





Abstract
Multidrug-resistant (MDR) tuberculosis (TB) is a threat to global TB control, as suboptimal and poorly tolerated treatment options have resulted in largely unfavourable outcomes for these patients. The last of six cohort studies conducted in Bangladesh which assessed a new shorter regimen using currently available TB drugs showed promising results and offered the possibility of a more acceptable and more effective regimen than the one recommended by the World Health Organization (WHO). The aims of stage 1 of the STREAM (Evaluation of a Standardised Treatment Regimen of Anti-tuberculosis Drugs for Patients with Multidrug-resistant Tuberculosis) trial are to evaluate the efficacy and safety of this regimen, compared to the current WHO-recommended standard of care. Stage 2 evaluates two new bedaquiline-containing regimens: one an all-oral regimen and the second a further shortened and simplified version of the stage 1 study regimen, comparing the efficacy and safety of each to that of the stage 1 study regimen and also to the WHO-recommended standard of care. Success of the stage 1 study regimen would in all probability provide a new standard of care for MDR-TB patients, while positive results from the bedaquiline-containing regimens in stage 2 may allow for even greater progress in the management of this difficult population.
Abstract
A review of the STREAM trial, which evaluates the safety and efficacy of new treatment regimens for MDR-TB http://ow.ly/VtVkQ
Introduction
The increasing burden of multidrug-resistant (MDR) tuberculosis (TB), defined as TB with resistance to isoniazid and rifampicin (the two core drugs of the drug-sensitive TB regimen) is threatening TB control programmes worldwide. In 2014, an estimated 480 000 people developed MDR-TB globally [1]. However, only an estimated 26% (123 000 people) were notified and even fewer (111 000, ∼23%) started treatment. Unlike drug-sensitive TB, which can be treated effectively and cured with the current standard of care, treatment outcomes for MDR-TB are poor, with less than half of cases having successful outcomes with no more than one in 10 MDR-TB patients being effectively identified and treated [1].
The World Health Organization (WHO)'s guidance on the management of MDR-TB recommends an 8-month intensive phase and a total duration of ≥20 months of therapy in treatment-naïve patients. However, these recommendations are conditional, with “very low-quality evidence” to support them [2, 3]. The poor MDR-TB treatment success rates suggest that current drug regimens are suboptimal. In addition, they are costly with a high pill burden, as many drugs, with significant potential for adverse events, are given for a long duration. These factors also inhibit good treatment compliance with further negative impact on treatment outcomes.
The poor outcomes and limited treatment options available to patients with MDR-TB led the Damien Foundation to conduct a series of six prospective observational cohort studies over a period of 12 years in Bangladesh to assess outcomes using fluoroquinolone-based regimens. The regimens were sequentially adapted based on the results of each preceding cohort and the most promising results were seen with the 9-month regimen used in the last cohort of 206 patients, which had a relapse-free cure rate of 87.9% [4]. This regimen included a fourth-generation quinolone, gatifloxacin, and isoniazid given at a higher than usual dose; the latter was used despite laboratory-confirmed resistance because there was evidence to suggest that patients with low levels of resistance conferred by the inhA mutation would benefit from it. The authors chose a regimen focused on effectiveness rather than efficacy, aiming for a better tolerated regimen to enhance compliance. The 9-month regimen also proved to be very cost-effective, costing just over €200 using generic formulations of the drugs, compared to the cost of treating MDR-TB and extensively drug-resistant TB in Europe, which has recently been estimated to be as high as €82 000 [5, 6]. An update from this cohort in >500 patients showed that 84% maintained a favourable outcome [7].
A number of countries have begun to introduce the “Bangladesh regimen” or a variant of it into their programmes, although it has not been evaluated in a randomised controlled trial. A similar regimen to that studied in Bangladesh but given over 12 months has been assessed in cohort studies in Cameroon and Niger, with an 89% cure rate reported in both countries [8, 9]. The 9-month regimen is also currently being evaluated in cohort studies in nine West African countries. Preliminary results are promising, with 96% of enrolled patients achieving sputum culture negativity at the end of the 4-month intensive phase of treatment [10]. However, the regimen has never been studied in a randomised controlled trial and greater evidence on its safety and efficacy is required in order for the WHO to recommend the regimen for widespread programmatic use.
A recent individual patient data meta-analysis of 9153 MDR-TB patients from 32 observational studies conducted in 23 countries showed a 54% treatment success rate [11]. It confirmed that treatment success was associated with use of later-generation fluoroquinolones, addition of ethionamide or prothionamide as well as use of at least four likely effective drugs in the intensive phase and at least three likely effective drugs in the continuation phase.
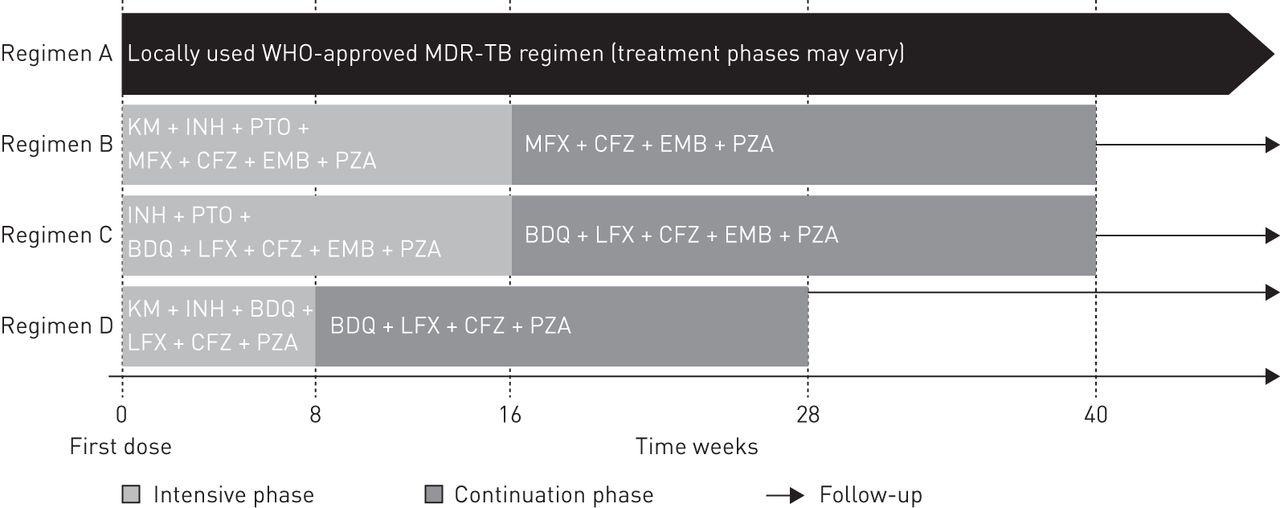
Stage 1 of STREAM (Evaluation of a Standardised Treatment Regimen of Anti-tuberculosis Drugs for Patients with Multidrug-resistant Tuberculosis) is a multicentre randomised controlled trial comparing outcomes of a 9-month regimen, based closely on the one developed in Bangladesh, with the current standard of care, the WHO-recommended regimen [12]. The trial is being conducted in a variety of settings including in the presence of HIV co-infection and different levels of resistance to other commonly used drugs such as pyrazinamide. In a second stage, two other short-course regimens will also be evaluated (figure 1).

{kind=link}
STREAM (Evaluation of a Standardised Treatment Regimen of Anti-tuberculosis Drugs for Patients with Multidrug-resistant Tuberculosis) treatment regimens. WHO: World Health Organization; MDR-TB: multidrug-resistant tuberculosis; KM: kanamycin; INH: isoniazid; PTO: prothionamide; MFX: moxifloxacin; CFZ: clofazimine; EMB: ethambutol; PZA: pyrazinamide; BDQ: bedaquiline; LFX: levofloxacin.
STREAM stage 1
Primary objectives
Stage 1 of STREAM was initiated in July 2012 with the aim of expanding the limited evidence base for the treatment of the MDR-TB population. The two primary objectives were 1) to assess whether the proportion of patients with a favourable efficacy outcome 132 weeks after randomisation of a 9-month regimen based closely on the one used in Bangladesh is not inferior to the WHO-approved MDR-TB regimen (control regimen); and 2) to compare the proportion of patients who experience grade 3 or greater adverse events (graded according to the Division of AIDS severity criteria for adverse events), during treatment or follow-up, on the 9-month regimen when compared to the control regimen [13].
Choice of regimens
The aim of STREAM is to compare, in a noninferiority design, the efficacy and safety of a 9-month regimen based on the one studied in Bangladesh (regimen B) with the WHO-recommended standard of care (regimen A). Regimen B is comprised of moxifloxacin, clofazimine, ethambutol and pyrazinamide given for 9 months (40 weeks) with kanamycin, isoniazid and prothionamide given during the 4-month (16 weeks) intensive phase. The intensive phase can be extended by 4 or 8 weeks in the event of delayed sputum smear conversion. Regimen doses are prescribed according to weight bands, as in Bangladesh (table 1).
Stage 1 drug doses
The study regimen differs slightly from the regimen studied in Bangladesh in that gatifloxacin has been replaced by moxifloxacin as the later-generation fluoroquinolone. The two drugs have similar bactericidal activity [14]; the substitution was necessary because gatifloxacin has been withdrawn from the market by the manufacturer due to reports of associated dysglycaemia [15], but the higher than standard dose of moxifloxacin in the higher weight bands has not been studied before and requires careful safety monitoring.
Sites
The countries selected to participate in the STREAM trial were assessed on predefined criteria as outlined previously [12]. Seven sites were found suitable and willing to participate in STREAM stage 1: two sites in Ethiopia (Addis Ababa), three in South Africa (Durban, Pietermaritzburg and Johannesburg) and one each in Vietnam (Ho Chi Minh City) and Mongolia (Ulaanbaatar).
Patient eligibility criteria
Adult patients with confirmed MDR-TB who consented to participate in the trial were recruited if they met the STREAM eligibility criteria at screening (table 2). The Institute of Tropical Medicine (Antwerp, Belgium) confirmed species identification and susceptibility of all positive sputum cultures.
Stage 1 eligibility criteria
Study design, statistical analysis plan, medical monitoring plan, ethical approval and health economics assessment
The recruitment process, study design, medical monitoring plan, ethics approval process and statistical analysis plan have been described in an earlier article, as was the outline of the health economics substudy component of stage 1 [12].
Status
Recruitment to stage 1 was completed in June 2015, by which time a total of 424 patients had been randomised. Follow-up is ongoing and results are expected early in 2018.
STREAM stage 2
Following the successful initiation of stage 1 the investigators were invited to consider whether the trial could be adapted to include additional regimens. After extensive discussions with the STREAM collaborators and other experts it was decided that the two most relevant questions to address were: 1) is it possible to have an effective fully oral 9-month regimen for MDR-TB in order to avoid the problems of administration and toxicity of the injectable drug; and 2) could treatment be further shortened to only 6 months. Discussions with the United States Agency for International Development and Janssen Pharmaceuticals (Titusville, NJ, USA), the manufacturer of bedaquiline, a provisionally licensed novel drug which is the first US Food and Drug Administration (FDA)-approved TB drug in 50 years [16, 17], led to an agreement to evaluate two additional short-course regimens, both of which included bedaquiline in stage 2 of the STREAM trial.
Current evidence regarding the use of bedaquiline is largely based on compassionate use programmes where it is given for 6 months to MDR-TB patients in addition to an optimised background regimen as per WHO guidelines. The limited information available highlights the importance of stage 2 of STREAM in order to obtain more robust data regarding the long-term safety and efficacy of bedaquiline [18, 19].
Stage 2 regimens
Regimen C is a fully oral 9-month regimen in which bedaquiline replaces kanamycin and is prescribed throughout the 9 months, and levofloxacin replaces moxifloxacin. The duration of the intensive phase and the remaining drugs are the same as for regimen B. Regimen D is a 6-month regimen where bedaquiline, clofazimine, pyrazinamide and levofloxacin are prescribed for 28 weeks, supplemented by isoniazid and kanamycin for the first 8 weeks. The substitution of moxifloxacin for levofloxacin was necessary to reduce the potential risk of QT prolongation with co-administration of bedaquiline and moxifloxacin.
The impact of the alternative regimens on the use of healthcare resources will also be assessed in stage 2, as part of the STREAM health economics substudy.
Primary objectives of STREAM stage 2
The primary objectives of programmatic relevance are to assess whether the proportion of patients with a favourable efficacy outcome on regimen C and regimen D is noninferior to that on regimen B at 76 weeks. In addition, a third objective, requested by the FDA, to meet the regulatory requirements for bedaquiline is to assess whether the proportion of patients with a favourable efficacy outcome on regimen C is superior to that on regimen B at 76 weeks.
A particularly important secondary objective of stage 2 is to compare the proportion of patients who experience grade 3 or greater adverse events (graded according to the Division of AIDS severity criteria for adverse events), during treatment or follow-up.
Patient eligibility criteria
The eligibility criteria from stage 1 will remain, with a few additional criteria. Since bedaquiline is known to contribute to QT prolongation [17], the exclusion criteria for stage 2 include risk factors for QT prolongation; in addition, the threshold at which patients are excluded on account of evidence of possible corrected QT prolongation has been lowered from 500 to 450 ms. Furthermore, patients who have received recent MDR-TB treatment, rifampicin or previous bedaquiline will be excluded, as will patients with a CD4 count <50 cells·mm−3, those with severe liver or renal impairment or abnormal levels of potassium, magnesium or calcium at screening.
Treatment allocation
Eligible patients will be allocated to the locally approved current WHO regimen (regimen A), the 9-month regimen studied in stage 1 (which becomes the new control regimen for stage 2: regimen B) or one of the two new study regimens (C or D), with a ratio of 1:2:2:2, respectively. Randomisation will be stratified by site, HIV status and CD4 count (<350 or ≥350 cells·mm−3).
Duration of follow-up and assessment of primary outcome
Since the primary comparisons in stage 2 will be between the new study regimens, C and D, each with the control regimen for stage 2, regimen B, and not with regimen A, the primary outcome for stage 2 will be at the earlier time point of 76 weeks from randomisation (36 weeks after completion of treatment for regimens B and C, and 48 weeks for regimen D). This is expected to capture the majority of relapses that are likely to occur post-treatment based on evidence from trials in drug-sensitive disease [20]. As in stage 1, patients will continue to be followed up to 132 weeks from randomisation, when secondary comparisons will be made between regimens C and D, with regimen B and with regimen A.
Sample size assumptions
The stage 2 primary efficacy assessments are noninferiority comparisons, as in stage 1. Assuming a favourable efficacy outcome at week 76 in regimen B of 75% (consistent with stage 1), and the same efficacy outcome in regimens C and D, given a noninferiority margin of 10% and an assumption that as many as 10% of patients will not be assessable in the primary analysis, then a total of 990 patients (330 each for regimens B, C and D) would be required to demonstrate noninferiority, with 80% power and 2.5% significance (one-sided). 165 patients will be randomised concurrently to regimen A.
Analysis of primary end-points
For the primary efficacy analysis, the difference in proportion of favourable outcomes between regimen C and B, and between regimens D and B, with 95% confidence intervals and p-values, will be estimated using a stratified analysis of the difference from each stratum using Cochran–Mantel–Haenszel weights. The analysis will be stratified by HIV status, and, if HIV-positive, by CD4 count <350 or ≥350 cells·mm−3. The upper limit of the 95% confidence intervals of the difference in proportion of patients found to be favourable between regimens B and C, and between regimens B and D must be <10% in both the modified intention-to-treat and per-protocol populations for regimens C or D to be declared noninferior to regimen B.
In addition to the noninferiority outcomes, if regimen C or D is determined to be noninferior to B at the primary time point of 76 weeks from randomisation, then the superiority of regimen C or D compared to B will be assessed.
Secondary efficacy analyses will be conducted at the later time point of 132 weeks from randomisation, and will include comparisons between regimens C and D with regimens A and B.
In the event that regimen B is not found to be noninferior to regimen A in stage 1 or in stage 2, regimens B and C will be assessed in comparison with regimen A using the same criteria for noninferiority as described above.
Medical monitoring
As in stage 1, the monitoring of patient safety is a crucial aspect of the trial as multiple potentially toxic drugs are being used. In addition, as clinical experience with bedaquiline is limited, stage 2 involves stringent safety monitoring of adverse drug reactions, drug–drug interactions, QT abnormalities and liver, renal and pancreatic toxicities.
Status
Recruitment for stage 2 is due to start at the beginning of 2016, with enrolment expected to continue for 3 years. Primary results are expected in 2020, with secondary results available the following year.
Discussion
The suboptimal and toxic regimen currently recommended for MDR-TB has inhibited the successful management of affected patients, resulting in the poor treatment outcomes associated with this largely neglected disease. In addition, the absence of data from randomised clinical trials for MDR-TB has prevented the WHO from being able to produce strong recommendations to guide MDR-TB treatment.
The cohort studies conducted in Bangladesh suggested that better treatment outcomes are possible using alternative shorter regimens of currently available drugs. However, despite the promising results of the final Bangladesh cohort, the observational study design meant that many questioned the generalisability of these results, warranting a further study of this regimen within a randomised trial. Furthermore, the potential toxicity of the MDR-TB drugs makes the assessment of regimen safety in a randomised comparison particularly important for patients and treatment programmes.
STREAM stage 1 is the first randomised controlled trial to evaluate alternative MDR-TB regimens in multiple high-burden settings. If the study regimen is successful, it is expected to provide a new standard of care for MDR-TB. However, a potential limitation of the regimen is that its success may be adversely affected by a high prevalence of fluoroquinolone and pyrazinamide resistance in some settings, a factor currently under surveillance by the WHO [21].
Stage 2 compares the effectiveness of two new bedaquiline-containing short-course regimens, an all-oral regimen and a shorter 6-month regimen. If these are shown to be noninferior or superior to the stage 1 study regimen, this would represent an even greater advance for patients with MDR-TB and TB control programmes globally.
Acknowledgements
The members of the STREAM trial team are as follows. I.D. Rusen: International Union Against Tuberculosis and Lung Disease, Paris, France; Patrick P.J. Phillips, Ibrahim Abubakar, Karen Sanders, Wendy Dodds, Ben P.E. Spittle, Chiara P. Borg, Emma Beaumont, Andrew J. Nunn and Sarah K. Meredith: Medical Research Council Clinical Trials Unit at University College London, Institute of Clinical Trials and Methodology, London, UK; Armand Van Deun: International Union Against Tuberculosis and Lung Disease, Paris, France and Institute of Tropical Medicine, Antwerp, Belgium; Gabriela Torrea: Institute of Tropical Medicine, Antwerp, Belgium; Chen-Yuan Chiang: International Union Against Tuberculosis and Lung Disease, Paris, France, and Division of Pulmonary Medicine, Dept of Internal Medicine, Wan Fang Hospital, Taipei Medical University, Taipei City, Taiwan; S. Bertel Squire: Centre for Applied Health Research and Delivery, Liverpool School of Tropical Medicine, Liverpool, UK; and Jason Madan: Warwick Medical School, University of Warwick, Coventry, UK.
The STREAM Trial Management Group would like to acknowledge the contribution of our site collaborators: Francesca Conradie (Sizwe Tropical Diseases Hospital, Johannesburg, South Africa), Iqbal Master (King Dinizulu Hospital Complex, Durban, South Africa), Ronelle Narasimooloo (Doris Goodwin Hospital, Pietermaritzburg, South Africa), Tesfamariam Mebrahtu (Armauer Hansen Research Institute, Addis Ababa, Ethiopia), Daniel Meressa Kokebu (St Peter's TB Specialized Hospital, Addis Ababa, Ethiopia), Nguyen Thi Ngoc Lan and Phan Thuong Dat (Pham Ngoc Thach Hospital, Ho Chi Minh City, Vietnam) and Bazarragchaa Tsogt and Naranbat Nyamdavaa (National Centre of National Diseases, Ulaanbaatar, Mongolia).
Footnotes
This study is registered at ClinicalTrials.gov with identifier number NCT02409290.
Support statement: The primary funder of the trial is the United States Agency for International Development (USAID) through the Cooperative Agreement GHN-A-00-08-00004-00. The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government. Additional funding was provided by the UK Medical Research Council (MRC) and the UK Department for International Development (DFID) under the MRC/DFID Concordat agreement. No funders were involved in the design of the study, collection and analysis of the data or its interpretation, nor did they contribute to the writing of the manuscript or to the decision to submit the manuscript for publication. All authors are receiving financial support from the funders of the trial. Additional funding for STREAM stage 2 will be provided by Janssen Pharmaceuticals. Funding information for this article has been deposited with FundRef.
Conflict of interest: None declared.
Provenance: Submitted article, peer reviewed.
- Received November 2, 2015.
- Accepted November 22, 2015.
- Copyright ©ERS 2016.
ERR articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










