





Figures
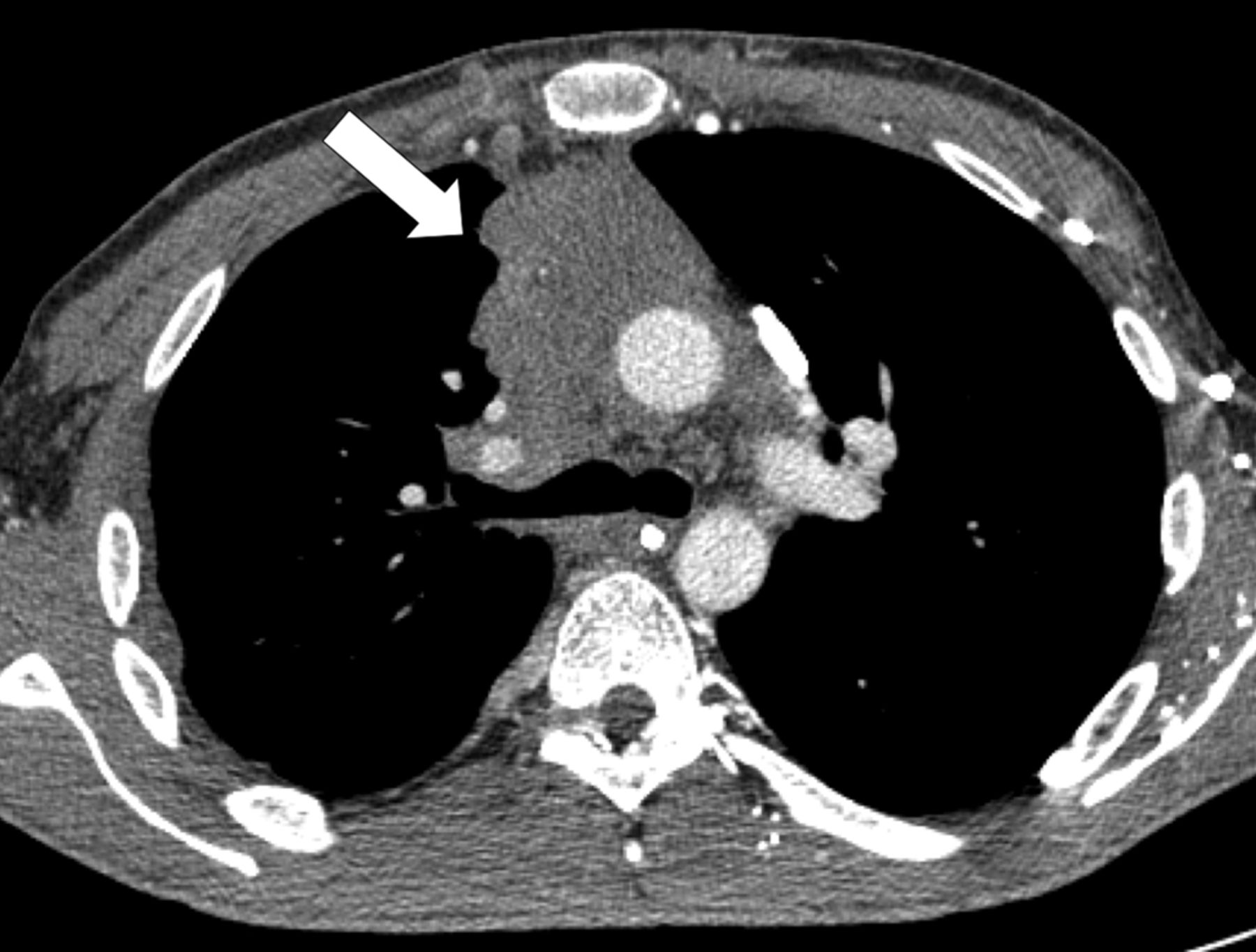
- Figure 1.
Computed tomography scan of a 35-yr-old male who presented with chest pain, showing a mass in the anterior mediastium (arrow). Surgical resection was performed immediately. The tumour was a type AB stage I thymoma. No post-operative treatment was administered.
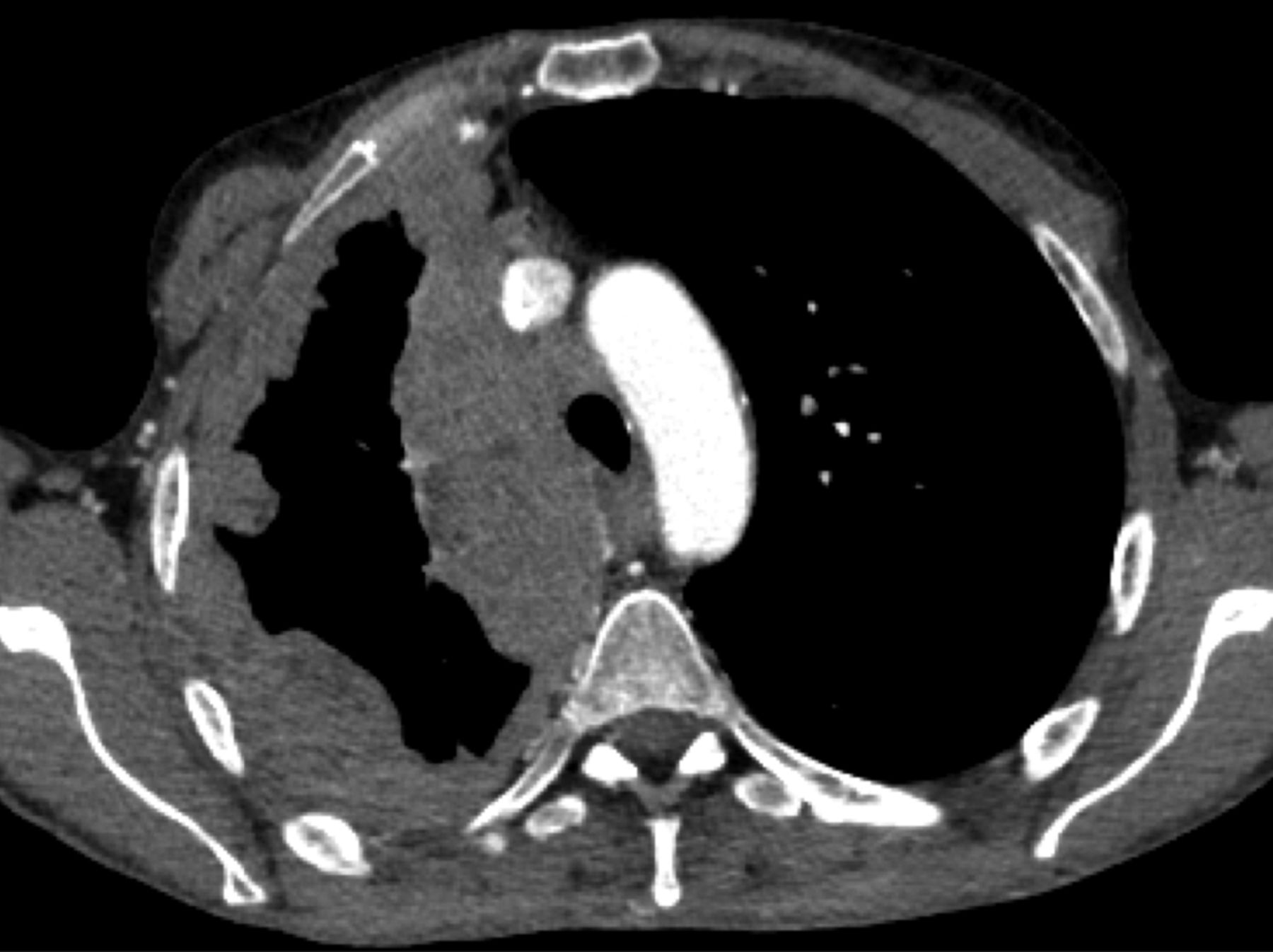
- Figure 2.
Computed tomography scan of a 37-yr-old male who presented with dyspnoea and fatigue. Invasive tumour of the anterior mediastin was observed in the right hemithorax (arrow); percutaneous biopsy showed a type B3 thymoma. The patient received multimodal treatment with primary chemotherapy followed by surgical resection. Resection status was R1. Post-operative radiotherapy was delivered.
- Figure 3.
Computed tomography scan of a 45-yr-old female who presented with shortness of breath and chest pain. “Pseudo-mesotheliomatous” pleural invasion was observed in the right hemithorax; surgical biopsy showed a type B1 thymoma. The patient is currently receiving definite chemotherapy with cyclophosphamide, adriamycin, and cisplatin.


{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1. The World Health Organization histopathological classification of thymic epithelial tumours
Type Pathological features Invasiveness % 10-yr disease-free survival % A Spindle or polygonal cell lacking atypia 10–40 100 Resembles medullary thymoma with paucity of immature thymocytes AB Mixed pattern of type A (lymphocyte-poor) and type B (lymphocyte-rich) thymoma 30–40 100 Immature and mature lymphocytes B1 Thymoma resembling the cortical thymus 45–50 B2 Subtypes B1, B2 and B3 differentiated by an increasing epithelial/lymphocyte ratio and the emergence of atypia 65–70 85 B3 Mature lymphocytes 85–90 35 Thymic carcinoma Epithelial cell atypia 90–95 15 Infiltration Absence of immature lymphocytes Frequent expression of CD5/KIT Adapted from [3].
- Table 2. The Masaoka–Koga International Thymic Malignancy Interest Group staging system
Stage Koga et al. [5] Detterbeck et al. [24] I Grossly and microscopically completely encapsulated tumour Invasion into but not through the capsule
In the absence of capsule, absence of invasion into surrounding tissuesIIa Microscopic transcapsular invasion Microscopic transcapsular invasion (not grossly appreciated) IIb Macroscopic invasion into thymic or surrounding fatty tissue, or grossly adherent to but not breaking through the mediastinal pleura or pericardium Gross extension into normal thymus or perithymic fat surrounding the tumour (microscopically confirmed)
Adherence to pleura or pericardium, with microscopic confirmation of perithymic invasionIII Macroscopic invasion into neighbouring organ (i.e. pericardium, great vessel or lung) Microscopic invasion of the mediastinal pleura (either partial or penetrating the elastin layer)
Microscopic invasion of the pericardium (either partial in the fibrous layer or penetrating through to the serosal layer)
Microscopically confirmed direct penetration into the outer elastin layer of the visceral pleura or into the lung parenchyma
Invasion into the phrenic or vagus nerves (microscopically confirmed)
Invasion into or penetration through major vascular structures (microscopically confirmed)
Adherence (i.e. fibrous attachment) of lung or adjacent organs only if there is mediastinal pleural or pericardial invasion (microscopically confirmed)IVa Pleural or pericardial metastasis Microscopically confirmed separate nodules in the visceral or parietal pleural, pericardial or epicardial surfaces IVb Lymphogenous or haematogenous metastasis Any nodal involvement (e.g. anterior mediastinal, intrathoracic, low/anterior cervical nodes or any other extrathoracic nodes)
Distant metastases (i.e. extrathoracic and outside the cervical perithymic region) or pulmonary parenchymal nodules (not a pleural implant)Adapted from [5] and [24].
- Table 3. Stage-based proposal of therapeutic strategies for thymic epithelial tumours
Stage Treatment strategy# I Upfront surgery Complete resection
Thymoma: no post-operative radiotherapy
Thymic carcinoma: consider post-operative radiotherapyIncomplete resection: post-operative radiotherapy IIa Upfront surgery Complete resection
Type A-B2 thymoma: no post-operative radiotherapy
Type B3 thymoma-thymic carcinoma: consider post-operative radiotherapyIncomplete resection: post-operative radiotherapy IIb Upfront surgery Complete resection
Type A-B1 thymoma: no post-operative radiotherapy
Type B2-B3 thymoma-thymic carcinoma: consider post-operative radiotherapyIncomplete resection: post-operative radiotherapy III–IVa Resectable tumour
Upfront surgery with en bloc resection of the tumour and involved structures
Post-operative radiotherapy with boost on areas of concernUnresectable tumour
Primary chemotherapy
If the tumour becomes resectable:
Surgery with en bloc resection of the tumour and involved structures
Post-operative radiotherapy with boost on areas of concern
If the tumour remains unresectable:
Definite radiotherapyIVb Definite chemotherapy #: expert opinion.
- Table 4. Landmark studies reporting on palliative chemotherapy regimens in advanced thymic malignancies
Primary chemotherapy regimen Subjects n Tumour Design Response rate Subsequent treatment Type Stage Surgery Radiotherapy None Patients Complete resection Chemotherapy Macchiarini [78] CEE 7 T/TC III Phase II 100 100 57 0 0 Berruti [79] ADOC 6 T III–IVA Phase II 83 NR 17 NR NR Rea [80] ADOC 16 T III–IVA Retrosp 100 100 69 0 0 Berruti [81] ADOC 16 T III–IVA Phase II 81 56 56 31 13 Venuta [82] CEE 15 T/TC III Retrosp 66 100 NR NR NR Bretti [83] ADOC/PE 25 T/TC III–IVA Retrosp 72 68 44 NR NR Kim [74] CAPP 22 T III/IVA Phase II 77 100 72 0 0 Lucchi [84] CEE 36 T/TC III–IVA Retrosp 67 69 78 19 3 Jacot [85] CAP 5 T/TC III–IVA Retrosp 75 38 25 50 12 Yokoi [86] CAMP 14 T/TC III, IV Retrosp 93 64 14 14 21 Kunitoh [87] CODE 21 T III Phase II 62 62 43 24 14 Park [88] DDP-Docetaxel 27 T/TC III/IV Phase II 63 70 63 4 25 Chemoradiation Loehrer [72] CAP/54 Gy 23 T/TC III–IVA Phase II 70 0 0 0 100 Wright [37] PE, ADOC, CAP, CEE/45–60 Gy 10 T/TC III–IVA Retrosp 40 100 80 0 0 Data are presented as %, unless otherwise stated. CEE: cisplatin, epirubicin and etoposide; ADOC: adriamycin, cisplatin, vincristine and cyclophosphamide; PE: platin and etoposide; CAP: cyclophosphamide, doxorubicin and cisplatin; CAPP: CAP and prednisone; CAMP: cisplatin, adriamycin and methylprednisolone; CODE: cisplatin, vincristine, adriamycin and etoposid; DDP: cisplatin; T: thymoma; TC: thymic carcinoma; Retrosp: retrospective; NR: not reported.
- Table 5. Selected studies reporting on pre-operative chemotherapy or chemoradiation for locally-advanced thymic tumours
Subjects n Tumour type Study Regimen Agents Doses Response rate % Single-agent chemotherapy Bonomi [90] 21 T/TC Phase II Cisplatin 50 mg·m−2 every 3 weeks 10 Highley [91] 15 T/TC Retrosp Ifosfamide 1.5 g·m−2×5 days every 3 weeks 46 Loehrer [92] 27 T/TC Phase II Pemetrexed 500 mg·m−2 every 3 weeks 17 Combination chemotherapy Fornasiero [93] 32 T Retrosp ADOC Adriamycin 40 mg·m−2 every 3 weeks 85–92 Cisplatin 50 mg·m−2 every 3 weeks Vincristin 0.6 mg·m−2 every 3 weeks Cyclophosphamide 700 mg·m−2 every 3 weeks Loehrer [94] 30 T/TC Phase II CAP Cisplatin 50 mg·m−2 every 3 weeks 51 Adriamycin 50 mg·m−2 every 3 weeks Cyclophosphamide 500 mg·m−2 every 3 weeks Giaccone [95] 16 T Phase II PE Cisplatin 60 mg·m−2 every 3 weeks 56–60 Etoposide 120 mg·m−2×3 days every 3 weeks Loehrer [96] 34 T/TC Phase II VIP Etoposide 75 mg·m−2×4 days every 3 weeks 32 Ifosfamide 1.2 g·m−2×4 days every 3 weeks Cisplatin 20 mg·m−2×4 days every 3 weeks Lemma [97] 46 T/TC Phase II Carbo-Px Carboplatin AUC 5 every 3 weeks 43 Paclitaxel 225 mg·m−2 every 3 weeks Palmieri [98] 15 T/TC Phase II CAP-GEM Capecitabine 650 mg·m−2 b.i.d.×14 days every 3 weeks 40 Gemcitabine 1000 mg·m−2×2 days every 3 weeks Okuma [99] 9 TC Retrosp Cisplatin-irinotecan Cisplatin 80 mg·m−2 every 4 weeks 56 Irinotecan 60 mg·m−2×3 days every 4 weeks T: thymoma; TC: thymic carcinoma; Retrosp: retrospective; ADOC: adriamycin, cisplatin, vincristine and cyclophosphamide; CAP: cyclophosphamide, doxorubicin and cisplatin; PE: platin and etoposide; VIP: etoposide, ifosfamide and cisplatin; Carbo-Px: carboplatin and paclitaxel; CAP-GEM: capecitabine and gemcitabine; AUC: area under the curve.
- Table 6. Growth inhibitory drug effects in cell lines containing KIT mutations identified in thymic carcinomas
Mutation Exon Imatinib Sunitinib Dasatinib Nilotinib E490K 9 ++ +++ NE NE Y553N 11 +++ NE NE NE W557R 11 +++ +++ NE NE V559A 11 +++ +++ NE NE V560del 11 +++ +++ +++ +++ L576P 11 + ++ ++ + P577-D579del 11 NE NE NE NE H697Y 14 + +++ NE NE D820E 17 0 0 ++ ++ NE: not evaluated; 0: half maximal inhibitory concentration (IC50) >1,000 nM, resistance; +: IC50 between 500 and 1,000 nM, low sensitivity; ++: IC50 between 100 and 500 nM, mid-sensitivity; +++: IC50 <100 nM, high-sensitivity.









