





Figures
- Figure 1.
Chest high-resolution computed tomography scans. Multi-slice computed tomography demonstrates a) apical emphysema and b) honeycombing and reticulation with subpleural, basal predominance. Extensive ground-glass opacities can be seen in both panels. Image courtesy of Claus P. Heussel (Thoraxklinik, University of Heidelberg, Heidelberg, Germany).
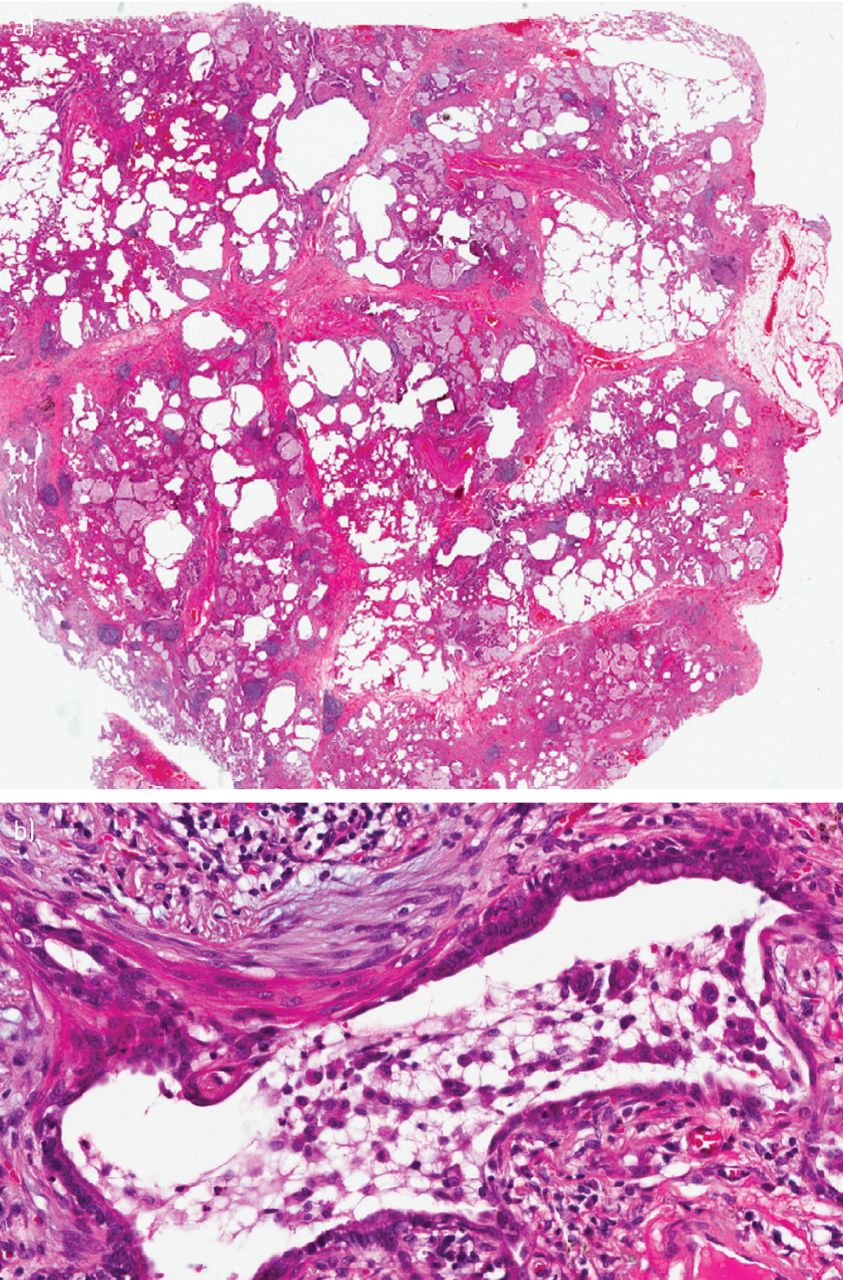
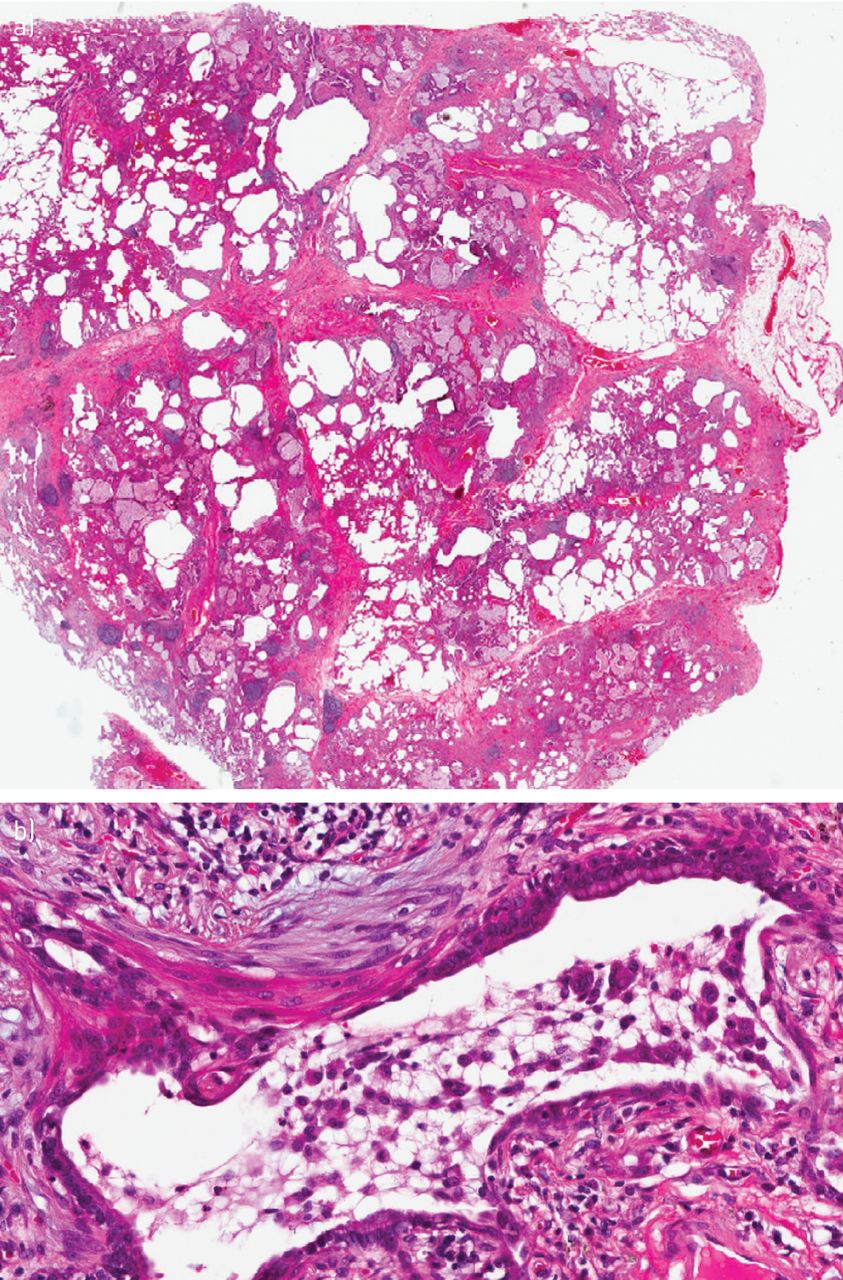
- Figure 2.
a) Low magnification histopathological biopsy showing typical features of usual interstitial pneumonia pattern with a heterogeneous appearance and areas of fibrosis with scarring and honeycomb change. Areas with less affected parenchyma also show emphysematous changes. b) Higher magnification of the histopathological biopsy reveals diffuse pulmonary involvement of numerous macrophage accumulations within most of the distal airspaces, consistent with a desquamative interstitial pneumonia pattern. Image courtesy of Philipp A. Schnabel (Institute of Pathology, University of Heidelberg, Heidelberg, Germany).
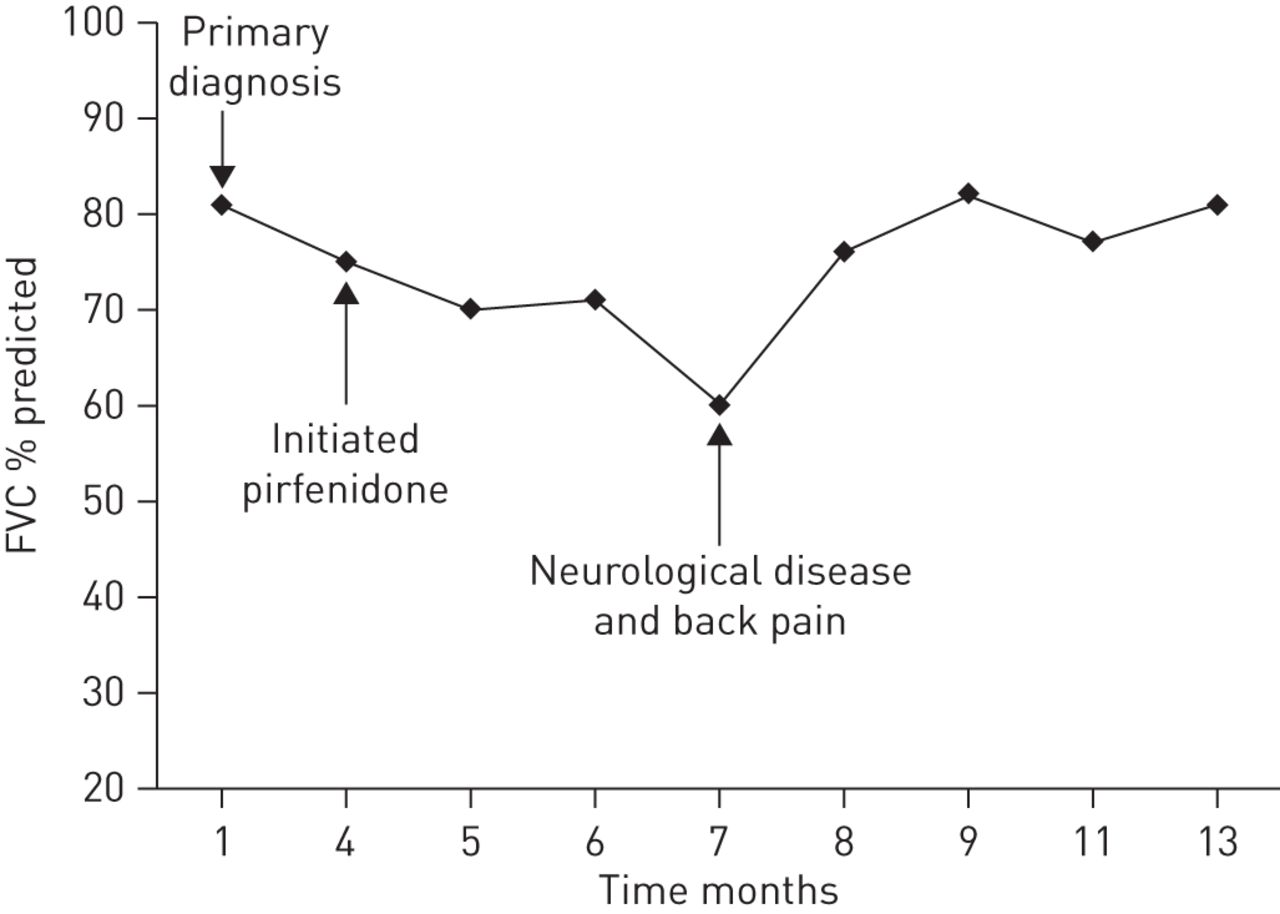
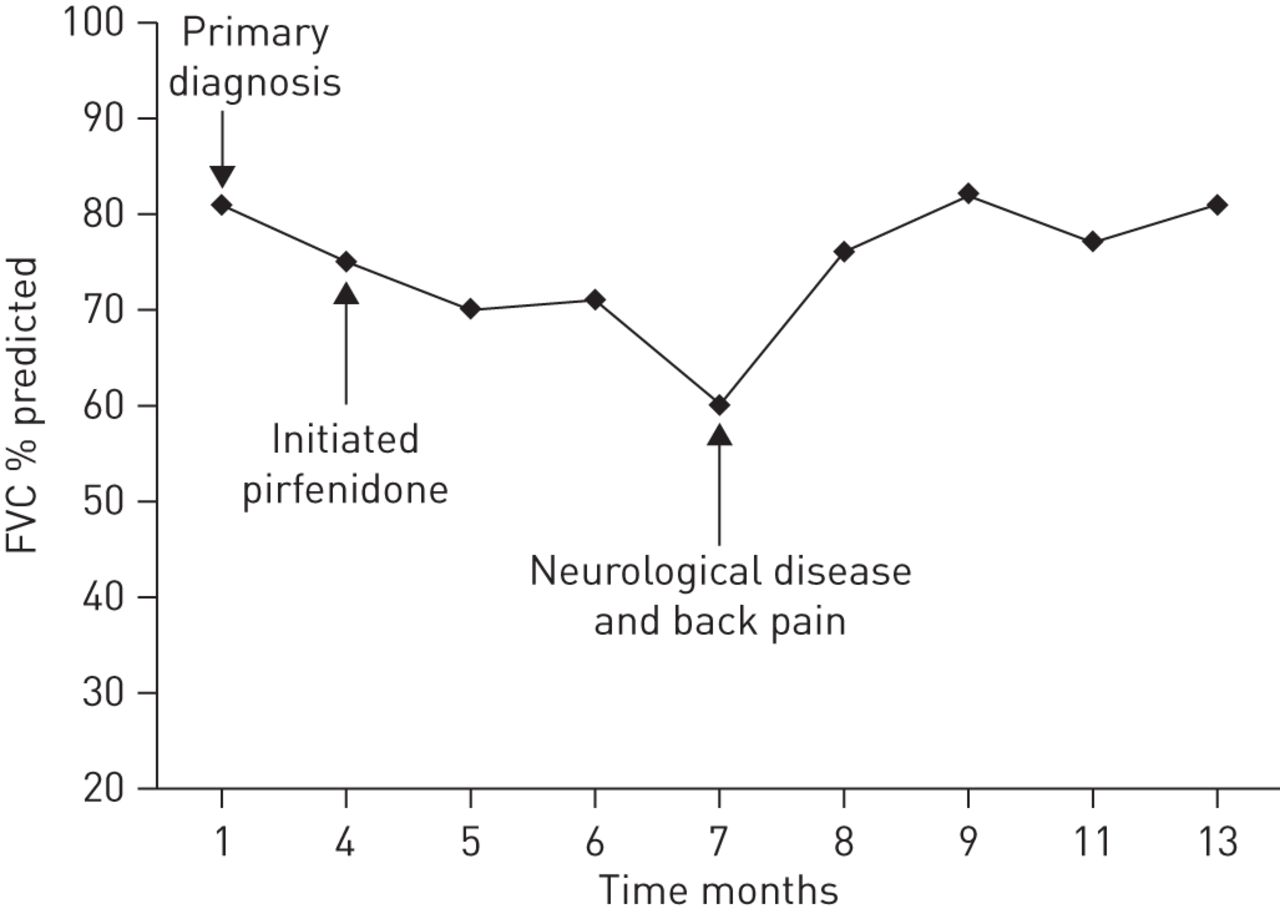
- Figure 3.
Forced vital capacity (FVC) over the course of the disease, some disease stabilisation can be seen following initiation of pirfenidone therapy. However, there was a significant decline in FVC due to neurological disease. After treatment for this disease the patient’s FVC increased again.
- Figure 4.
Chest high-resolution computed tomography scans performed on a) August 16, 2011 and b) September 4, 2012.
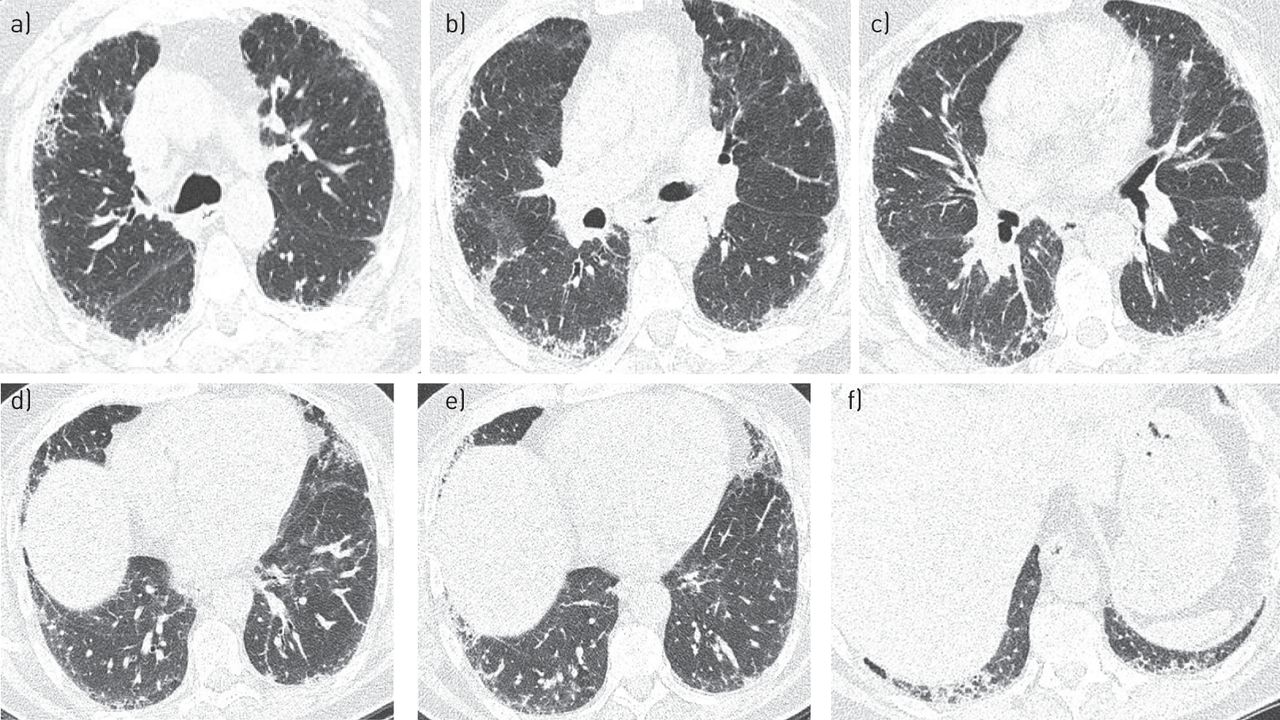
- Figure 5.
Initial high-resolution computed tomography scans performed in November 2011 showing mild reticulation and sub-pleural honeycombing. Representative sections of the lungs from a) the upper to f) the lower zones.
- Figure 6.
Progression in the patient’s pulmonary function tests from 2010 to 2013. a) Forced vital capacity (FVC); b) total lung capacity (TLC); c) diffusing capacity of the lung for carbon monoxide (DLCO); d) 6-min walking distance (6MWD); and e) oxygen saturation (arrow indicates patient was receiving supplemental oxygen). Start: oxygen saturation at the beginning of the 6MWD; end: oxygen saturation at the end of the 6MWD.
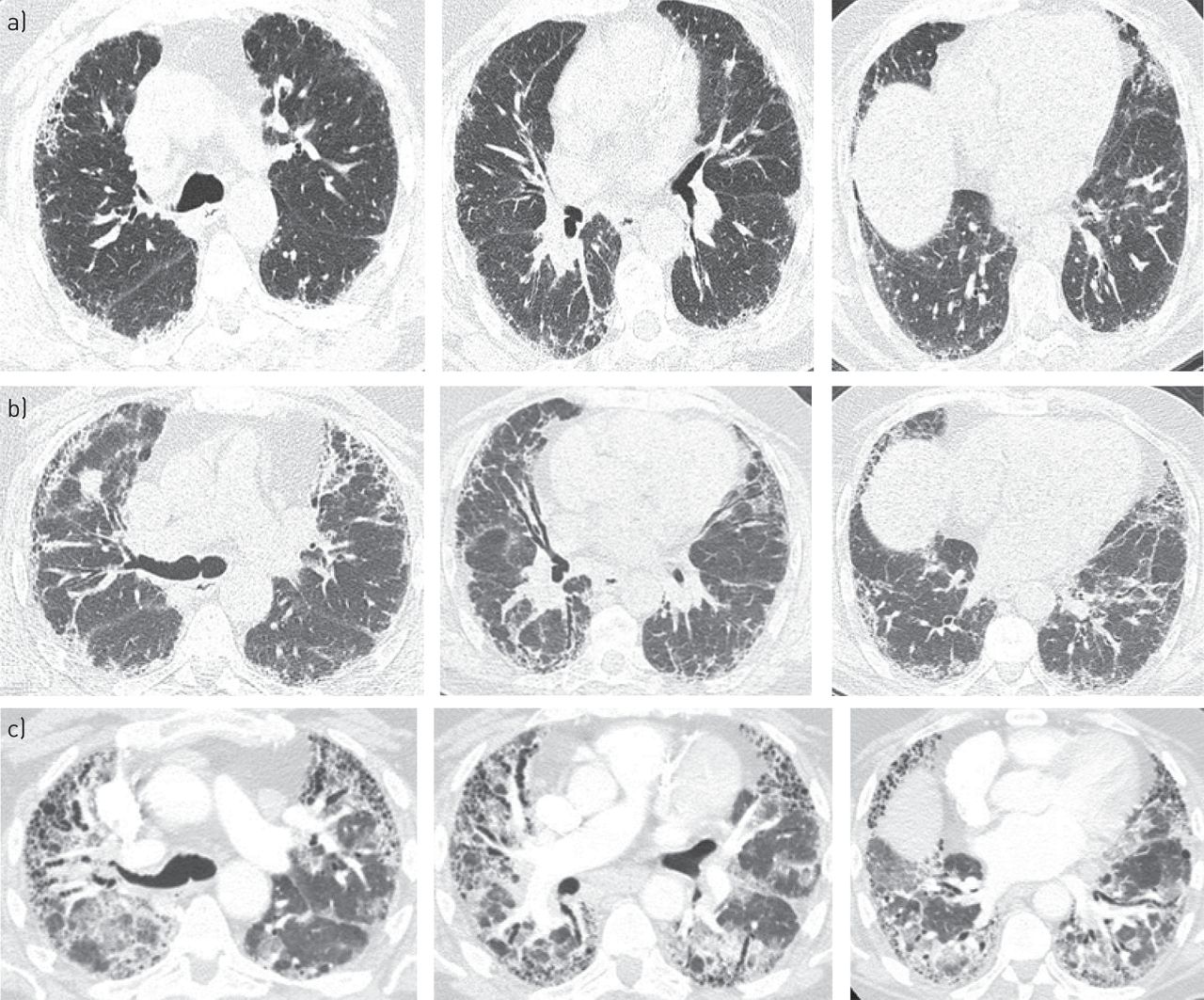
- Figure 7.
Patient computed tomography scans performed in a) 2010, b) 2012 and c) 2013. Representative sections of the lungs from the upper region to the lower region (left to right).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1. Pulmonary function tests
Parameter Absolute % Predicted FVC L 2.5 81 FEV1 L 2.1 82 FEV1/FVC % 84 106 RV L 2.2 124 TLC L 4.7 94 DLCO-SB 36 DLCO–VA 54 FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; RV: residual volume; TLC: total lung capacity; DLCO: diffusing capacity of the lung for carbon monoxide; SB: single breath; VA: alveolar volume.
- Table 2. Pulmonary function tests performed between 2000 and 2012#
Lung function Date of test Feb 1, 2000 May 29, 2006 Oct 31, 2011 April 21, 2012 Sept 15, 2012 Oct 27, 2012 VC % predicted 100 101 80 88 88 88 FVC % predicted 101 103 80 94 91 94 FEV1 % predicted 95 98 72 93 91 92 FEV1/VC % predicted 71 71 65 76 74 67 DLCO % predicted 100 76 32 42 51.2 VC: vital capacity; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; DLCO: diffusing capacity of the lung for carbon monoxide. #: the full dose of pirfenidone was started in November 2011.
- Table 3. Initial pulmonary function tests performed in November 2011
Predicted Patient Normal Range Measured % Predicted Lung volumes TLCpleth L 6.44 >5.07 4.61# 72 VC L 4.13 >3.30 2.97# 72 RV L 2.30 <2.99 1.64 71 RV/TLC 35.8 <46.9 35.6 100 FRC L 2.2 Spirometry FVC L 4.13 >3.30 2.86# 69 FEV1 L 3.19 >2.51 2.30# 72 FEV1/FVC % 77.1 >67.9 80.4 FEF25–75 L·s−1 2.8 >1.5 2.1 75 FEFmax L·s−1 7.8 >4.4 11.0 142 FIFmax L·s−1 3.7 FEF50/FIF50 0.7 MVV L·min−1 124 >91 87# 71 Diffusing capacity DLCO-SB L·min−1·mmHg−1 25.3 >17.3 15.4# 61 DLCO adjusted for Hb 16.0 g·dL−1 14.8# 59 VA L 6.23 >5.07 3.82# 61 Oximetry Oxygen saturation % 96 ≥93 96 Heart rate Pulse beats·min−1 70 TLCpleth: total lung capacity (TLC) measured by plethysmography; VC: vital capacity; RV: residual volume; FRC: functional residual capacity; FVC: functional vital capacity; FEV1: forced expiratory volume in 1 s; FEF25–75: forced expiratory flow at 25–75% of FVC; FEFmax: maximal forced expiratory flow; FIFmax: maximum forced inspiratory flow; FEF50: forced expiratory flow at 50% of FVC; FIF50: forced inspiratory flow at 50% of FVC; MVV: maximum voluntary ventilation; DLCO: diffusing capacity of the lung for carbon monoxide; SB: single breath; Hb: haemoglobin; VA: alveolar volume. #: outside normal limits.
Disclosures
Files in this Data Supplement:









