





Figures
- FIGURE 1
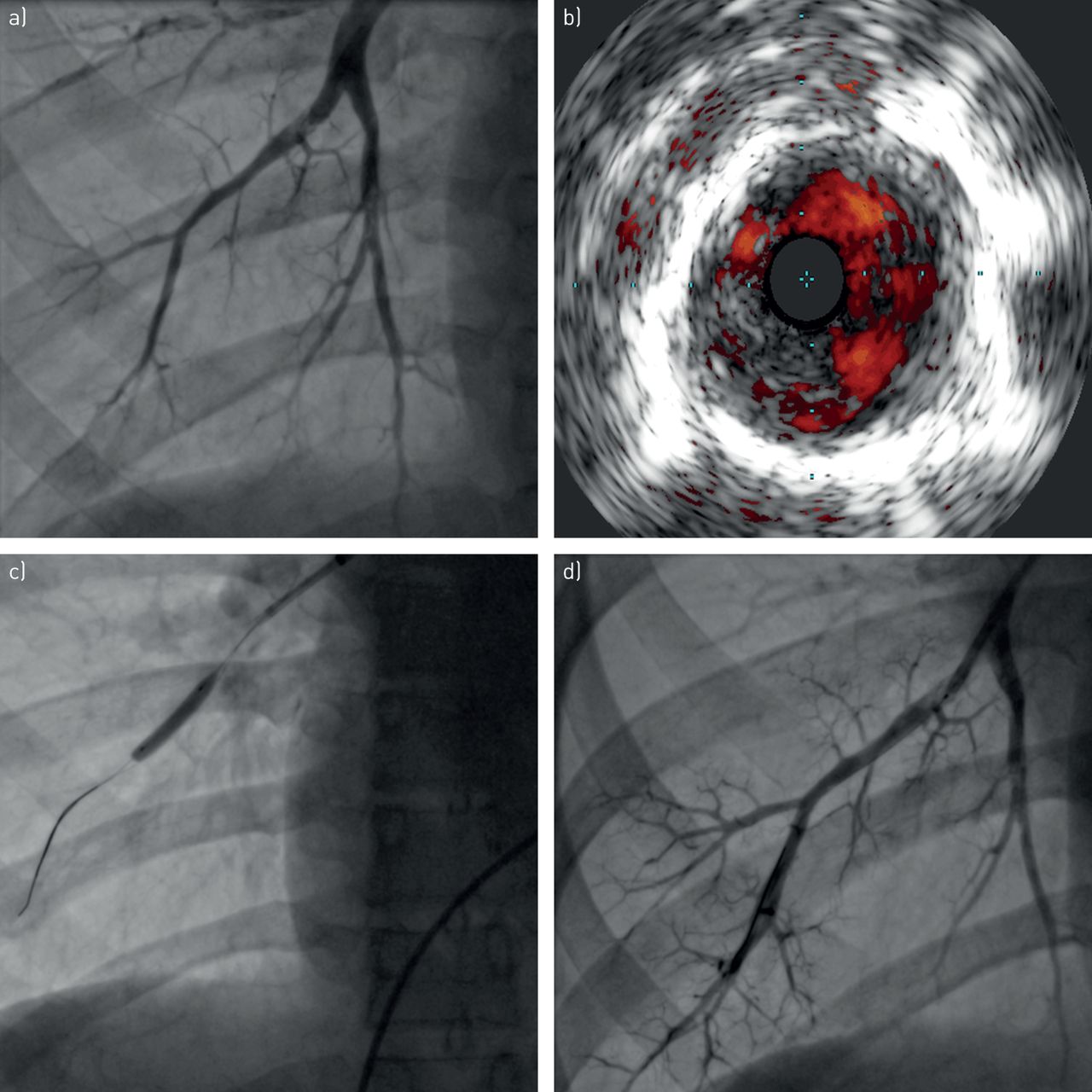
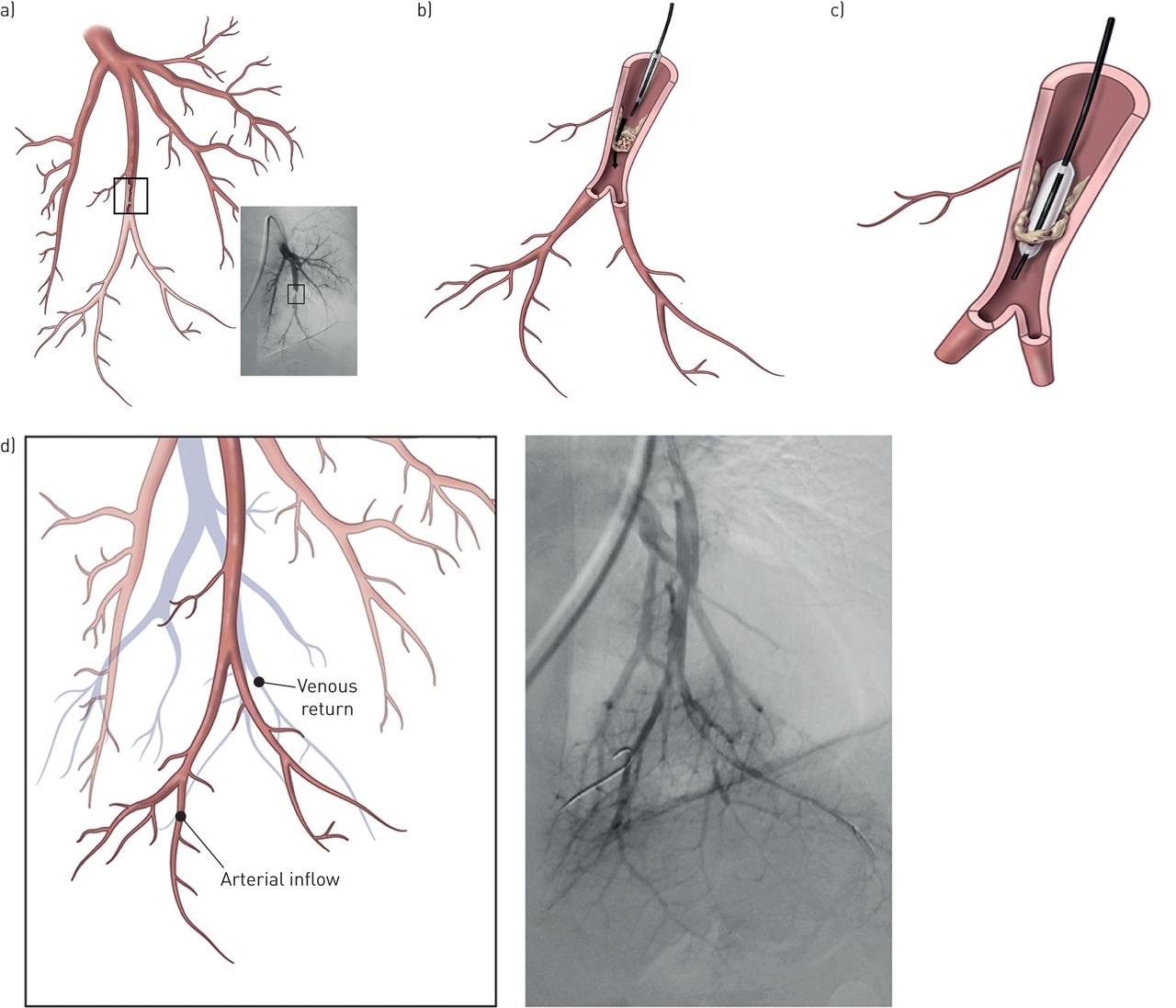
a) Pulmonary angiography, showing a stenosis in the subsegment of the 10th segmental artery (anterior view); b) the catheter is introduced into a web stenosis; c) the wire is introduced between the fibrotic material and the balloon is inflated, leading to rupture of the web. d) Angiography after balloon pulmonary angioplasty shows an improvement of blood flow with better perfusion of the parenchyma and quick venous return. In contrast to pulmonary endarterectomy, the fibrous material is not removed from the arteries, but is crushed against the vessel wall.
- FIGURE 2
Pulmonary arterial imaging before and after percutaneous balloon pulmonary angioplasty (BPA). a) Pre-procedure pulmonary angiogram demonstrating an intra-arterial fibrous “web” lesion; b) the corresponding intravascular ultrasound image showing the intravascular filling defect; c) the BPA balloon in place; d) pulmonary angiogram after the BPA procedure, showing the patent arterial lumen.
- FIGURE 3
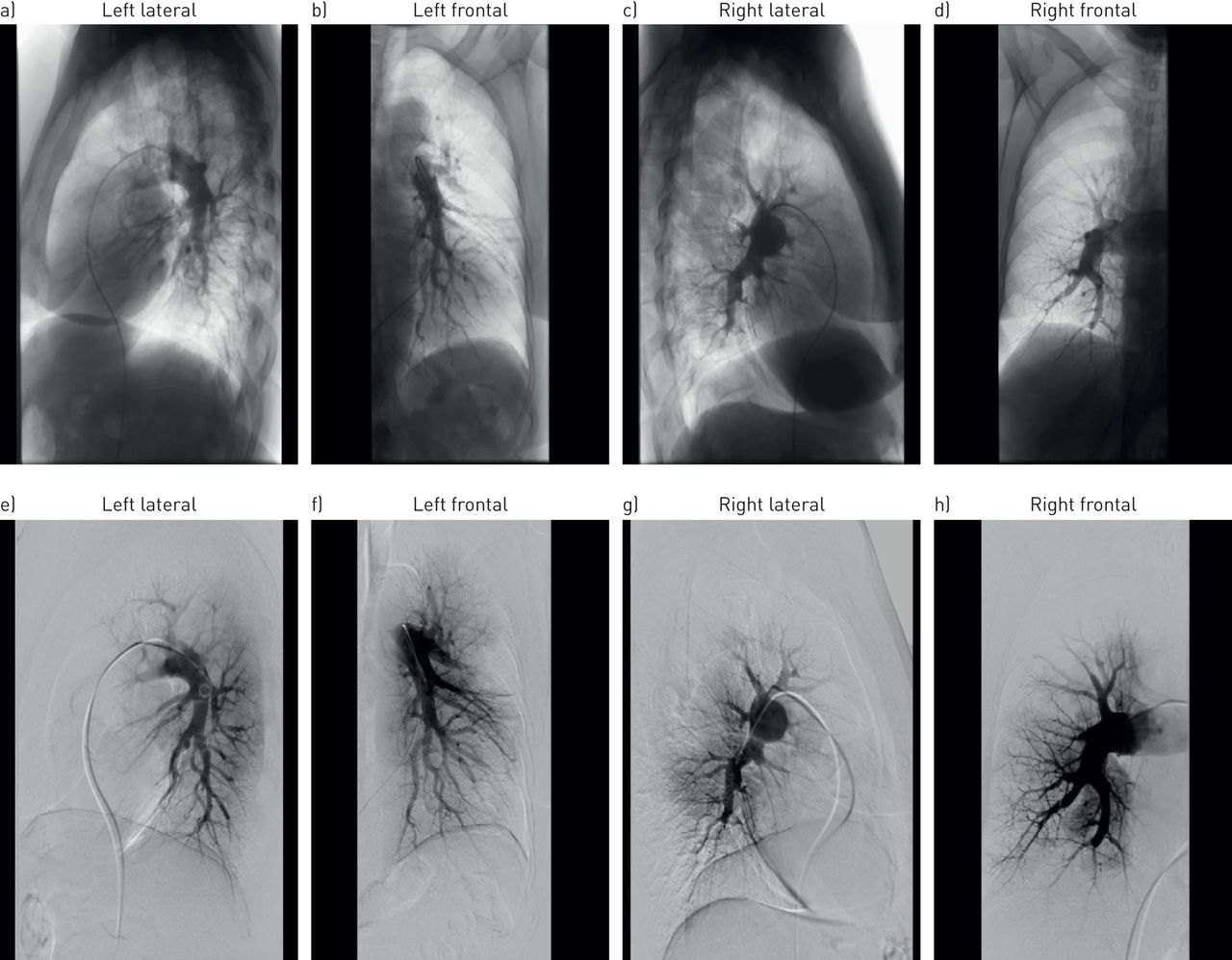
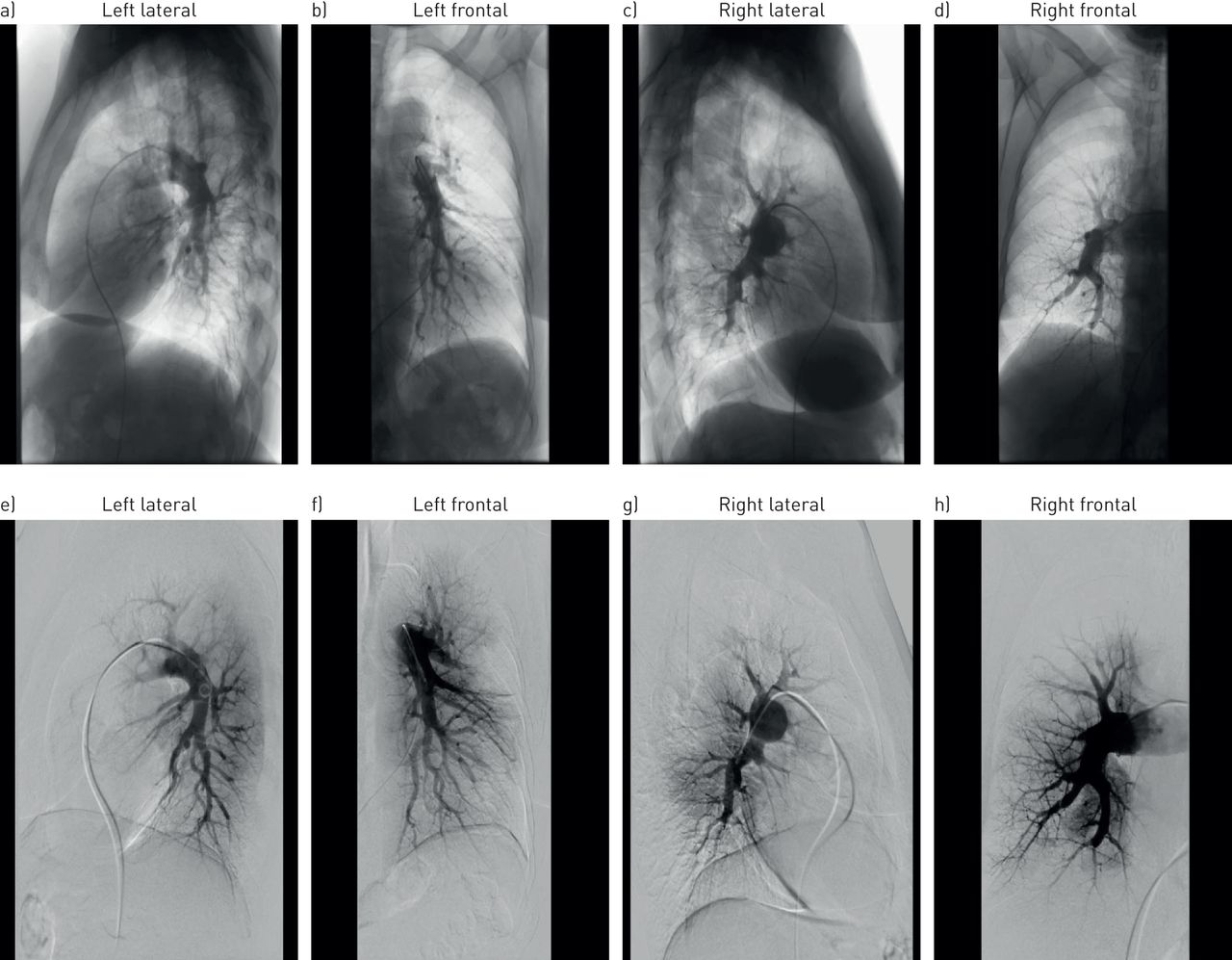
a–d) Selective angiograms and e–h) digital-subtraction angiograms of the right and left pulmonary arteries in a 76-year-old female with chronic thromboembolic pulmonary hypertension manifestation at the level of segmental and subsegmental branching. e–h) Image acquisition in the digital-subtraction angiography technique in frontal or lateral (90° left anterior oblique) projection using intra-arterial contrast injection (iomeprol 300 mg iodine·mL−1, flow rate 12 mL·s−1, volume per injection 35 mL, frame rate 7.5·s-1).
- FIGURE 4
a) Conventional pulmonary angiogram, with b) and c) corresponding optical coherence tomography images from a patient with chronic thromboembolic pulmonary hypertension, showing the nature of vascular obstructions at two locations. #: location for b); ¶: location for c). Scale bars=1 mm.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Published results with balloon pulmonary angioplasty (BPA) in the management of patients with chronic thromboembolic pulmonary hypertension (CTEPH)
First author, year [ref.] Patients (location) Procedures CTEPH medical therapy pre-BPA Mean age years Reduction in mPAP mmHg FC improvement 6MWD improvement Complications Acute mortality (<30 days after BPA) Long-term outcomes Feinstein, 2001 [15] 18 (USA) 47 catheterisations
107 dilations
Mean 2.6 procedures per patientNR 52±12 43.0±12.1 to 33.7±10.2 (p=0.007) NYHA FC 3.3 to 1.8 (p<0.001) 209 to 497 yards (p<0.0001) 11/18 RPO
3/18 MV1 (5.6%)
RPO + RHF, day 716/18 (89%)
alive at 34.2 monthsMizoguchi, 2012 [43] 68 (Japan) 255 sessions;
2–8 sessions
per patient;
1–14 vessels dilated
per session68/68 epoprostenol
1–5 ng·kg−1·min−1
for ∼5 days
pre-BPA62.2±11.9 45.4±9.6 to
24±6.4 (p<0.01)WHO FC
3.0 to 2.0 (p<0.01)296 to 368 m (p<0.01) 76/255 sessions RPO
4/68 patients MV1 RHF, day 28 66/68 (97%) alive at 2.2±1.4 years Kataoka, 2012 [16] 29 (Japan) 51 procedures (mean 1.8 per patient)
Mean 3 vessels dilated per session
Mean 6.5 vessels per patient14/29 bosentan
2/29 ambrisentan
24/29 PDE-5i
15/29 beraprost62.3±11.5 45.3±9.8 to 31.8±10 (p<0.01) At 6 months
NYHA FC (p<0.01)#NR 27/51 procedures RPO
1/29 patients MV1 wire perforation of PA NR Sugimura, 2012 [17] 12 with distal webs
39 controls (Japan)Mean 5 procedures
14 lesions1–3 months pre-BPA:
7/12 epoprostenol
5/12 beraprost
11/12 sildenafil
5/12 bosentan58 Mean±sem 47.8±11.6 to 24.8±4.9 (p<0.01) WHO FC
II/III/IV 33/42/25% at baseline; 100% FC II at follow-upMean±sem 350±105 m to 441±76 m (p<0.05) 6/12 haemoptysis 0 All alive at mean 12 months Andreassen, 2013 [18] 20 (Norway) 73 catheterisations
Mean 3.7 procedures and 18.6 BPAs per patient2/20 sildenafil, stopped before BPA 60±10 45±11 to 33±10 (p<0.001) NYHA FC 3.0±0.5 to 2.0±0.5 (p<0.001) NR 7/20 RPO 1 RVF, day 1
1 acute PE, day 917/20 (85%) patients alive at median 51 months Fukui, 2014 [19] 20 (Japan) Mean 3.2±0.9 procedures per patient 5/20 ERA
13/20 PCA
4/20 PDE-5i
6/20
combination therapy67±9.0 39.4±7.6 to 27.3±8.5 (p<0.001) WHO FC 2.8 to 2.0 (p<0.001) 361±104 m to 463±76 m (p<0.001) No major events 0 NR (1-year retrospective study) Shimura, 2015 [20] 110, including 9 post-PEA (Japan) 423
44 BPA sessions in 9 post-PEA patientsNR 55.1 (post-PEA patients) 43 to 26 (p<0.05) NYHA FC
I/II/III/IV 0/3/5/1 to 7/2/0/0 (p<0.05)NR 1 RPO 0 9/9 alive at median 1.97 years after BPA Inami, 2014 [21] 103 (Japan) 350 procedures; 145 with PEPSI + PWG Bosentan, ambrisentan, sildenafil, tadalafil or beraprost 65 In patients with PEPSI + PWG, from 38 to ≈24¶ NR In patients with PEPSI + PWG, from ≈360 to ≈420 m¶ 0 with PEPSI + PWG 0 with PEPSI + PWG 0 at median 6.4 months with BPA + PEPSI + PWG Inami, 2014 [22] 68 (Japan) 213 sessions For BPA and PEA patients combined (n=107)
prostanoids 60%
PDE-5i 66%
ERAs 55%62 42.9 to 25.0 NYHA FC improved (p<0.05) 349±130 m to 424±111 m (p<0.0001) RPO 7.0%
Haemosputum 2.3%
Haemoptysis 3.3%
Dissection 2.3%
Perforation 0.9%1.47% Mortality 1.5% at 14.3±10.4 months Yanagisawa, 2014 [23] <65 years: 39
≥65 years: 31 (Japan)<65 years: mean 4 sessions
≥65 years: mean 3 sessions (p=0.054)Bosentan, ambrisentan, sildenafil, tadalafil or beraprost <65 years: 54
≥65 years: 70<65 years: 42 to 26.0
≥65 years: 41 to 23.5 (p=0.11)Improved in both groups (p<0.05)
More in age ≥65 years (p<0.0001)<65 years: 380 to 441 m
≥65 years: 310 to 409 m (p=0.553)1 wire perforation At 1 year
<65 years: 0%
≥65 years: 3.2%Kurzyna, 2015 [9] 20 (Poland) 37 procedures
105 vessels82% of patients, mainly sildenafil NR 58±6 to 41±9 WHO FC III/IV 95% at baseline;
35% at follow-upImproved exercise tolerance 2 RPO 10% (RPO) NR Velázquez Martín, 2015 [24] 7 (Spain) 22 (mean 3 procedures per patient; each procedure mean 2.4 segments, 1.2 lobes) ERA + sildenafil + epoprostenol in most patients 61 56±17 to 36±10 (p<0.06) NYHA FC 3.8±0.2 to 2.3±0.2 (p<0.001) NR 2 RPO 1 CVA day 7 NR Roik, 2016 [25] 9 (Poland) 27 sessions in 9 patients
Mean 3 per patient6/11 sildenafil 76 Median (IQR) 40 (32−54) to 34.5 (29−42)
(p=0.01)NYHA FC
I/II/III/IV 0/0/6/3 to 0/7/2/0 (p=0.018)Median (IQR) 304 (135−450) to 304 (205−530)
(p=0.03)2 RPO
1 haemoptysis0 NR Aoki, 2016 [26] 25 (Japan) 113 procedures
Mean 4.7 per patientERA 4%
PDE-5i 71%
Oral prostanoid 21%
Epoprostenol 8%
Riociguat 12%Median (IQR)
70 (60–74)Median (IQR)
37 (28–45) to 23 (19–27) (p<0.01)WHO FC
I/II/III/IV 0/50/46/4% at baseline; 24/76/0/0% at follow-up (p=0.04)Median (IQR) 390
(286–484) m to 490 (411–617) m (p<0.01)No severe complications 0 NR Kawakami, 2016 [27] 97 (Japan) 500 procedures
Mean 5.2 per patient
(1936 lesions)ERA 47.4%
PDE-5i 36.1%
Oral prostanoid 50.5%
i.v. prostanoid 9.3%61.7±12.3 45.1±10.8 to 23.3±6.4 (p<0.01) WHO FC
I/II/III/IV 0/0/70/27% at baseline; 13/76/4/0% at follow-up276.3±123.2 m to 359.3±91.9 m (p<0.01) Haemoptysis (19.6%)
Pulmonary injury (26.0%)4% NR Kimura, 2016 [28] 66 (Japan) Mean 6.8 sessions per patient; mean 13.1 vessels per patient ERA 41%
PDE-5i 55%
Prostanoid 29%
Riociguat 11%63.2±13.2 39.2±10.5 to 20.9±5.4 (p<0.001) NR NR Haemosputum (6.1%)
RPO requiring NPPV (1.1%)0 NR Koike, 2016 [29] 8 (Japan) 16 procedures
Mean 2 per patientNR 70.8±8.6 30.4±11.0 to 25.6±8.2 (p=0.04) NR 332.3±59.6 m to 352.1±
64.1 m (p<0.0001)NR 0 NR Ogo, 2016 [30] 80 (Japan) 385 sessions
Mean 4.8 per patient (1155 lesions)ERA 23%
PDE-5i 25%
Oral prostanoid 42%
i.v. prostanoid 6%
Riociguat 6%Median (IQR)
68 (58–76)42±11 to 25±6 (p<0.01) WHO FC
3.0±0.4 to 1.8±0.4 (p<0.01)372±124 m to 470±99 m (p<0.01) Wire perforation (7.5%)
RPO (4.7%)
Haemoptysis (4.7%)0 NR Tsugu, 2016 [31] 26 (Japan) Mean 6 sessions per patient ERA 46%
PDE-5i 72%
Prostanoid 40%63±16 38.3±8.4 to 18.0±4.2 (p<0.01) WHO FC
2.9±0.6 to 1.2±0.4 (p<0.01)326.8±83.7 m to 400.3±77.4 m (p<0.01) NR NR NR Yamasaki, 2016 [32] 29 (Japan) Mean 2.7 sessions per patient ERA 45%
PDE-5i 50%
Oral prostanoid 40%
Riociguat 40%61.9±10.6 42.6±11.0 to 30.0±6.6 (p<0.0001) NR 391±75 m to 437±68 m (p<0.0001) NR 0 NR Data are presented as n or mean±sd, unless otherwise stated. mPAP: mean pulmonary arterial pressure; FC: functional class; 6MWD: 6-min walking distance; NR: not reported; NYHA: New York Heart Association; RPO: reperfusion pulmonary oedema; MV: mechanical ventilation; RHF: right heart failure; PDE-5i: phosphodiesterase type-5 inhibitor; PA: pulmonary artery; WHO: World Health Organization; PE: pulmonary embolism; ERA: endothelin receptor antagonist; PCA: prostacyclin analogue; PEA: pulmonary endarterectomy; PEPSI: Pulmonary Edema Predictive Scoring Index; PWG: pressure-wire guidance; CVA: cerebrovascular accident; IQR: interquartile range; NPPV: non-invasive positive pressure ventilation. #: values not reported; ¶: estimated from graphs.
Supplementary Material
H-A. Ghofrani ERR-0119-2016_Ghofrani
I. Lang ERR-0119-2016_Lang
H. Matsubara ERR-0119-2016_Matsubara
E. Mayer ERR-0119-2016_Mayer
B.C. Meyer ERR-0119-2016_Meyer










