





Figures
- Figure 1.
Elastic staining of paraffin-embedded lung tissue. A pulmonary arterial lesion from a patient with idiopathic pulmonary arterial hypertension, illustrating the perivascular lymphocytic infiltrate (centre), a small pulmonary artery (left) and a bronchiole (right). Haematoxylin and eosin elastic stain. Scale bar=100 μm. Reproduced and modified from [13] with permission from the publisher.
- Figure 2.
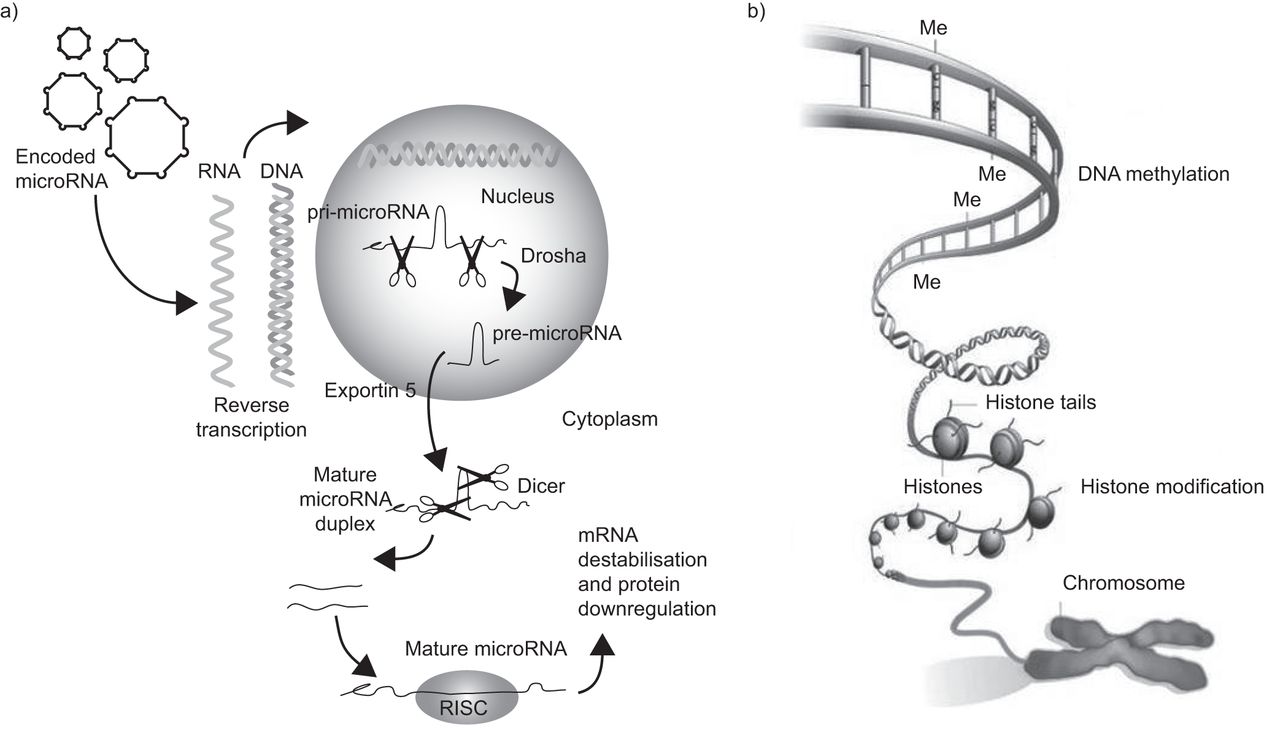
a) Primary microRNA (pri-microRNA) is processed by Drosha in the nucleus to form pre-microRNA. The pre-microRNA enters the cytoplasm via exportin 5 where it is further processed by Dicer into a mature microRNA duplex. One strand of this duplex is incorporated into the RNA-induced silencing complex (RISC) where it binds to the target mRNA. The mRNA is destabilised and, consequently, the protein is downregulated. Reproduced and modified from [14] with permission from the publisher. b) The two main components of the epigenetic code are DNA methylation, in which methyl (Me) groups added to certain bases repress gene activity, and histone modification, where a combination of chemical modifications of the histone “tails” alter the activity of the DNA wrapped around them. Reproduced and modified from [15] with permission from the publisher.
- Figure 3.
Plexiform lesion from a patient with severe pulmonary hypertension demonstrating the exuberant proliferation of cells that comprise the lumen of the small pulmonary artery. Multiple slit-like vascular spaces are all that remain of the original lumen (Haematoxylin-eosin). Reproduced from [19] with permission from the publisher.



{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1. Classification of pulmonary hypertension
1 Pulmonary arterial hypertension 1.1 Idiopathic 1.2 Heritable 1.2.1 Bone morphogenetic protein receptor type II 1.2.2 Activin receptor-like kinase 1, endoglin (with or without hereditary haemorrhagic telangiectasia) 1.2.3 Unknown 1.3 Drug and toxin induced 1.4 Associated pulmonary arterial hypertension 1.4.1 Connective tissue disease 1.4.2 HIV infection 1.4.3 Portal hypertension 1.4.4 Congenital heart disease 1.4.5 Schistosomiasis 1.4.6 Chronic haemolytic anaemia 1.5 Persistent pulmonary hypertension of the newborn 1′ Pulmonary veno-occlusive disease and/or pulmonary capillary haemangiomatosis 2 Pulmonary hypertension due to left heart disease 2.1 Systolic dysfunction 2.2 Diastolic dysfunction 2.3 Valvular disease 3 Pulmonary hypertension due to lung diseases and/or hypoxia 3.1 Chronic obstructive pulmonary disease 3.2 Interstitial lung disease 3.3 Other pulmonary diseases with mixed restrictive and obstructive pattern 3.4 Sleep-disordered breathing 3.5 Alveolar hypoventilation disorders 3.6 Chronic exposure to high altitude 3.7 Developmental abnormalities 4 Chronic thromboembolic pulmonary hypertension 5 Pulmonary hypertension with unclear and/or multifactorial mechanisms 5.1 Haematological disorders: myeloproliferative disorders, splenectomy 5.2 Systemic disorders: sarcoidosis, pulmonary Langerhans’ cell histiocytosis, lymphangioleiomyomatosis, neurofibromatosis, vasculitis 5.3 Metabolic disorder: glycogen storage disease, Gaucher disease, thyroid disorders 5.4 Others: tumoural obstruction, fibrosing mediastinitis, chronic renal failure on dialysis Reproduced and modified from [1] with permission from the publisher.









