





Figures
- FIGURE 1
Involvement of the endothelin, nitric oxide and prostacyclin (PGI2) pathways in the pathogenesis of pulmonary arterial hypertension [1–14]. DP1, EP2, EP4, EP1 and FP are not functionally expressed in the pulmonary artery and do not contribute to vessel tone in the pulmonary artery. In the endothelin pathway the effects of endothelin (ET)-1 are mediated via the ETA and ETB receptors. Receptor binding leads to activation of phospholipase-C and mobilisation of calcium, resulting in vasoconstriction. Selective and dual endothelin receptor antagonists (ERAs) inhibit this pathway. In the pulmonary artery the prostanoid receptors IP, EP3 and TP regulate vessel tone. The prostacyclin pathway involves prostacyclin binding to the IP receptor, which belongs to a family of prostanoid target receptors. Prostanoid binding to the IP receptor induces adenylate cyclase activity, cAMP production and ultimately reduction of Ca2+ concentrations, and leads to vasodilation. TP binding activates phospholipase C, mediating mobilisation of calcium and vasoconstriction. EP3 receptor binding leads to a decrease in cAMP, which blocks vasodilation. Prostacyclin analogues activate this pathway (EP3 pathway). The nitric oxide (NO) pathway involves the production of cGMP, which leads to inhibition of calcium entry, resulting in vasodilation. Phosphodiesterase type 5 inhibitors (PDE-5i) and soluble guanylate cyclase (sGC) stimulators activate this pathway [2–5, 7–14]. #: prostacyclin analogues activate at least one prostanoid receptor in addition to IP. Reproduced and modified from [1], with permission from the publisher.
- FIGURE 2
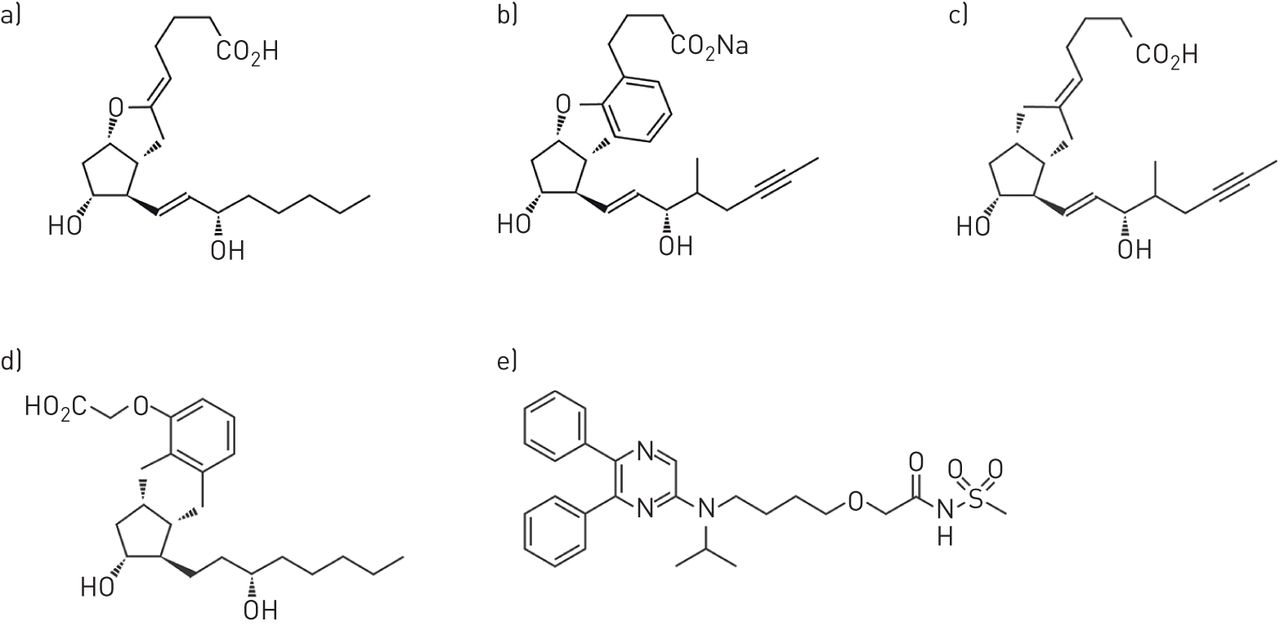
Chemical structures of drugs that bind to the prostacyclin pathway. a) Prostacyclin; b) beraprost sodium; c) iloprost; d) treprostinil; and e) selexipag.
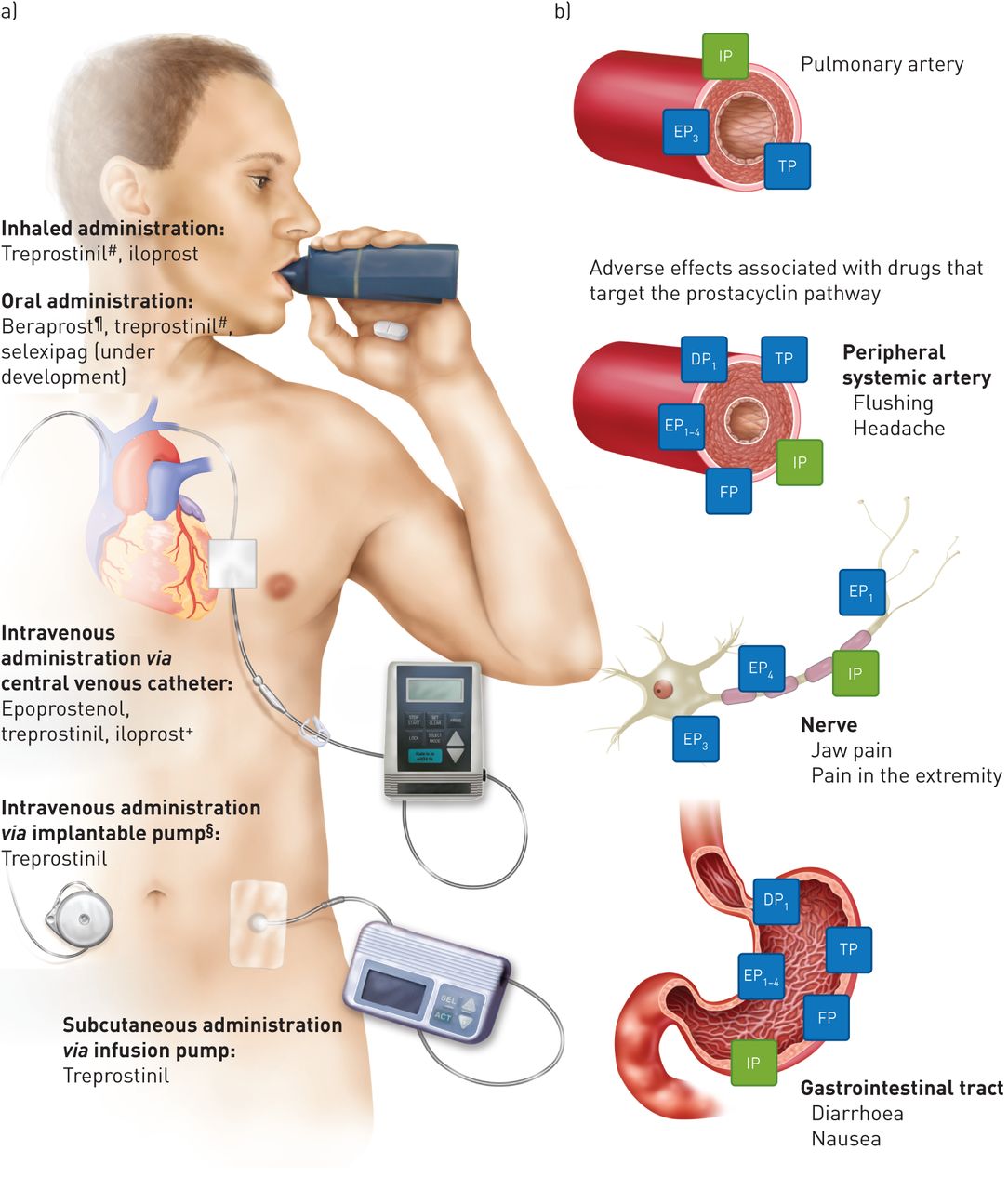
- FIGURE 3
Drugs that target the prostacyclin pathway. a) Routes of administration, and b) target receptors and adverse events [3, 16, 19, 20]. Key tissues associated with known adverse effects are listed. #: approved only by the US Food and Drug Administration; ¶: approved only in Japan and South Korea; +: approved only in New Zealand; §: this pump is an innovation that is not yet widely available.


{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Evidence-based monotherapy treatment algorithm for drugs that target the prostacyclin pathway
Recommendation Evidence PAH severity WHO FC II WHO FC III WHO FC IV Recommended (class I) Data derived from multiple randomised clinical trials or meta-analyses, or from a single randomised clinical trial or large nonrandomised studies Selexipag oral# Epoprostenol i.v.¶; iloprost inhaled+; treprostinil s.c. and inhaled§; selexipag oral# Epoprostenol i.v. Should be considered (class IIa) Consensus of opinion of the experts and/or small studies, retrospective studies and registries Iloprost i.v.+; treprostinil i.v.§ May be considered (class IIb) Data derived from a single randomised clinical trial or large nonrandomised studies Beraprost oralƒ; treprostinil oral Iloprost inhaled and i.v.; treprostinil s.c., i.v. and inhaled Recommendation IA for prostanoid use in sequential combination therapy for inadequate clinical response at maximal therapy [3]. WHO: World Health Organization; FC: functional class. #: not approved at the time of publication; ¶: approved for continuous i.v. administration for pulmonary arterial hypertension (PAH) WHO FC III–IV by the US Food and Drug Administration (FDA) in 1995; +: approved for aerosol administration for PAH WHO FC III in the European Union and Australia in 2003, and PAH WHO FC III–IV by the FDA in 2004; §: approved for s.c. administration for PAH WHO FC II–IV by the FDA and Health Canada in 2002; ƒ: approved for oral administration for idiopathic PAH in Japan in 1995 [36]. Information from [15, 16].
- TABLE 2
Key randomised controlled clinical trials of drugs that target the prostacyclin pathway
First author [ref.] Year (trial acronym) Background therapy Drug Patients n Duration Primary end-point Primary end-point met? Epoprostenol# Rubin [37] 1990 None i.v. epoprostenol 24 8 weeks Change in total pulmonary resistance Yes Barst [38] 1996 None i.v. epoprostenol 81 12 weeks Change in 6MWD Yes Badesch [39] 2000 None i.v. epoprostenol 111 12 weeks Change in 6MWD Yes Badesch [40] 2009 None i.v. epoprostenol 102 3 years Survival No Humbert [41] 2004 (BREATHE-2) None i.v. epoprostenol with bosentan or placebo 33 16 weeks Change in total pulmonary resistance No Simonneau [42] 2008 (PACES) i.v. epoprostenol Sildenafil or placebo 267 16 weeks Change in 6MWD Yes Iloprost¶ Olschewski [43] 2002 None Inhaled iloprost or placebo 203 12 weeks Composite ≥10% increase in 6MWD and improvement in WHO FC Yes Hoeper [44] 2006 (COMBI) Bosentan Inhaled iloprost 40 12 weeks Change in 6MWD No McLaughlin [45] 2006 Bosentan Inhaled iloprost 67 12 weeks Change in 6MWD and WHO FC Yes Treprostinil+ Simonneau [46] 2002 None s.c. treprostinil or placebo 470 12 weeks Change in 6MWD Yes Jing [47] 2013 (FREEDOM-M) None Oral treprostinil or placebo 349 12 weeks Change in 6MWD Yes Tapson [48] 2012 (FREEDOM-C) ERA, PDE-5i or both Oral treprostinil or placebo 350 16 weeks Change in 6MWD No Tapson [49] 2013 (FREEDOM-C2) ERA, PDE-5i or both Oral treprostinil or placebo 310 16 weeks Change in 6MWD No McLaughlin [50] 2010 (TRIUMPH-I) Bosentan or sildenafil Inhaled treprostinil or placebo 235 12 weeks Change in 6MWD 10–60 min after inhalation Yes Beraprost§ Galiè [51] 2002 (ALPHABET) None Oral beraprost or placebo 130 12 weeks Change in 6MWD Yes Barst [52] 2003 None Oral beraprost or placebo 116 12 months Difference in disease progression Yes Selexipag McLaughlin [53] 2015 (GRIPHON) None, ERA, PDE-5i or both Oral selexipagƒ 1156 3 years Time to first morbidity or mortality event Yes 6MWD: 6-min walking distance; WHO: World Health Organization; FC: functional class; ERA: endothelin receptor antagonist; PDE-5i: phosphodiesterase type 5 inhibitor. #: approved for continuous i.v. administration for pulmonary arterial hypertension (PAH) WHO FC III–IV by the US Food and Drug Administration (FDA) in 1995; ¶: approved for aerosol administration for PAH WHO FC III in the European Union and Australia in 2003, and PAH WHO FC III–IV by the FDA in 2004; +: approved for s.c. administration for PAH WHO FC II–IV by the FDA and Health Canada in 2002; §: approved for oral administration for idiopathic PAH in Japan in 1995 [36]; ƒ: not approved at time of publication.
Disclosures
Files in this Data Supplement:









