





Abstract
This review describes a framework for providing a personalised approach to selecting the most appropriate airway clearance technique (ACT) for each patient. It is based on a synthesis of the physiological evidence that supports the modulation of ventilation and expiratory airflow as a means of assisting airway clearance. Possession of a strong understanding of the physiological basis for ACTs will enable clinicians to decide which ACT best aligns with the individual patient's pathology in diseases with anatomical bronchiectasis and mucus hypersecretion.
The physiological underpinning of postural drainage is that by placing a patient in various positions, gravity enhances mobilisation of secretions. Newer ACTs are based on two other physiological premises: the ability to ventilate behind obstructed regions of the lung and the capacity to achieve the minimum expiratory airflow bias necessary to mobilise secretions. After reviewing each ACT to determine if it utilises both ventilation and expiratory flow, these physiological concepts are assessed against the clinical evidence to provide a mechanism for the effectiveness of each ACT. This article provides the clinical rationale necessary to determine the most appropriate ACT for each patient, thereby improving care.
Abstract
Understanding the basis of airway clearance assists in determining the most appropriate technique for the patient http://ow.ly/uQuz307iCIZ
Introduction
Personalised medicine has been used to describe the application of genomics, proteomics and biomarkers to precisely tailor therapy according to various characteristics of an individual patient [1]. This concept of personalised medicine can also be applied to a variety of therapies, such as airway clearance, by taking into account individual patients' lung pathology, clinical, functional, environmental and social factors, as well as the physiological concepts underlying airway clearance techniques (ACTs) [2]. Personalised medicine results in resources being more effectively directed to the most appropriate patients, thereby ensuring that patients receive the specific techniques that optimise the likelihood of benefit in terms of lung health and time commitment. The use of ACTs can be further enhanced by the appropriate use of inhaled medications such as mucoactive agents; however, these medications are not within the scope of this review [3].
This article provides an overview of the physiological principles underlying ACTs and links these physiological principles to the evidence base of commonly used ACTs. This will help clinicians to personalise airway clearance techniques specific to patients’ underlying lung pathology as well as other clinical, functional, environmental and social factors. While some patients with chronic lung disease are ventilated, the vast majority breathe spontaneously. As the physiological mechanisms described differ in ventilated patients, it must therefore be emphasised that this review only describes the spontaneously breathing patient [4].
Background
ACTs are used to supplement the body's mucociliary clearance system when it is impaired by disease. This system is an important lung defence mechanism consisting of airway surface liquid comprising mucus and periciliary layers (PCLs), ciliary epithelium and cough clearing mechanisms [5]. In healthy people, cilia beat at a mean frequency of 11–13 Hz [6], propelling mucus proximally up the airways at a rate of 4–5 mm·min-1 [7, 8]. The rate of clearance is strongly influenced by the hydration state, rigidity and viscosity to elasticity ratio of the mucus [9, 10].
The mucociliary transport system is impaired in chronic suppurative lung diseases, such as cystic fibrosis (CF), primary ciliary dyskinesia (PCD) and bronchiectasis not caused by CF. This is due to the occurrence of one or more of the following conditions: dehydration of the PCL; absence of lubricant activity which prevents adhesion of mucus to airway surfaces [11]; an inherent defect within the cilia; or immunodeficiencies, including cellular defects. Any one of these may cause a failure of ciliary beat frequency and reduced mucociliary clearance. Once this mechanical defence system is breached, the lung is more susceptible to infection and inflammation that can result in further airway damage, eventually leading to bronchiectasis [12].
To be effective, ACTs should assist the body's natural mucociliary clearance system to transport secretions proximally up the airways. Historically, to achieve mucociliary clearance, postural drainage positions were utilised primarily for drainage by relying on gravity [13]. However, there is little supporting evidence that postural drainage utilising gravity effectively mobilises secretions [14, 15]. In CF patients, gravity in a head-down position increased the mucociliary clearance rate only from 0 mm·min-1 to 3–5 mm·min-1 [8]. Based on the assumption that mucociliary clearance rates in gravity dependent positions remain the same in different lung regions, to mobilise secretions from a subsegmental airway in the lower lobe would require a patient to be placed in a head-down position for ∼1 h. Thus, positioning a patient in a head-down position for 3–5 min (as historically used in CF centres) is expected to be ineffective and may even do harm by promoting gastro-oesophageal reflux [13, 16–20]. Two studies, one in CF adults and the other in patients with chronic bronchitis using radiolabeled tracer gases demonstrated that in the side-lying position more secretions are mobilised from the dependent lung than from the nondependent lung, which suggests that the impact of body position on ventilation plays a greater role than gravity in mobilising secretions [21–23]. Since these data were published there has been limited translation of these findings into clinical practice, which is perhaps why in many countries, positioning for drainage remains a key ACT. Positioning for ventilation is discussed later.
Newer ACTs rely on two overriding physiological principles. First, a mechanism to allow air to move behind obstruction and ventilate the regions distally and second, modulation of expiratory airflow in such a way as to propel secretions proximally up the airways. We describe the physiological theories and evidence underlying the use of individual ACTs in the nonventilated spontaneously breathing patient.
Principles for optimising ventilation to obstructed regions of the lung
In normal healthy individuals, during inspiration, airflow takes the path of least resistance, ventilating all areas of the lung, although there may be some asynchronous ventilation secondary to regional and stratified inhomogeneity [24]. In patients with obstructed airways, secretions decrease the diameter of the airway and increase airway resistance, causing preferential ventilation of unobstructed regions and hypoventilation of obstructed regions [24]. Over time, air gradually moves behind the obstruction, but it is not expired, leading to dynamic hyperinflation of the obstructed lung unit. Several mechanisms used in ACTs optimise ventilation to obstructed lung units.
Interdependence during deep inspiration
When tidal volume is increased during a deep inspiration, expanding alveoli exert a traction force on the less well expanded alveoli they surround, thereby assisting in the re-expansion of collapsed alveoli due to the elasticity of the surrounding interstitium. This is known as “interdependence”. It results in air moving into the small airways obstructed by secretions, a phenomenon that has been called Pendelluft [25] and which results from the interdependence. The theory of interdependence was proposed by Mead et al. [26] and a physical model was created to test this hypothesis. The theory was later confirmed in clinical studies on anaesthetised dogs [27].
Collateral ventilation
Ventilation can also occur between adjacent lung segments through collateral channels [28, 29]. In healthy individuals, the importance of collateral ventilation is negligible, due to resistance to airflow being higher in the collateral channels than in the airways. However, if an airway proximal to these collaterals becomes blocked, the collateral channels allow air to move through these pathways due to the pressure differences between adjacent lung units and function to minimise collapse of lung units. Studies have shown that excised human lungs can be re-inflated using collateral channels [30, 31]. There are three types of collateral connections: channels of Lambert, pores of Kohn and pathways/channels of Martin.
Channels of Lambert represent epithelium-lined tubular communications between distal bronchioles and the adjacent alveoli. These are probably the primary channels responsible for collateral ventilation [32]. Pores of Kohn are interalveolar connections. There are ∼50 pores of Kohn, varying from 3 to 13 µm in diameter in each alveolus [33, 34]. In vivo, these pores are mostly filled by fluid and act as a pathway for alveolar lining fluid, surfactant components and cells such as macrophages to move between adjacent alveoli [34]. The pathways/channels of Martin are interbronchiolar connections. Results of an experiment with excised dog lungs, pressurised to 17–28 cmH2O indicated connections between respiratory bronchioles and terminal bronchioles from adjacent lung segments [35], suggesting that use of collateral ventilation channels forms the basis for use of positive expiratory pressure (PEP) ACTs.
3-s breath hold
A 3-s breath hold is another method of ventilating obstructed lung units. When the unobstructed region of the lung has been preferentially ventilated, a pause for 3 s alters the time constants and allows air to move from the unobstructed regions, where the pressure gradient is higher, to the obstructed regions of the lung. This transient movement of gas out of some alveoli into others at the end of inspiration is known as Pendelluft flow. Multiple-breath washout tests have shown that a breath hold increases alveolar gas mixing and decreases the inhomogeneity of ventilation in normal subjects [36]. In post-operative clinical practice it has been demonstrated that a 3-s breath hold is effective in reducing atelectasis [37].
Positioning to optimise ventilation in adults and children
Positioning may be used to enhance ventilation to specific lung regions where secretions are located, such as in bronchiectasis patients. The increased ventilation to those lung regions can then be used effectively to mobilise secretions [21, 22]. There are differences in chest shape and lung mechanics between adults and children which result in differences in ventilation patterns.
When adults are placed in the upright position, optimum ventilation occurs in the mid and lower lobes, while perfusion is greatest in the lower lobes. Theoretically, ventilation/perfusion ratio is 1 at the level of the right middle lobe and lingula [38]. When an adult is placed in a side-lying position, the dependent lung is preferentially ventilated due to the dependent hemi-diaphragm being stretched, causing a greater length to tension ratio, with increased contractility. This creates a greater negative pleural pressure, which, clinically, results in increased ventilation [39]. Perfusion is greater to the dependent lung in both adults and children because it is gravity dependent.
When very young children are placed in the side-lying position, the nondependent lung is preferentially ventilated, probably due to the differences in lung and chest wall mechanics. This occurs in children aged <12 years, causing airway closure to occur in the more dependent regions, independent of lung disease [39].
Supine is the best position to ventilate the upper lobes [38]. However, if this is not suitable, as when taking an inhaled medication, side lying may be an alternative position. Inhaled drug deposition is improved by 13% to the dependent upper lobe when healthy adults were placed in the side-lying position. Adults with mild CF lung disease improve upper lobe deposition by 4% with the same side-lying strategy [40]. Table 1 shows optimal positioning for use during airway clearance to optimise ventilation to obstructed regions of the lung, based on changes in ventilation patterns with positioning.
Optimal positioning for airway clearance techniques to enhance ventilation to obstructed regions of the lung
Use of mobilisation to increase ventilation
Moving a patient into different positions affects ventilation in two different ways. First, a change in body position alters regional ventilation as noted above. Second, by increasing the mobility of a patient, oxygen demand increases, resulting in a corresponding increase in minute ventilation and lung volumes [41]. The resultant increase in ventilation allows air to move into obstructed lung units by interdependence and collateral ventilation.
Methods of utilising expiratory airflow to enhance secretion removal
Increasing the velocity of the expiratory airflow in such a way as to create high shearing forces at the airway walls, and high kinetic energy that enhances the cephalad movement of secretions is a second key mechanism to mobilise airway secretions.
Cough
Coughing is a normal reflex defence mechanism used to clear excessive secretions down to the 7th or 8th generation of airways [42]. During a typical cough, a deep inspiration is followed by closure of the glottis. High intrathoracic pressure (up to 300 mmHg) builds up, resulting in a high explosive, turbulent expiratory flow rate that may exceed 500 L·min-1 [43] when the glottis is opened. During this time, dynamic compression of the airways occurs, resulting in an increase in velocity and kinetic energy which produces a shear force detaching mucus from the airway walls and enhancing the cephalic movement of mucus proximally up the airways. Distal to the regions where the airways are compressed, there may be a collapse of the airways, especially when airway instability is present [43].
Cough is an effective method of clearing secretions from the larger airways in healthy individuals. However, in chronic supperative lung disease, where narrowing and “floppy” airways may close prematurely, it can have detrimental effects if used inappropriately over an extended period as the primary method of clearing secretions. When repeated coughs are used, bronchial wall instability may result from recurrent compression of the airways, thereby reducing expiratory flow and limiting the effectiveness of the cough [44]. Therefore, we recommend that ACTs be used as the primary method of mobilising secretions from the middle and small airways to the larger airways. Then one effective cough be used to clear secretions from the larger airways, thereby preserving the integrity of the larger airways.
Huff/forced expiratory manoeuvre
A forced expiration manoeuvre may also be described as a “huff”. It accelerates the expiratory airflow, creating high linear velocities that shear mucus from the airway walls. Unlike a cough that is performed with a closed glottis, a huff is performed with an open glottis. The huff concept is based on the equal pressure point (EPP) theory [45]. At the EPP, dynamic compression of the airways occurs, creating an increase in the linear velocity of the expiratory airflow which propels secretions proximally. The site of the EPP is determined by the size of expiratory force, airway stability and the elastic recoil. Initiating a forced expiration at a low lung volume shifts the EPP to the periphery, targeting secretions in the small airways. Similarly, initiating a forced expiration from a high lung volume will move the EPP centrally towards the thoracic aperture. This is sometimes referred to as a “huff-cough” [38].
Two-phase gas-liquid flow mechanism
Mucus clearance can be modelled as a two-phase gas-liquid flow mechanism [46]. This indicates that peak expiratory flow rate (PEFR) must exceed peak inspiratory flow rate (PIFR) by ≥10% for mucus to move proximally. The PEFR must also exceed 30–60 L·min-1 to overcome the adhesive strength by which the mucus is attached to the interface. Mucus factors affecting mucociliary clearance are the mucus depth and the viscoelastic properties of mucus. Viscosity is a liquid property of mucus, whereas elasticity is described as the energy storage with an applied stress to a solid. The rate of mucus transport is higher with viscoelastic mucus than with nonelastic viscous mucus [47].
During normal tidal volume breathing at rest, PEFR is not >30 L·min-1 and PIFR is greater than PEFR. The result is that secretions are not mobilised. In order to use airflow to mobilise secretions it is necessary to optimise the expiratory airflow so that PEFR>PIFR by ≥10%, and the velocity of the expiratory flow rate is ≥30–60 L·min-1, depending on the properties of the secretions. In a clinical study that examined the effect of a cough and a huff on regional lung clearance, mean PEFR recorded with a cough was 288±29 L·min-1 and 203±25 L·min-1 with a huff [48]. Both were sufficient to increase tracheobronchial clearance by 44% and 42%, respectively, confirming that an increase in PEFR will enhance lung clearance [48]. Further studies have demonstrated that, in addition to huffing and coughing, manual vibration, oscillating PEP (using the Flutter VRP1; VarioRaw, Aubonnie, Switzerland) and autogenic drainage met the criteria for using expiratory flow to mobilise secretions proximally [49, 50] (table 2).
Effects of airway clearance interventions on peak flow rates
Effects of expiratory airflow on airway surface liquid
Studies have been conducted on the effect of airflow on the volume of airway surface liquid (ASL), using an oscillatory motion device and a cyclic compressive device [47, 52]. The use of these devices caused normal airway cell cultures to double their ASL height with oscillatory motion of 0.3–0.4 Hz, and CF cultures to increase their ASL height to ∼7 µm, thereby becoming capable of maintaining mucus transport for protracted intervals. It is hypothesised that oscillatory shear stress stimulates ATP, which in turn stimulates calcium-mediated chlorine secretion and inhibits sodium absorption.
These important physiological findings provide some basis for the use of airway clearance techniques utilising expiratory airflow and pressure support. However, the oscillation rate of 0.3–0.4 Hz, which is defined in these experiments, is only slightly greater than the rate of breathing in an adult, and does not equate to the oscillation rate of 11–15 Hz described later as the oscillation rate necessary for effective airway clearance. Further studies are needed to confirm these in vitro experiments.
Oscillation
Oscillation frequencies of 5–17 Hz improve tracheal mucus clearance rates in dogs, with frequencies of 11–15 Hz increasing mucus clearance from 8.2 mm·min-1 to 26 mm·min-1 [53], which corresponds to the ciliary beat frequency. In addition, oscillations have an effect on the mucus rheological properties of mucus rigidity (sum of viscosity and elasticity), spinnability (thread forming capacity of mucus) and a derived cough clearance index (CCI). A higher CCI indicates that the mucus is easier to clear with a cough. In an in vitro study, oscillations at 19 Hz using an oscillatory PEP device (Flutter VRP1) resulted in only a small nonsignificant decrease in mucus rigidity and no significant change in the CCI [54]. The use of recombinant human (rh)DNase had the same effect. However, when oscillations were combined with rhDNase the result was a significant decrease in rigidity and a significant change in the CCI. A 4-week clinical study confirmed the findings from the in vitro study and demonstrated a significant decrease in sputum rigidity and spinnability following oscillation with the Flutter compared to autogenic drainage [55]. In another study of CF patients who exercised for 20 min on a treadmill, there was also a significant reduction in sputum rigidity [56]. This result may be due to trunk oscillations associated with treadmill exercise.
Vibrations
Vibrations are the application of fine manual oscillatory movements (either back and forth or side to side) applied to the chest wall during expiration. In studies of healthy subjects vibrations increase PEFR by 50% over relaxed expiration [57, 58]. The frequency of vibration and its effect on expiratory airflow has been compared to several other airway clearance interventions in clinical studies: Acapella (Smiths Medical International, Hythe, UK), PEP, Flutter and percussion [49]. Vibration was applied during expiration after a slow maximal inspiration (table 2). The resultant PEFR of 94.8 L·min-1 and PEFR/PIFR ratio of 1.51 were sufficient to assist in mucus clearance and were greater than the other interventions, but lower than a huff or cough manoeuvre [49]. This work has added greatly to our understanding of the effects of vibration, particularly its impact on expiratory flow rates. In addition, based on studies demonstrating that oscillation frequencies of 5–17 Hz improve mucociliary clearance [52], there is a sound rationale to suggest that vibrations with a frequency of <17 Hz will improve mucociliary transport [49, 58].
Applying physiological principles to airway clearance techniques
In order to determine which ACT is most suitable for the individual patient, it is important to understand how each ACT incorporates the physiological elements of ventilation and expiratory airflow, as described earlier. Both are essential for enhancing mucus clearance. Table 3 gives a synopsis of the physiological basis for each ACT followed by a more detailed outline of their physiological components. The ACTs included in this section are evidence based and have randomised controlled long-term clinical trials to support their use. There are other ACTs and ACT devices in use, and which are currently being researched, but they have not been included in this review as they lack the rigour of evidence from long-term studies.
Physiological basis for each airway clearance technique
Active cycle of breathing techniques
The active cycle of breathing techniques (ACBT) ventilates behind obstructed lung units, using interdependence and collateral ventilation, during thoracic expansion exercises [59]. A 3-s breath hold is included at the end of inspiration. This increases alveolar gas mixing and decreases the inhomogeneity of ventilation [36] (table 3). The main driver of expiratory airflow is huffing, which relies on the use of EPP to enhance mucus clearance. The peak expiratory flow rate, with a huff at high lung volume, is similar to a cough (table 2), demonstrating that the increase in air flow linear velocity is sufficient to promote cephalic movement of secretions [60]. Both the breathing level at which the huff is performed and the strength of the huff are adjusted to allow the EPP to occur where the secretions are located. As huffing is a forced expiration manoeuvre, which can lead to bronchospasm, it is necessary to intersperse it with breathing control, i.e. the forced expiration technique, which is a combination of huffing and breathing control [61]. ACBT is performed in either upright, recumbent or drainage positions [60].
Autogenic drainage
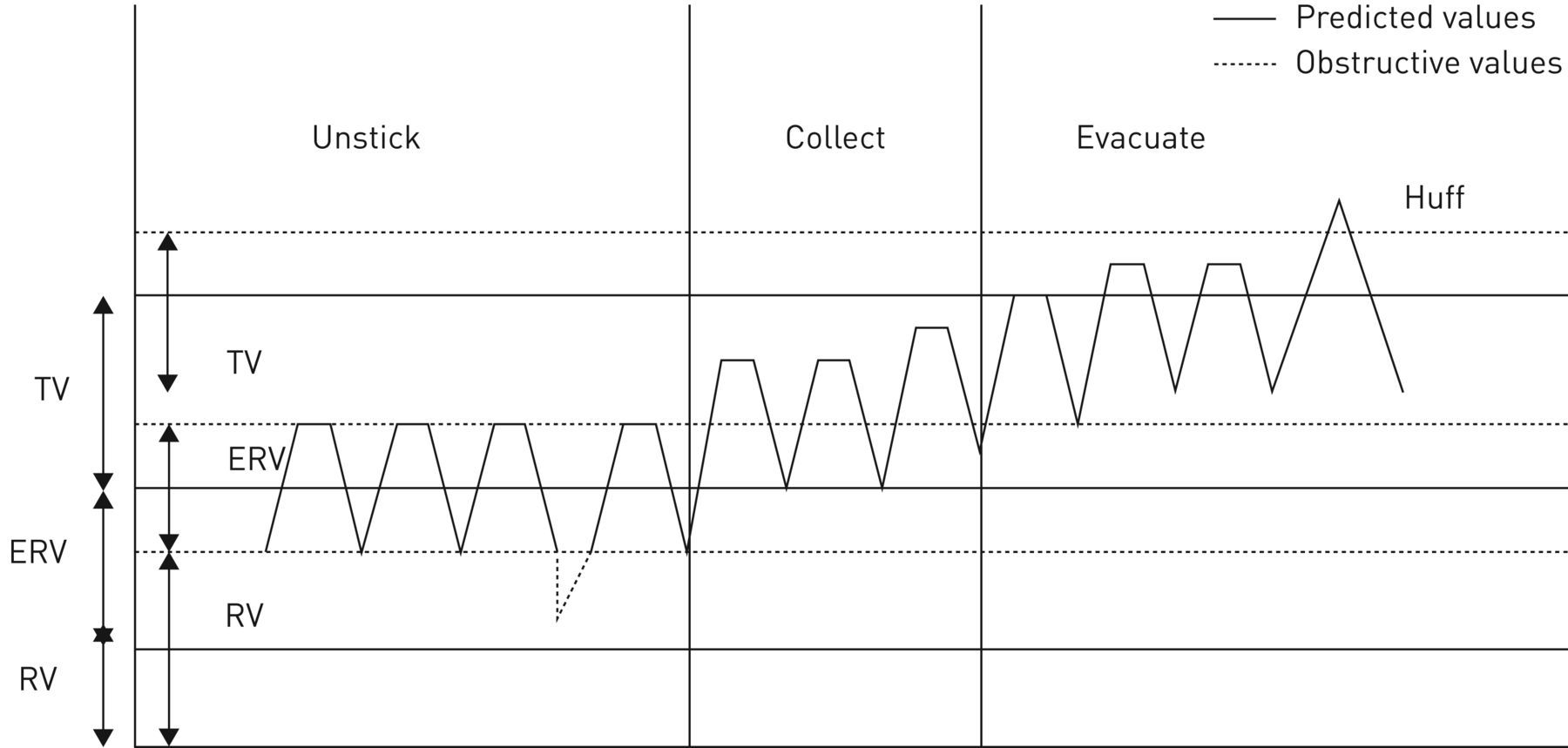
In autogenic drainage, ventilation to obstructed lung regions is achieved using a 3-s breath hold on inspiration during tidal volume breathing, utilising the collateral ventilation channels. The expiratory airflow is modulated so that at each level (unsticking phase, collecting phase and evacuating phase), tidal volume breathing is performed and the expiratory airflow velocity is maximised without causing dynamic compression of the airways (figure 1) [43, 62]. In a study with patients who had obstructive lung disease, when autogenic drainage was performed, the expiratory airflow varied in the range 40–70 L·min-1 depending on lung volume and level of breathing, thereby moving secretions proximally [50]. A slow inspiratory flow rate is necessary to create an expiratory flow rate bias by ≥10%. Autogenic drainage is usually performed in an upright position; an alternative position may be used to enhance ventilation to specific lung regions.

Breathing pattern during autogenic drainage. TV: tidal volume; ERV: expiratory reserve volume; RV: residual volume.
PEP mask
This is a flow-regulating technique employing PEPs of 10–20 cmH2O [63, 64]. Functional residual capacity (FRC) is temporarily increased by breathing through a closed system using a PEP mask (figure 2) [65]. Usually PEP is performed in a sitting position and the patient is instructed to take 12–15 tidal volume breaths through the PEP mask before it is removed for huffing [66]. If the patient removes the mask prematurely, before completing 12 breaths, or uses a mouthpiece without a good seal, the positive pressure in the airways is lost and FRC returns to normal, thereby lessening the effect of the technique. The effect of an application of PEP on collateral channels was demonstrated by Martin [35]. The PEP technique uses a pressure similar to that used in studies on the effect of pressure on ASL [47, 52]. Therefore, it may also enhance mucociliary transport by increasing ASL.

{kind=link}
{kind=link}
Schematic representation of breathing levels during positive expiratory pressure in an obstructed patient. TV: tidal volume; FET: forced expiration technique; TLC: total lung capacity; FRC: functional residual capacity; RV: residual volume. Courtesy L. Lannefors (Sahlgrenska University Hospital, Gothenburg, Sweden).
While ventilation is improved through the use of the PEP mask, the expiratory airflow necessary to mobilise secretions proximally is not achieved, as PEP only has a PEFR/PIFR of 0.47 [49]. Therefore, PEP must be combined with a manoeuvre such as huffing or autogenic drainage.
Oscillating PEP
Flutter and Acapella devices generate an automatically controlled oscillating PEP, although both utilise different physiological bases. They provide similar frequency of oscillation within the range necessary to decrease the viscoelastic and spinnability properties of mucus, and thereby improve mucus clearance [53, 55.] Flutter oscillates with frequencies 15–29 Hz, with average PEPs of 5–19 cmH2O. Acapella oscillates with frequencies of 13–30 Hz, with an average pressure of 6–21 cmH2O [67]. These oscillation frequencies are much higher than the 0.3–0.4 Hz [47, 52] used in the in vitro experiments in which ASL height was doubled. The effect of frequencies of 6–26 Hz on ASL are still to be determined.
Oscillating PEP with Flutter
While exhaling through the Flutter device to expiratory reserve volume (ERV), the individual tunes the device to their ventilatory ability, thereby enabling a modulation of both pressure and airflow oscillation frequency, increasing expiratory airflow, to mobilise secretions proximally [68]. Flutter produces an expiratory flow bias of PEFR/PIFR of 1.15, which is sufficient to mobilise secretions [49]. In addition, huffing is added at the end of each breathing cycle. Unlike the PEP mask, FRC is not increased with the Flutter due to the inability to inspire through the device. To overcome ventilatory asynchronism, inspiration is followed by a 3-s breath hold.
While the Flutter meets the two criteria for mobilising secretions, it raises some concerns. Sometimes, expiration is into the ERV, where closing volume has the potential to cause airway closure [69]. FRC level is not temporarily increased so that the effect of PEP on opening collateral channels is negated. However, the 3-s breath has been shown to increase alveolar gas mixing, alter time constants and allow air to move distal to any obstruction. Another limitation of the Flutter is that due to its pipe-like design, it can only be used in the upright position.
Oscillating PEP with Acapella
Because inspiratory and expiratory manoeuvres are performed through the Acapella in a closed system for 12–15 breaths, its physiological basis is similar to the PEP technique, allowing air to move behind secretions through collateral ventilation channels as a result of an increased FRC level. The addition of oscillation should enhance the technique. Similar to PEP, the expiratory flow bias is insufficient with a PEFR/PIFR ratio of 0.64 [49], therefore the Acapella needs to be combined with huffing to assist in mucociliary clearance from the larger airways. Acapella is position independent, so it can be used in any position to optimise ventilation.
High-frequency chest wall oscillation
During high-frequency chest wall oscillation (HFCWO) (also described as high-frequency chest compression), oscillations are created over the chest wall at frequencies of 5–25 Hz. On expiration the oscillations enhance mucociliary transport in three essential ways, similar to the oscillations produced with oscillatory PEP devices: 1) by altering the rheological properties of mucus [54]; 2) by creating an expiratory flow bias that shears mucus from the airway walls and encourages its movement proximally [53]; and 3) by enhancing ciliary beat frequency [70]. The oscillatory expiration flow generated by compression of the chest wall (creating a PEFR <120 L·min-1) is sufficient to overcome mucus adhesion from the airway wall and propel it up the airway. However, the HFCWO device provides no means of ventilating behind obstructed airways. Unlike the other oscillatory devices, HFCWO does not provide any PEP, and the end-expiratory volume has been reported to decrease by 10–50% during compression [71]. While this may improve expiratory flows through the smaller airways, it may worsen expiratory flows if the airways are smaller and airway resistance is increased, leading to early airway closure [72]. This may lead to a worsening of lung disease. Several short-term randomised controlled trials in CF patients have been unable to demonstrate any significant difference between HFCWO and other ACTs [73–76]. However, in two long-term studies, HFCWO was associated with an increased number of respiratory exacerbations in one [77] and by a decreased in lung function in the other [78].
Personalising airway clearance strategies
While no one ACT has been found to be more effective than another, as synthesised in five Cochrane reviews [79–83] on ACTs in CF, traditionally the choice of ACT has been based on what is available locally, the training and expertise of the local physiotherapist and culture [84]. However, a one-size fits all approach based on regional preference may not address specific patient needs. An individualised strategy should take into account the patient's disease state, preference, motivation and maturity, which, together with the physiological knowledge base of each ACT, applies the most effective airway clearance intervention for that individual. Some examples of clinical considerations based on the unique physiological principles of each ACT are as follows.
A deep inspiration with a 3-s breath hold is a particularly effective means of increasing ventilation in patients with a restrictive component to their lung disease [37], but using a 3-s breath hold in a patient with a severe lung disease who is tachypnoeic may lead to hypoxia.
A forced expiration, as used in ACBT and with the various PEP devices, needs to be adapted to the individual's underlying lung pathology. In a patient with collapsible airways, a huff may compress the airways in such a way as to limit expiratory airflow rather than to increase the velocity of airflow [43]. Alternatively, if bronchospasm is present, airflow obstruction is greater therefore the force of the huff needs to be reduced.
In autogenic drainage the expiratory airflow is gently accelerated, avoiding compression of the airways. This technique is therefore more favourably suited to patients with bronchospasm, or patients with haemoptysis, where a gentler technique is required. In a clinical study, patients with bronchospasm responded best to autogenic drainage [85]. As autogenic drainage requires a self-awareness of one's own respiratory mechanics and concentration to perform, it is generally used in teenagers or adults, unless a caregiver is skilled in its administration.
PEP increases FRC during tidal volume breathing, evening out intrapulmonary distribution of ventilation and opening up regions that are otherwise closed off [65]. It is therefore effective in both restricted and obstructed patients. In addition, the PEP splints the airways during expiration, thereby avoiding airway collapse, which makes it a favourable technique for patients with unstable airways.
Adding oscillations to expiration, either by using an oscillatory PEP device or HFCWO device, has the added advantage of increasing mucociliary clearance [53], decreasing the viscoelastic properties of mucus and potentially rehydrating mucus. When using oscillation devices, the clinician must consider what method they want to use to first ventilate behind the obstructed units. Flutter uses a 3-s breath hold; Acapella, like PEP, increases FRC, splinting airways open. HFCWO needs to be combined with either deep inspiratory manoeuvres, 3-s breath hold or PEP.
Exhaling into the ERV, as used during autogenic drainage, Flutter and HFCWO assist in mobilising secretions from the small airways, but have the potential to cause airway closure [62, 69, 71]. To avoid this, during these techniques, the therapist should ensure that patients adequately incorporate methods to ventilate small airways, such as 3-s breath holds or thoracic expansion exercises.
A therapeutic strategy for an individual patient may involve a combination of ACTs. For example, in a patient with unstable large airways, the use of a PEP device will enhance ventilation, but during the huffing phase the airways may be unable to resist compression. By combining PEP with autogenic drainage, expiratory flow rates could be increased without causing airway compression, thereby mobilising secretions more effectively
Conclusion
The approach to care of the individual patient must be personalised. In clinical practice, more than one ACT may be effective for a patient at a given time in their disease trajectory, and choice of technique may then be dependent on availability and patient preference. Other considerations include cleaning and durability of an ACT device if one is used. However, more often than not, due to the varying nature of the underlying disease pathology and phenotypic characteristics, and taking into account the clinical, functional, environmental and social factors of individual patients, ACTs need to be personalised to meet patients’ specific needs. This requires a sound understanding of the physiological basis of each technique.
Examining the application of physiological principles to ACTs provides a better understanding of how to optimise airway clearance strategies to the individual patient's underlying pathology. This allows for both more personalized, improved patient care. Physiological theories which support ACTs had previously been identified [42, 43, 86]. However, this is the first review to present the physiological evidence supporting methods that ventilate behind obstructed lung units, and modulate of expiratory airflow, and to collate this physiological evidence in an effort to assist in translation into practice.
Disclosures
Supplementary Material
J.S. Elborn ERR-0086-2016_Elborn
Footnotes
Received: Aug 18 2016 | Accepted after revision: November 29 2016
Conflict of interest: Disclosures can be found alongside this article at err.ersjournals.com
Provenance: Submitted article, peer reviewed.
- Copyright ©ERS 2017.
ERR articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Principles for optimising ventilation to obstructed regions of the lung
- Methods of utilising expiratory airflow to enhance secretion removal
- Applying physiological principles to airway clearance techniques
- Personalising airway clearance strategies
- Conclusion
- Disclosures
- Footnotes
- References
- Figures & Data
- Info & Metrics