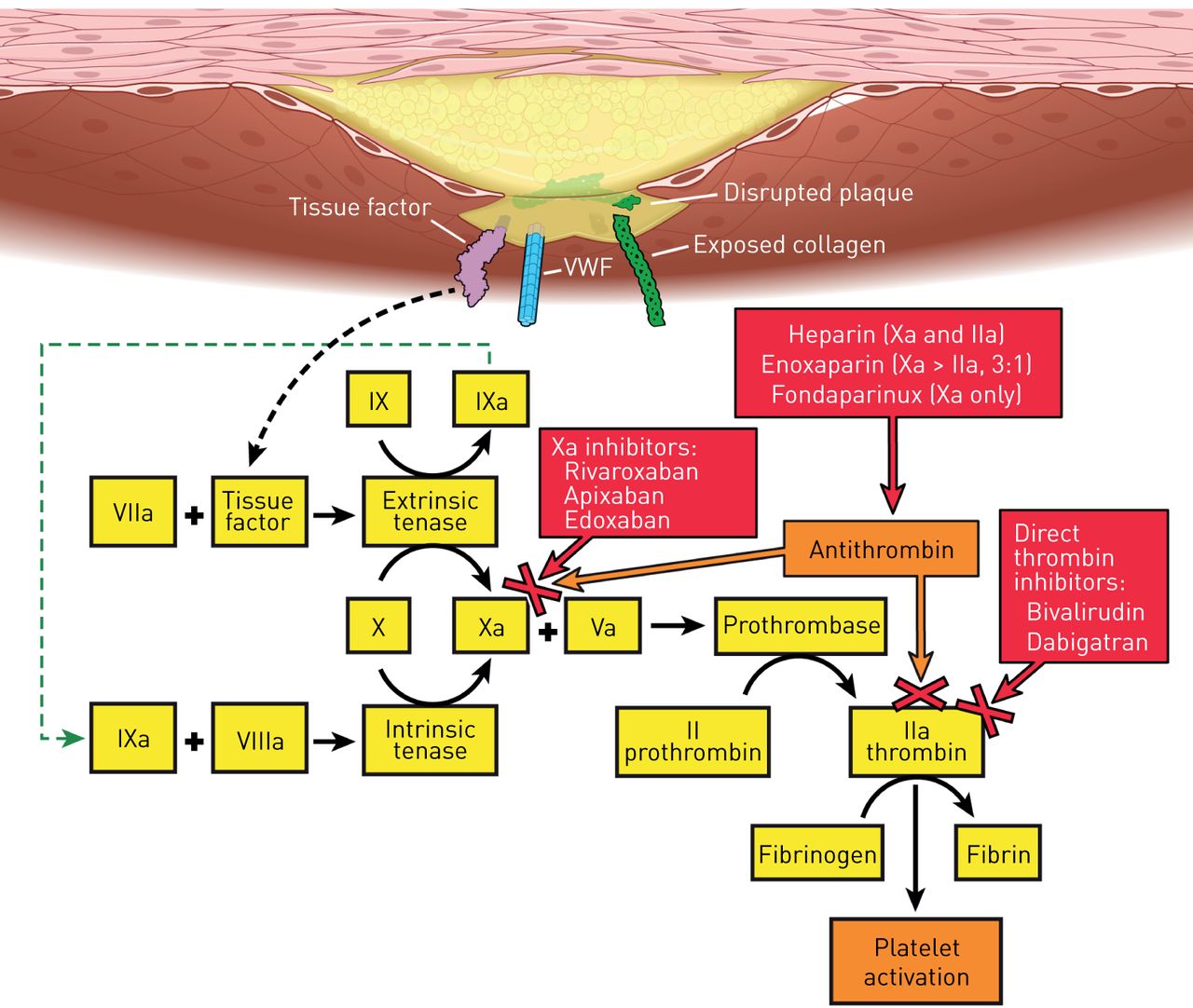
Anticoagulant drugs are likewise grouped into various subclasses based on their mechanism of action. These are described in detail in the following sections and summarised in table 7 and figure 2.
Management of anticoagulant agents in the peri-bronchoscopic period
{kind=link}
{kind=link}
Coagulation cascade and site of action of anticoagulant agents. VWF: von Willebrand factor. Reprinted with permission, Cleveland Clinic © 2016–2017. All rights reserved.
Oral anticoagulants
Vitamin K antagonists
Warfarin, acenocoumarol, phenindione and phenprocoumon constitute the vitamin K antagonists and act by inhibiting the production of vitamin K-dependent clotting factors II, VII, IX and X. In addition, they inhibit the carboxylation of the regulatory anticoagulant proteins C, S and Z [62, 63].
Warfarin (Coumadin)
Warfarin is the most commonly used oral anticoagulant. Drug–drug interactions and dietary restrictions are major drawbacks for its use. It is indicated for the primary and secondary prevention of venous thromboembolic diseases, for anticoagulation in atrial fibrillation and mechanical heart valves [64]. Warfarin should be stopped 5 days before bronchoscopic procedures and can be safely resumed within 12–24 h after bronchoscopy [65].
The prothrombin time and the international normalised ratio (INR) monitor its antithrombotic effects. In patients with impaired liver function, the use of the INR can be misleading. Checking the INR value 7 days before bronchoscopy is recommended to allow adequate time for planning of peri-bronchoscopic management. Rechecking the INR the day before surgery is suggested by multiple studies to allow correction with vitamin K supplementation and to avoid delaying the procedure [17, 66, 67].
The management of complications can be guided by the clinical scenario (urgent versus elective procedure). Multiple reversal strategies have been proposed, including the interruption of treatment, administration of vitamin K (oral or parenteral phytonadione, keeping in mind that the parenteral route should be reserved for patients in whom the risk is justified), FFP, prothrombin complex concentrate (PCC) or recombinant activated factor VII (rFVIIa) [68–70].
In situations where life-threatening bleeding has occurred and an immediate reversal of the anticoagulant effect of warfarin is needed, PCC has been shown in a randomised clinical trial to be non-inferior when compared with the traditional use of FFP to achieve haemostasis, and was associated with more rapid INR reduction [71]. Moreover, the use of FFP has its own drawbacks when compared with PCC; for example, FFP entails the use of larger volumes to achieve haemostasis, which may compromise the respiratory status and put certain patients at risk for transfusion-associated circulatory overload.
New oral anticoagulants
Due to the major drawbacks of vitamin K antagonists, more emphasis is being put on the use of newer oral anticoagulants such as the direct thrombin inhibitors and factor Xa inhibitors. These anticoagulants have been shown to be more effective in managing certain thromboembolic events, with fewer side-effects [72]. The use of these drugs over vitamin K antagonists for lower-extremity DVT or PE in non-cancer patients has been recommended by the recent ACCP guidelines [1].
Direct thrombin inhibitors
Dabigatran (Pradaxa)
Dabigatran is an oral, selective, reversible direct thrombin inhibitor. It is metabolised by the liver and eliminated by renal excretion. Its indications include the treatment and prevention of venous thromboembolism (VTE) and the prevention of stroke and arterial embolism in patients with non-valvular atrial fibrillation [73, 74]. Dose adjustment is needed in patients with a creatinine clearance of <30 mL·min−1 or in patients on selective glycoprotein IIb/IIIa inhibitors. Its use should be avoided in patients with advanced liver disease.
The half-life of dabigatran in plasma is 15 h and its time to peak effect is 2 h. Current recommendations are to stop dabigatran 1–2 days prior to procedures in patients with creatinine clearance >50 mL·min−1 and 3–5 days with creatinine clearance <50 mL·min−1 (longer if major bleeding is expected). Dabigatran can be safely restarted within 24 h after bronchoscopy if haemostasis is achieved. No monitoring is required [75].
An advantage of dabigatran is the availability of an antidote, idarucizumab, which can completely and rapidly reverse the anticoagulant effect of dabigatran; this received approval from the US Food and Drug Administration (FDA) in 2015 [76]. Dialysis is an another option for the management of dabigatran-induced bleeding [77].
Factor Xa inhibitors
Apixaban (Eliquis)
Apixaban is an oral, selective, reversible, direct factor Xa inhibitor. It is indicated for reducing the risk of stroke and systemic embolism in non-valvular atrial fibrillation, the treatment and prevention of DVT and PE, as well as prophylaxis of DVT following hip or knee replacement surgery. Apixaban undergoes hepatic metabolism with partial renal excretion. Dosage adjustment is recommended for renal disease as well as in patients aged ≥80 years, with body weight ≤60 kg or serum creatinine ≥1.5 mg·dL−1. It should be avoided in advanced liver disease. Apixaban has an approximate plasma half-life of 12 h, and reaches its peak effect at 3 h.
Edoxaban (Savaysa)
Edoxaban is a once-daily administered, rapidly acting direct factor Xa inhibitor. It has a similar safety and adverse reaction profile to other medications in this group. Its half-life is 12 h and peak time to onset is 2 h. It is indicated for the treatment of DVT and PE following 5–10 days of initial therapy with a parenteral anticoagulant [78]. It is also indicated for patients with non-valvular atrial fibrillation [79]. Dose adjustments are needed if a patient's creatinine clearance is 15–50 mL·min−1, if the patient weighs <60 kg and with the use of selective glycoprotein IIb/IIIa inhibitors. It is also recommended that edoxaban should not be used in patients with a creatinine clearance >95 mL·min−1 because of the increased risk of ischaemic stroke.
Rivaroxaban (Xarelto)
Rivaroxaban is an oral, selective and competitive active-site-directed, reversible factor Xa inhibitor; it has a predictable dose-dependent effect without the need for laboratory monitoring. It undergoes hepatic metabolism and partial renal excretion. It should be used cautiously in renal and liver disease patients.
Controlling bleeding
Along with the usual bronchoscopic manoeuvres to control bleeding, current measures include the use of activated and non-activated PCCs and rFVIIa [80–82]. In addition, andexanet alfa is a new antidote for factor Xa inhibitors [83]. In a multicentre, prospective study evaluating 67 patients who developed acute major bleeding after 18 h of using factor Xa inhibitors (apixaban, rivaroxaban, edoxaban or enoxaparin), it was shown that andexanet alfa can rapidly reverse their anticoagulant effect and achieve effective haemostasis in 79% of patients after 12 h of administration [84]. However, it should be noted that andexanet alfa has yet to be approved for use in the USA by the FDA.
Factor Xa inhibitors should be stopped 1–2 days before bronchoscopy (longer in patients prone to bleeding complications) and can be restarted within 24 h of bronchoscopy if haemostasis is achieved. However, the decision to restart these anticoagulants should be individualised based on the nature of the procedure performed and the risk of thromboembolic events.
Parenteral anticoagulants
Unfractionated heparin
Heparin is the most commonly used parenteral anticoagulant. It is indicated for primary and secondary prevention of VTE, ACS, mechanical heart valves, atrial fibrillation and for bridging from and to long-acting oral anticoagulants. Heparin binds to antithrombin, leading to conformational structural changes converting antithrombin from a slow thrombin inhibitor to a rapid inhibitor. In addition, it inhibits activated coagulation factors IX, X, XI, XII and plasmin, as well as the conversion of fibrinogen to fibrin [85, 86].
Unfractionated heparin has a half-life of 60–90 min and should be stopped 4–6 h prior to the bronchoscopic procedure when used intravenously. Discontinuing the drug for a longer period is suggested if major bleeding is expected [87, 88]. Heparin can be restarted 12–24 h post-bronchoscopy in intermediate- to high-risk procedures and sooner (4–6 h, preferably without a bolus) if the procedure was low-risk and intra-procedural haemostasis was achieved. Heparin's anticoagulant response varies among patients, so the need to monitor is of great significance. The activated partial thromboplastin time (APTT) or an anti-Xa assay is used to monitor the effect and adjust the dose of heparin [89, 90]. In addition to general measures for bleeding control, intravenous protamine sulfate at 1 mg per 100 circulating heparin units can rapidly reverse its anticoagulant effects [91, 92].
Low-molecular-weight heparin
Enoxaparin (Lovenox), dalteparin and tinzaparin are LMWH products available in the USA. They have smaller molecular weights than heparin, have a reduced inhibitory effect on thrombin, and have more selectivity to bind antithrombin than other plasma proteins [93].
LMWH products have multiple indications, including prophylaxis and treatment for VTE, especially in cancer patients, ACS and for bridging to and from the new oral anticoagulants and vitamin K antagonists [1, 94–96]. They have a more predictable dose–response relationship, longer half-life, and less incidence of heparin-induced thrombocytopenia (HIT) and bone loss compared to unfractionated heparin [97, 98]. The half-life of enoxaparin is 3–5 h, which can be prolonged in patients with renal impairment due to its renal elimination [99]. Dose adjustment is necessary for patients with a creatinine clearance <30 mL·min−1.
Due to their predictable effect, routine laboratory monitoring is not indicated (exceptions are obesity, pregnancy, renal insufficiency and paediatric age group). If necessary, an anti-Xa assay is the recommended test [100]. Enoxaparin should be stopped 24 h before bronchoscopy if the patient is on a dose of 1 mg·kg−1 every 12 h, and should be stopped 36 h before if the patient is on a schedule of 1.5 mg every 24 h. It can be restarted within 24–72 h post-bronchoscopy after homeostasis is achieved [88].
The inability of protamine sulfate to fully bind LMWH explains its incomplete neutralisation of the anticoagulant effect. Nevertheless, its use as an antidote is justifiable if bleeding is severe. Hirsh et al. [87] have suggested administering protamine sulfate at a dose of 1 mg per mg of LMWH within 8 h of the last dose of LMWH, and a second dose of 0.5 mg per mg of LMWH if bleeding continues.
Fondaparinux (Arixtra)
Fondaparinux, an indirect factor Xa inhibitor, is a synthetic pentasaccharide that binds antithrombin in the plasma, potentiating its effect on factor Xa. Fondaparinux is administered subcutaneously once daily and has a half-life of 17 h. Owing to its predictable anticoagulant effect, drug monitoring is not required. It is excreted unchanged in the urine, hindering its use in patients with renal disease [87, 101, 102]. Fondaparinux is used for the prevention of VTE in hip fracture, hip and knee replacement and abdominal surgery, and for treatment of VTE, HIT (off-label use) and ACS [103–108].
Due to its renal elimination, peri-procedural management of fondaparinux should take into account the creatinine clearance. For creatinine clearance >50 mL·min−1 it should be stopped 3 days before and restarted 24 h after bronchoscopy once haemostasis is achieved. It is recommended that it should be stopped for longer in patients with creatinine clearance <50 mL·min−1.
Unlike heparin, fondaparinux does not interact with protamine sulfate. In cases where uncontrolled bleeding occurs, PCCs or rFVIIa can be used in an attempt to reverse its anticoagulant effect [109, 110].
Direct thrombin inhibitors
Argatroban
Argatroban is an intravenously administered competitive reversible direct thrombin inhibitor. It is metabolised by the liver and can therefore be used safely in patients with renal failure [111]. It is approved for prophylaxis or treatment in patients with HIT and for patients with or at risk for HIT who undergo PCI [112, 113].
Argatroban has a plasma half-life of 45 min. In patients with normal liver function, it should be stopped 3 h before and restarted 24 h post-bronchoscopy [114]. The APTT is the recommended test for monitoring its anticoagulant effect [115].
Desirudin (Iprivask)
Desirudin is a recombinant hirudin derivative with irreversible direct thrombin inhibitor action [116]. Compared to argatroban, its use is not recommended in patients with renal failure, as it is cleared primarily by the kidneys, but it can be used in patients with impaired liver function [117]. Desirudin is used for VTE prophylaxis in patients undergoing total hip replacement [118]. Hirudin use for ACS has been studied, but not yet approved [119]. It has a plasma half-life of 2–3 h after intravenous administration [120]. Based on this, it should be stopped at least 6–8 h before bronchoscopy if administered intravenously and longer if subcutaneously. The APTT correlates well with the plasma level of desirudin and should be used for monitoring its anticoagulant effect [121].
Bivalirudin (Angiomax)
Bivalirudin is an analogue of hirudin, directly and reversibly inhibiting thrombin. The half-life is 25 min after intravenous injection, longer in patients with impaired renal clearance as it is partially cleared by the kidneys [122].
It has been approved by the FDA to be used as an alternative to heparin in patients undergoing PCI, especially in patients with a history of HIT [123]. It is also approved in patients who are undergoing urgent cardiac surgery and acute HIT. Because of its short half-life it can be stopped 1.5 h before the procedure in patients with creatinine clearance >30 mL·min−1 and can be restarted within 24 h after bronchoscopy.
There is no specific antidote for direct thrombin inhibitors. rFVIIa can be used to control excessive bleeding [110].
Conclusion
Peri-procedural management of ATAs can be a challenge. An individualised approach should be adopted prior to each bronchoscopic procedure. The risks and benefits should be thoroughly evaluated, and patient safety should always take precedence. A sound understanding of the different ATAs and their individual properties can help guide and simplify the decision-making. Should a bleeding complication occur, the bronchoscopist should be competent at managing complications and make use of the available drug-specific reversal agents.
Acknowledgements
All authors contributed to the content of this manuscript and to approval of the final version to be submitted.
Footnotes
Conflict of interest: None declared.
Provenance: Submitted article, peer reviewed.
- Received January 3, 2017.
- Accepted April 9, 2017.
- Copyright ©ERS 2017.
ERR articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










