





Abstract
Although it is often under-recognised, α1-antitrypsin deficiency (AATD) represents one of the most common genetic respiratory disorders worldwide. Since the publication of studies in the late 1980s, which demonstrated that plasma-derived augmentation therapy with intravenous α1-antitrypsin (AAT) can reverse the biochemical deficiencies in serum and lung fluid that characterise emphysema, augmentation therapy has become the cornerstone of patient management. This article, with a focus on experience gained in clinical practice in Germany, provides an overview of some of the research highlights and clinical experience gained in the use of augmentation therapy for AATD during the past 25 years, and briefly discusses the potential role of AAT augmentation therapy in lung transplant recipients. Additionally, the goals of AAT augmentation therapy will be discussed, namely to delay the progression of emphysema, reduce the frequency of exacerbations and improve health-related quality of life. Beyond pulmonary disease, there is recent growing evidence to indicate that AATD could also play a role in rare disorders such as panniculitis, granulomatosis with polyangiitis and ulcerative colitis.
Abstract
Overview of long-term experience gained with AAT augmentation therapy for the treatment of AATD http://ow.ly/HmJLR
Introduction
α1-antitrypsin deficiency (AATD) is one of the most common, but often under-recognised, genetic respiratory disorders worldwide [1]. One of the earliest landmark studies of replacement therapy for AATD associated with emphysema was published in the 1980s by Wewers et al. [2]. This study demonstrated the feasibility of intravenous administration of α1-antitrypsin (AAT) and introduced the concept that is still used in practice today, namely that infusion of AAT 60 mg·kg−1 body weight stabilises serum levels above a predefined threshold (80 mg·dL−1) for at least 1 week. After a rapid rise in serum AAT levels, a significant decrease is observed within 2 days due to redistribution within the body, followed by stabilisation over at least 1 week above the predefined threshold. Importantly, this study demonstrated that AAT infusions derived from plasma are safe and can reverse the biochemical abnormalities in serum and lung fluid that characterise emphysema. Indeed, the study speculated that, in combination with lifetime cigarette smoking avoidance, replacement therapy with AAT may prove to be a logical approach to long-term medical treatment [2].
Due to improvements in technology over recent years, the limits of the “protective threshold” (the threshold for replacement therapy) have recently been re-evaluated, based on data from >6000 individuals enrolled in the Swiss Cohort Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) study [3]. An AAT serum level of 50 mg·dL−1 has been proposed as the limit of the protective threshold, below which individuals are classified as having severe deficiency (fig. 1). The threshold for intermediate deficiency is 90 mg·dL−1 [3].

Suggested areas corresponding to severe α1-antitrypsin (AAT) deficiency (below the protective threshold) and intermediate AAT deficiency (above the protective threshold and below the 10th percentile of the AAT range for subjects carrying the PI*MS genotype). Bars represent the 5th and 95th percentiles of AAT serum levels. Even MZ can have normal serum levels. Reproduced from [3] with permission from the publisher.
What is the optimal dosing interval for i.v. AAT augmentation therapy? The approved frequency is weekly infusions, as proposed by Wewers et al. [2]. However, this is not convenient for some patients and alternative schedules, including twice weekly and every 4 weeks, have been evaluated [4, 5]. With a twice weekly schedule (AAT 120 mg·kg−1), 41% of AAT levels were above the 80 mg·dL−1 predefined threshold for 7 days but the level did not remain above the threshold in any individual for >14 days [4]. Nevertheless, many patients still use this dosing schedule as it could be more convenient than weekly dosing. In nine patients with severe AATD (<35 mg·dL−1), nadir serum levels gradually increased over time with a 4-week AAT dosing interval (250 mg·kg−1). By 12 months, serum levels exceeded 80 mg·dL−1 for a mean duration of 25 days of the 28-day dosing interval [5].
A number of purified AAT preparations, sourced from pooled human plasma, are currently available in various markets (table 1) [6]. The purification process and the amount of active substance differ among the different preparations. A review by Stoller and Aboussouan [7], which evaluated data from two large studies in almost 1200 patients receiving AAT, showed that therapy can be associated with a small proportion of adverse effects, such as dyspnoea or headache, which are generally mild and can be readily managed. In addition, given the relatively high cost of i.v. augmentation therapy, cost-effectiveness considerations need to be taken into account and balanced with the general lack of specific alternative treatment options for AATD [7].
Commercially available preparations of purified α1-antitrypsin
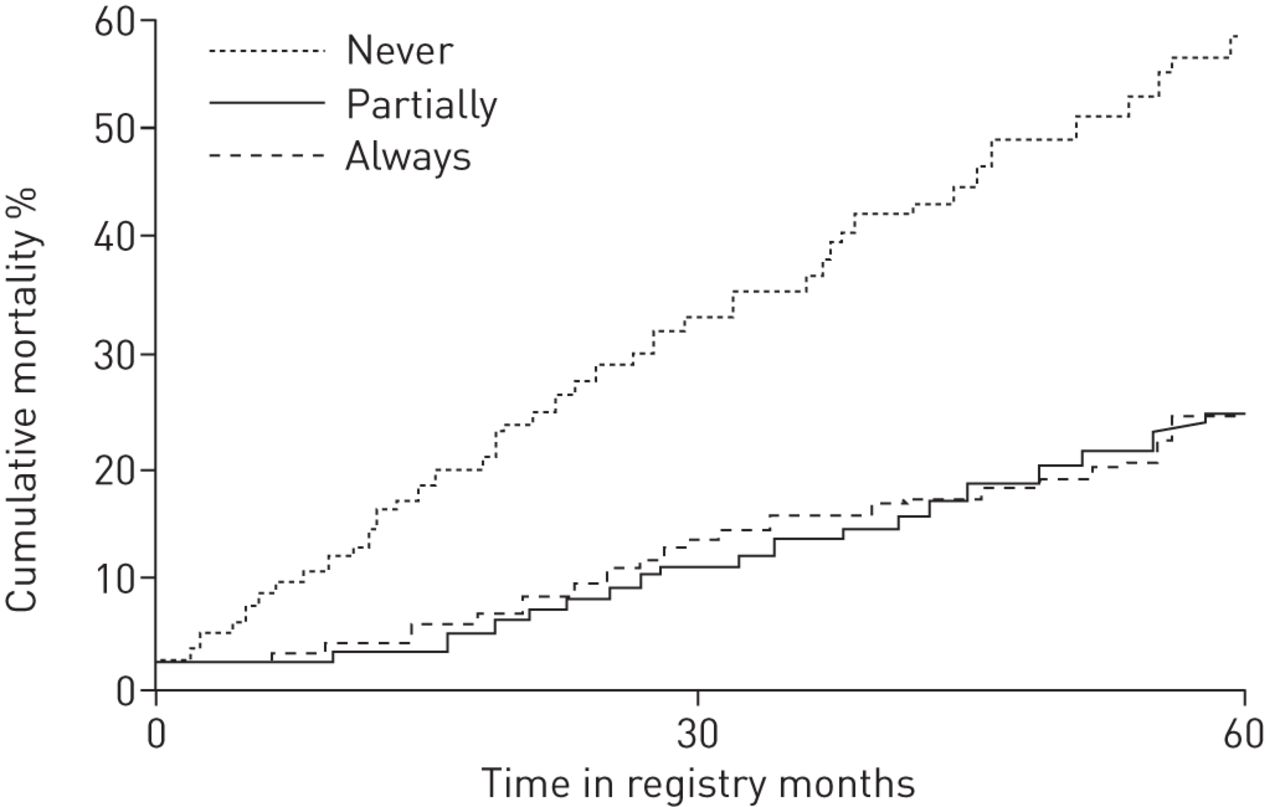
Another landmark study in the area of AATD research was published by the Alpha-1-Antitrypsin Deficiency Registry Study Group [8]. In this study of 1129 individuals with severe AATD enrolled in the US National Heart, Lung and Blood Institute (NHLBI) registry of patients with severe AATD, 382 patients had never, 357 had partially and 390 had always received AAT, and the optimal patient population for AAT therapy was defined by a mean forced expiratory volume in 1 s (FEV1) of 30–65% predicted (moderate obstruction). Whilst it is important to note that the NHLBI registry is limited by its observational design and missing data, in those patients who were either partially or always treated with AAT a survival benefit was observed over 60 months compared with patients who had never received AAT (fig. 2). Pooled analysis of data from 198 treated German and 97 untreated Danish patients also showed that patients with an FEV1 of 31–65% predicted might benefit the most from AAT augmentation therapy [9]. A subsequent meta-analysis of five clinical trials in 1509 patients with follow-up, including spirometry, for at least 1 year further reinforced the findings from earlier studies that the most likely group of patients with AATD to benefit from AAT augmentation are those with a baseline FEV1 30–65% predicted. In this patient subset, augmentation therapy was associated with a 26% reduction in the rate of FEV1 decline (absolute difference 17.9 mL·year−1 (95% CI 9.6–26.1 mL year−1)) [10]. Whilst acknowledging that evidence is not derived from randomised controlled clinical trials, these findings are also endorsed by recommendations from the Alpha-1 Antitrypsin Deficiency Task Force of the American Thoracic Society (ATS)/European Respiratory Society (ERS) [11].
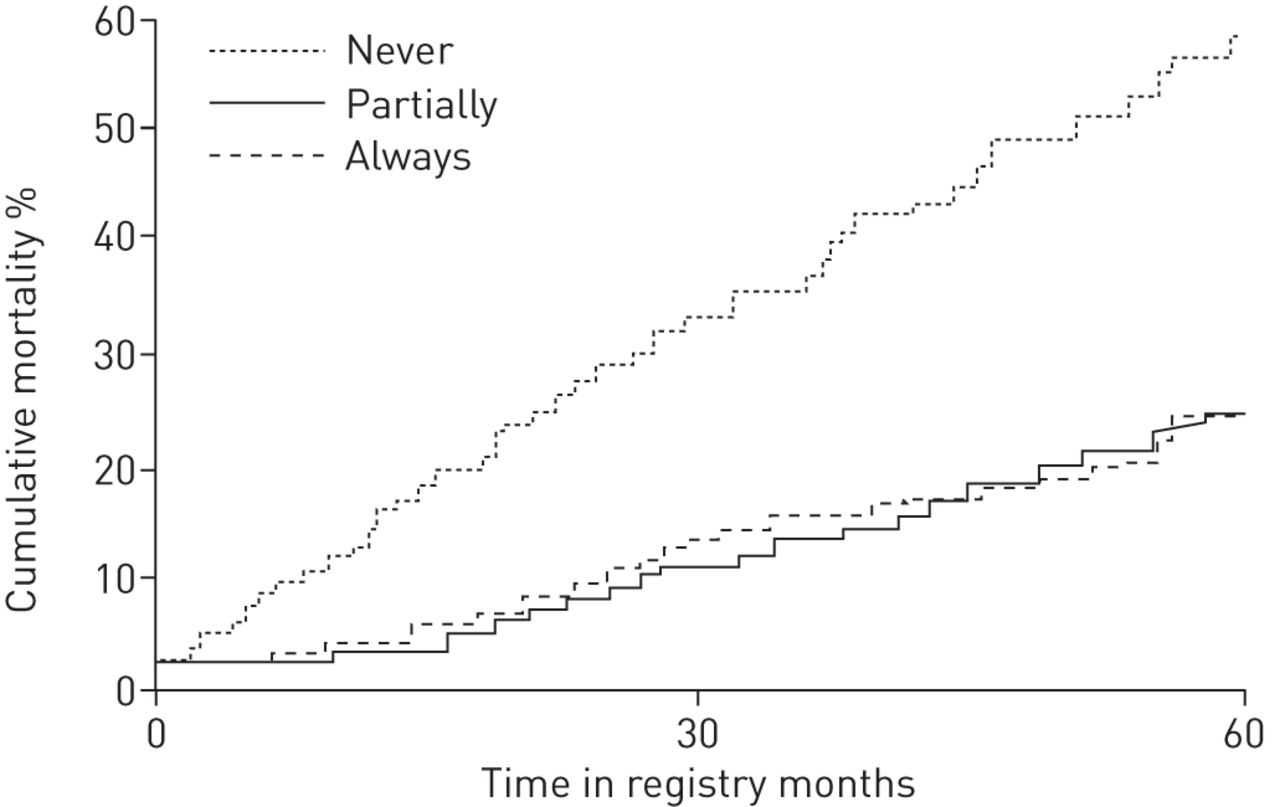
Cumulative mortality over 60 months in patients with α1-antitrypsin deficiency and an initial forced expiratory volume in 1 s <50% predicted who never (n=382), partially (n=357) or always (n=390) received augmentation therapy. Reproduced with modification from [8] with permission from the publisher.
Goals of augmentation therapy with AAT
The three key goals of AAT augmentation therapy are to: 1) delay the progression of emphysema; 2) reduce the frequency of exacerbations; and 3) improve health-related quality of life (HRQoL).
Delaying the progression of emphysema
A number of studies have used computed tomography (CT)-assessed lung density as an indicator for disease progression during AAT augmentation therapy. One of the earlier studies, conducted by Dirksen et al [12], assessed the change in pulmonary function tests and CT-lung density with and without AAT augmentation therapy. 30 patients with moderate emphysema (FEV1 30–80% predicted and AATD of PI*ZZ phenotype) were randomised to either AAT (250 mg·kg−1) or albumin (625 mg·kg−1) infusions at 4-week intervals for at least 3 years. The study showed no significant between-group differences in the primary end-point (pulmonary function tests: daily spirometry and diffusion capacity); however, there was a trend over time towards significant improvements in the change in lung density (whole lung measured by CT) with AAT augmentation infusions compared with albumin (p=0.07) [12].
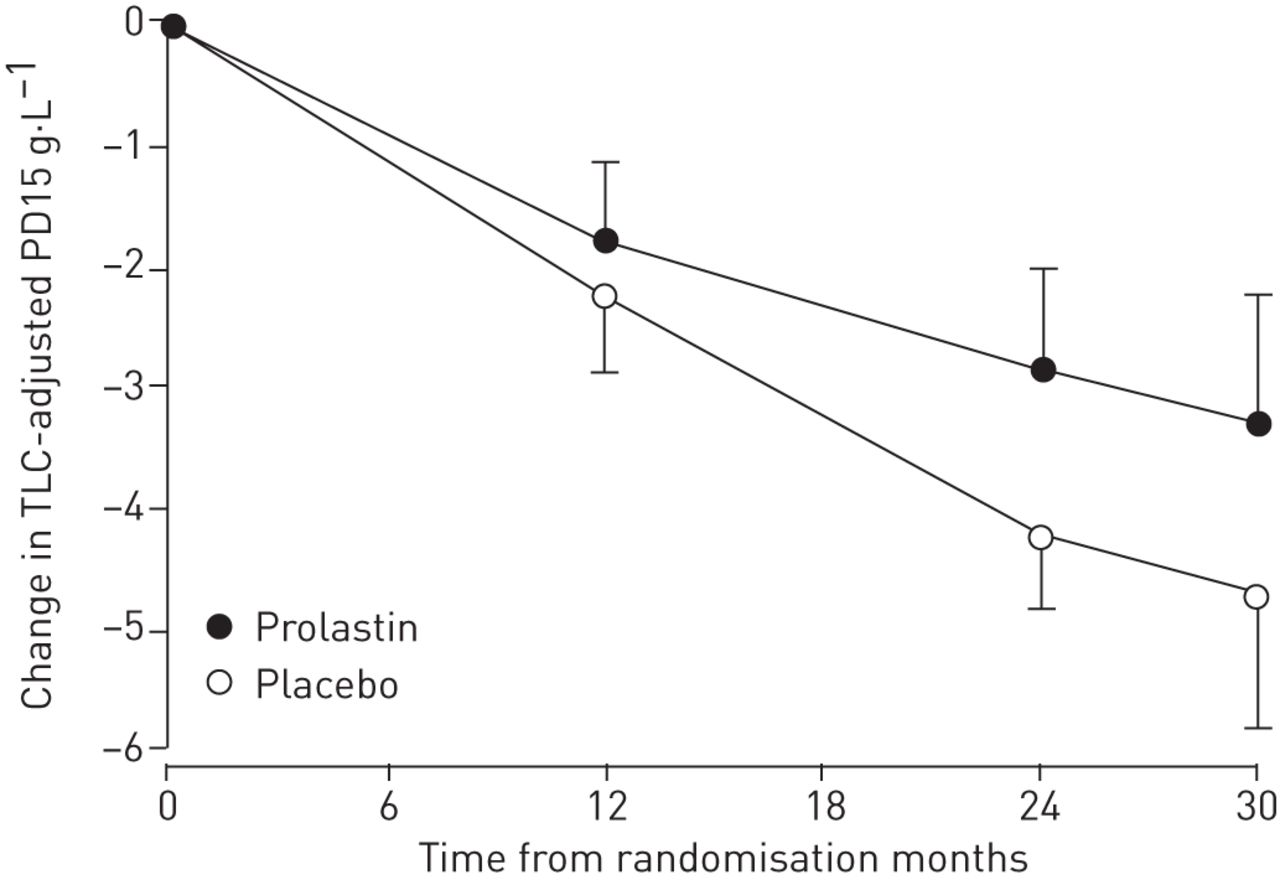
The Exacerbations and Computed Tomography Scan as Lung End-points (EXACTLE) randomised controlled trial also evaluated changes in CT lung density in 77 patients receiving weekly Prolastin 60 mg·kg−1 or placebo [13]. As in the previous study [12], the effect of AAT augmentation therapy was not significantly different from that of placebo but a clear trend towards an effect on lung density was observed (p=0.068) (fig. 3).
{kind=link}
{kind=link}
{kind=link}
Change from baseline in total lung capacity (TLC)-adjusted 15th percentile lung density (PD15) over the course of the study. The error bars indicate sem. Estimated treatment difference in mean slopes (annual change in lung density) 0.857 (p=0.068). Reproduced with modification from [13] with permission.
These studies indicate that CT is a more sensitive outcome measure of emphysema-modifying therapy than physiology and health status, and demonstrate a trend towards a treatment benefit from AAT augmentation.
Data from two similar randomised, double-blind, placebo-controlled trials (the EXACTLE study and a Danish–Dutch study), both of which investigated the efficacy of AAT augmentation therapy on emphysema progression using CT densitometry, were pooled (to increase the statistical power) [14]. Mean follow-up was ∼2.5 years. The mean change in lung density from baseline to last CT scan was −4.082 g·L−1 for AAT therapy and −6.379 g·L−1 for placebo, with a treatment difference of 2.297 (95% CI 0.669–3.926; p=0.006). The corresponding annual declines in lung density were −1.73 g·L−1·year−1 and −2.74 g·L−1·year−1, respectively [14].
Preliminary data from the ongoing RAPID (Randomised, placebo-controlled trial in Alpha-1 Proteinase Inhibitor Deficiency) trial in 153 patients with the PI*ZZ phenotype demonstrated that, over a 2-year follow-up period, weekly AAT 60 mg·kg−1 (standard of care) was associated with a significantly reduced annual CT lung density loss (primary end-point) compared with placebo (−1.45 k·L−1·year−1 versus −2.19 g·L−1·year−1; p=0.017) [15]. However, there were no significant between-group differences in secondary efficacy end-points (spirometry, diffusing capacity of the lung for carbon monoxide and shuttle walk test).
Controversy remains regarding how patients with severe AATD and an initial FEV1 >65% predicted should be managed. Based on our experience, we believe that these patients need to be evaluated every 6 months for lung function. Individuals showing a rapid decline in lung function would be initiated on AAT augmentation therapy [16]. Given the general lack of good quality clinical data, decisions regarding the management of patients in this population are generally made on an individual basis.
Reducing exacerbation frequency
Limited evidence supports the hypothesis that AAT augmentation therapy reduces the incidence of lung infections in addition to slowing the deterioration of lung function and leading to decreased mortality [13, 17–19].
The effect of AAT augmentation therapy on respiratory exacerbations was evaluated by Lieberman [17] via a questionnaire submitted to patients with a PI*ZZ phenotype for AATD. 96 patients receiving augmentation therapy (Prolastin) for 1–10 years were compared with 47 similar patients not receiving augmentation therapy. The questionnaire evaluated whether the patient was aware of any personal benefit of therapy and whether the therapy had an effect on the frequency of lung infections. 74 out of 89 patients who had received AAT therapy for >1 year claimed that they had definitely benefited from such therapy. Of these patients, 56 attributed this to a reduction in the number of lung infections since starting therapy with AAT augmentation. Before starting AAT therapy, the majority of patients had experienced 3−5 infections·year−1 and this number decreased to 0−1 infections·year−1 during AAT therapy (p<0.001) [17].
A recent multicentre, retrospective observational study in 127 severe AATD patients with chronic obstructive pulmonary disease (COPD) demonstrated that augmentation therapy with AAT concentrates (Prolastin or Trypsone) for at least 18 months was associated with a reduced incidence and severity of exacerbations, which subsequently resulted in significant hospitalisation cost savings [18].
A post hoc analysis from the EXACTLE study also assessed the impact of AAT augmentation therapy on the reduction of severe exacerbations [13]. Although overall exacerbation frequency was unaltered by treatment, AAT augmentation therapy was associated with a reduction in exacerbation severity. Compared with placebo, AAT augmentation therapy had a highly significant effect on the number of severe exacerbations (requiring corticosteroids or hospitalisation) (6.7% versus 13.5%; p=0.013) [13].
In patients with AATD, it is important to optimise treatment. In addition to augmentation therapy, vaccination against pneumococci and/or influenza can play an important role in minimising exacerbations. In a cross-sectional questionnaire survey of patients in Germany and Austria with PI*ZZ phenotype AATD, vaccination and augmentation therapy both significantly reduced the frequency of exacerbations compared with no vaccination (p=0.01) and no augmentation therapy (p=0.044) [19].
Improving HRQoL
There are limited data regarding the impact of AAT augmentation therapy on HRQoL in patients with AATD. A recent small, prospective feasibility study conducted in Germany has shown that home-based weekly i.v. Prolastin, administered by an experienced nurse, appears to be safe and results in fewer exacerbations and reduced loss of lung function compared with an historical cohort [20]. Moreover, there were no complications related to home-based infusions and the approach resulted in no elective hospitalisations.
Increased awareness is also an important factor in optimising the management of patients with AATD. With this in mind, an Alpha-1-Center Network has been established in Austria and Germany in order to provide AATD patients with the best possible care. The centre functions as a reference centre for physicians, in addition to the alpha-1 child centres, the AAT core laboratory (Marburg, Germany) and the German AAT register (Homburg, Germany). Through educational meetings, publications in local media and publications in scientific journals the Alpha-1-Center Network aims to disseminate knowledge about AATD and support research in AAT-associated diseases (www.alpha-1-center.de).
Other clinical manifestations of AATD and the role of AAT augmentation therapy in lung transplant recipients
Accumulating evidence indicates that, beyond pulmonary disease, AATD could also play a role in rare disorders including panniculitis, granulomatosis with polyangiitis and ulcerative colitis [21]. Whilst the implications of these extrapulmonary manifestations of AATD are still to be further elucidated, it is important to focus on the overall clinical problems for an individual patient. Of course, their obstructive lung disease should be treated, inhaled corticosteroids should be considered in situations of bronchial hyperresponsiveness, bronchiectasis should be evaluated and managed, and acute exacerbations should be treated. The most important factor, however, is that the patient must stop smoking. Nevertheless, despite best efforts to control obstructive lung disease, many patients will eventually require lung transplantation.
What is the role of AAT augmentation therapy in lung transplant recipients? Based on current ATS/ERS guidelines, augmentation therapy is not recommended in patients with AATD undergoing lung transplantation, due to insufficient clinical evidence [11]. However, there may be individual lung transplant patients for whom this advice may not be appropriate. A recent study by Banga et al. [22] assessed the outcome of single and double lung transplantation in patients with AAT-replete COPD (n=231) and AATD (n=45). There were no significant between-group differences in overall rates of FEV1 decline (p>0.09). However, although the single lung transplant patients had similar trends in FEV1 in both groups, patients with AATD with double lung transplant declined faster (p<0.002) than the AAT-replete patients with COPD. A possible explanation for the difference may be that a higher prevalence of augmentation therapy use by AAT deficient individuals undergoing single lung transplant may have resulted in a slower decline in lung function. There were no between-group differences in acute cellular rejection events or in early or late mortality. Whilst additional studies are needed to better understand the apparent differences between single and double lung transplant in AATD, it is interesting to speculate that these findings indicate that patients with AATD should be eligible for lung transplantation [22]. Indeed, in our clinic we have treated a number of lung transplant patients with augmentation therapy. One interesting case involved a 37-year-old woman with severe PI*ZZ homozygous AATD who had received augmentation therapy for many years before her lung function declined and she underwent successful lung transplantation. However, within a relatively short period her lung function deteriorated quite rapidly and, despite our best efforts, there was no improvement and she underwent re-transplantation. The new transplant performed very well for ∼12 months before a reduction in pulmonary function was observed. Bronchoalveolar lavage identified a high neutrophil burden and azithromycin was started, but without effect. We initiated augmentation therapy and the patient improved and has maintained good lung function for >7 years. In total, we have had four such cases and two of these responded to augmentation therapy.
Based on our limited personal experience with individual patients, the thoughtful use of AAT augmentation therapy for episodes of infection or rejection may be sensible but, at the present time, there is a lack of robust data to confirm the feasibility of this approach and further clinical studies are warranted.
Conclusion
The past 25 years have seen significant developments in the area of AATD and its treatment with augmentation therapy. Nevertheless, despite advances in our knowledge, AAT often remains under-recognised. Delaying the progression of emphysema, reducing the frequency of exacerbations and improving HRQoL are the three key goals of AAT augmentation therapy. Although controversy exists in relation to the use of augmentation therapy in lung transplant recipients, accumulating evidence indicates that, in selected patients, the thoughtful use of augmentation therapy represents a viable option. Looking to the future, the next 25 years will no doubt see further significant advances in the treatment of AATD.
Acknowledgements
Writing assistance was provided by Content Ed Net (Madrid, Spain) with funding from Grifols (Barcelona, Spain).
Footnotes
Conflict of interest: Disclosures can be found alongside the online version of this article at err.ersjournals.com
Provenance: Publication of this peer-reviewed article was supported by Grifols, Barcelona, Spain (article sponsor, European Respiratory Review issue 135).
- Received November 13, 2014.
- Accepted December 17, 2014.
- Copyright ©ERS 2015.
ERR articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References









