





Figures
- Figure 1.
The spectrum of pulmonary aspergillosis.
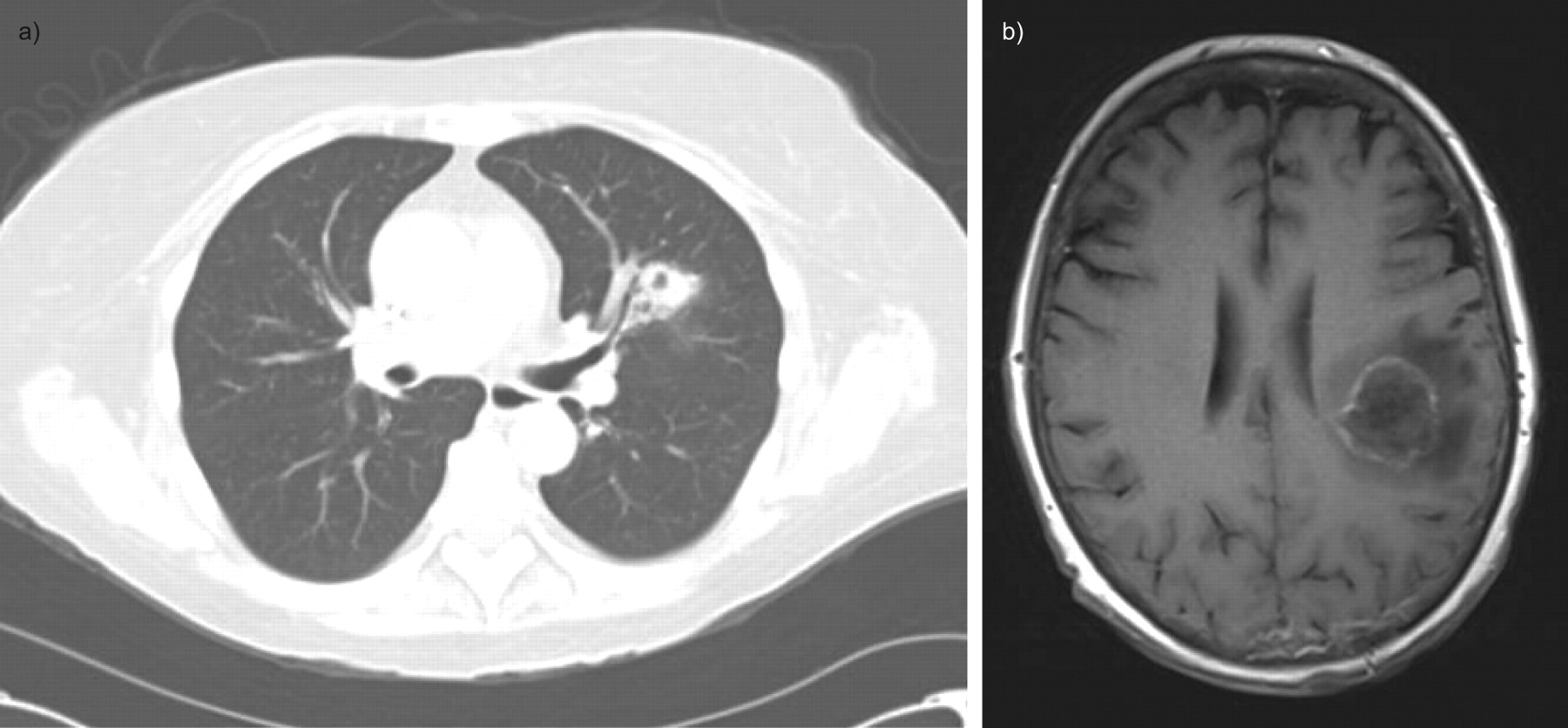
- Figure 2.
a) Chest computed tomography image showing left upper lobe cavitary lesion consistent with invasive pulmonary aspergillosis (IPA) in an allogeneic haematopoietic stem-cell transplantation recipient. b) Brain magnetic resonance image from the same patient showing left parietal ring enhancing lesion due to disseminated IPA.
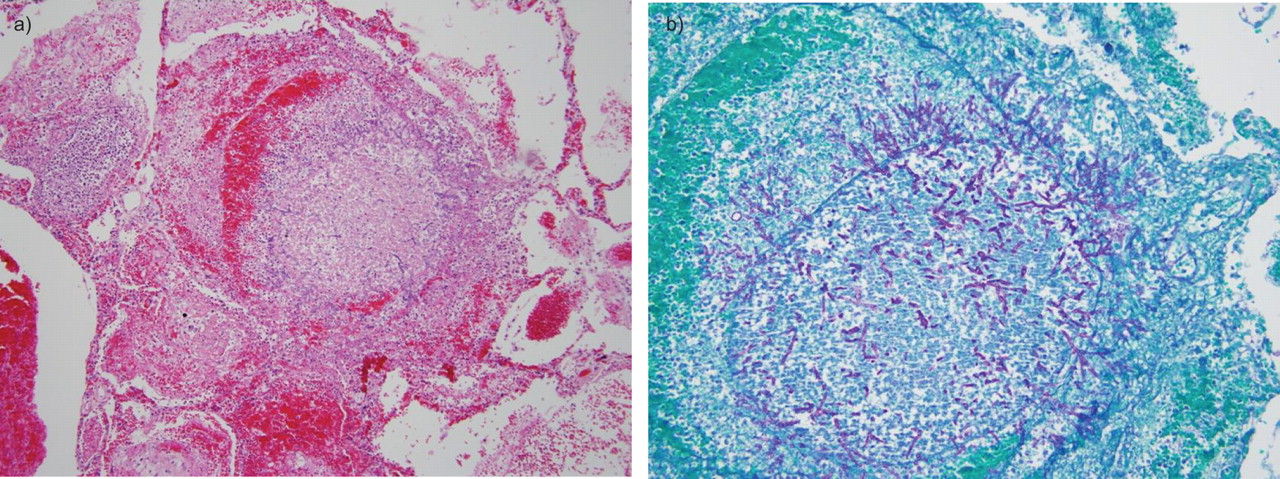
- Figure 3.
Invasive pulmonary aspergillosis. a) Pulmonary parenchyma with necrosis and pulmonary haemorrhage and Aspergillus hyphae (haematoxylin and eosin 100×). b) Branching Aspergillus hyphae involving lung parenchyma (Grocott Methenamine silver fungus stain 200×). Images courtesy of Dr. Mousa Al-Abbadi (East Tennessee State University, Johnson City, TN, USA).
- Figure 4.
Chest computed tomography image showing a right upper lobe aspergilloma in a patient with sarcoidosis.
- Figure 5.
Chest computed tomography image showing central bronchiectasis in a patient with allergic bronchopulmonary aspergillosis.
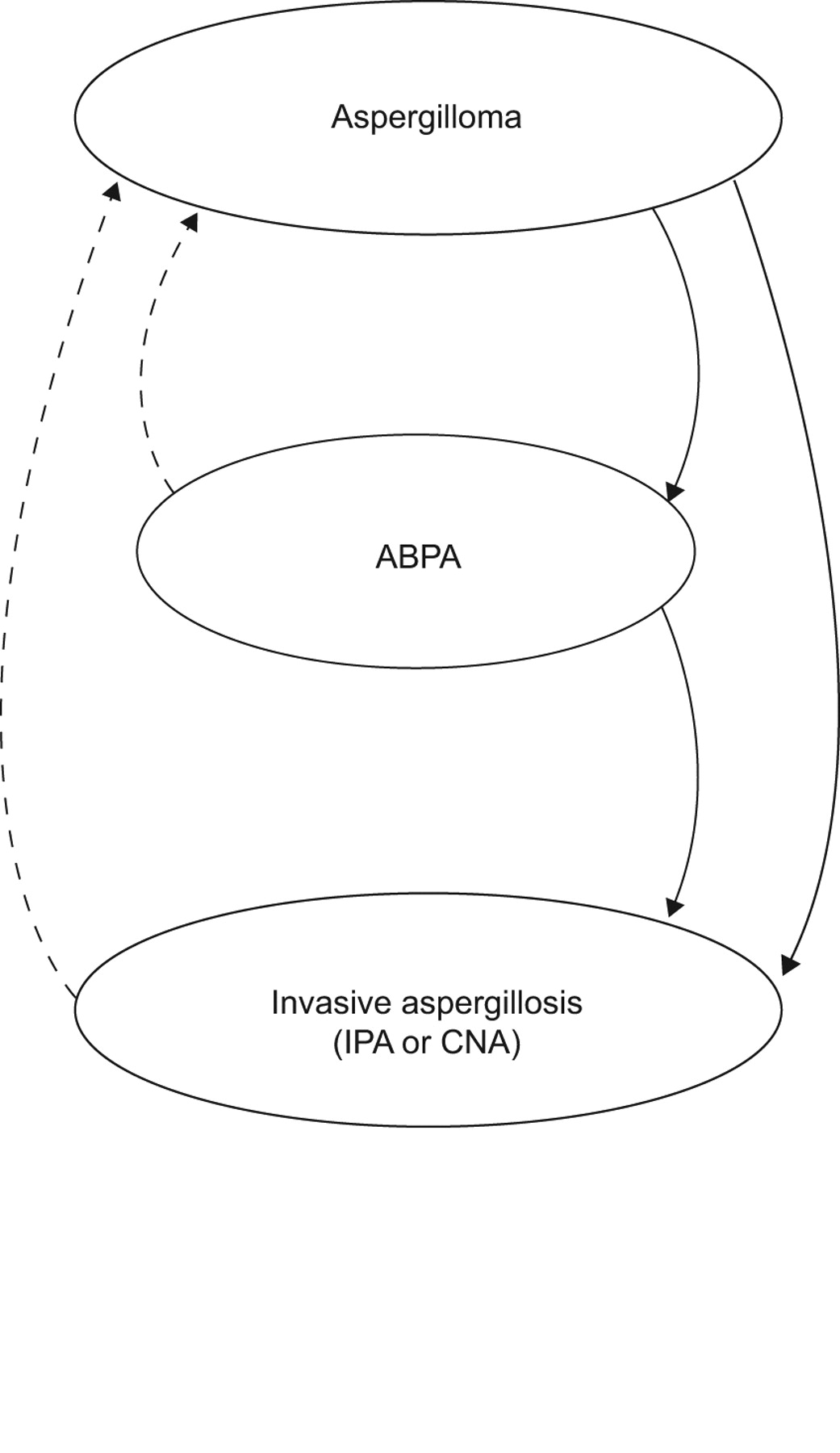
- Figure 6.
Clinical scenarios of Aspergillus overlap syndromes in the lungs. ABPA: allergic bronchopulmonary aspergillosis; IPA: invasive pulmonary aspergillosis; CNA: chronic necrotising aspergillosis.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1. Classical risk factors for invasive pulmonary aspergillosis
Prolonged neutropenia (<500 cells·mm−3 for >10 days) [10] Transplantation (highest risk is with lung transplantation and HSCT) [11–14] Prolonged (>3 weeks) and high-dose corticosteroid therapy [10, 15, 16] Haematological malignancy (risk is higher with leukaemia) [5, 7] Chemotherapy [5, 7, 17] Advanced AIDS [18–21] Chronic granulomatous disease [22] HSCT: haematopoietic stem-cell transplantation.
- Table 2. Diagnostic criteria for invasive pulmonary aspergillosis
Diagnosis Criteria Proven Histopathological or cytopathological examination of lung tissue showing hyphae from needle aspiration or biopsy specimen with evidence of associated tissue damage
OR
positive culture result for Aspergillus from a sample obtained by sterile procedure from the lung
AND
clinically or radiologically abnormal site consistent with infectionProbable Host factor (table 1)
AND
mycological evidence (positive Aspergillus microscopy or culture from the sputum or BAL or positive antigen assay#)
AND
clinical criteria consistent with infection¶Possible Host factor (table 1)
AND
clinical criteria consistent with the infection¶BAL: bronchoalveolarlavage. #: Positive antigen assay: galactomannan antigen detected in plasma, serum, BAL fluid or cerebrospinal fluid, or β-d-glucan detected in serum. ¶: Clinical criteria: new characteristic infiltrates on computed tomography imaging (dense, well-circumscribed lesion(s) with or without a halo sign, air-crescent sign, or cavity), tracheobronchitis seen by bronchoscopy, or noncharacteristic new infiltrates with a specific pulmonary symptom or sign (such as pleural rub, pleural pain, haemoptysis). Adapted from [117].
- Table 3. Treatment recommendations for pulmonary aspergillosis
Disease Primary treatment Other treatments Invasive pulmonary aspergillosis Voriconazole [119–123] Alternative therapy: liposomal amphotericin B [124] Continuation therapy: voriconazole or itraconazole [122, 123] Salvage therapy: echinocandin or posaconazole [125–127] Chronic necrotising aspergillosis Voriconazole [120, 123] Alternative therapy: itraconazole [128, 129] Severe cases: intravenous voriconazole or liposomal amphotericin B [123, 128, 130] Consider surgical resection [130] Aspergilloma Observation [123] Bronchial artery embolisation [131] Surgical resection [132–135] Consider itraconazole [136–138] Allergic bronchopulmonary aspergillosis Corticosteroids [139–142] Itraconazole or voriconazole as steroid-sparing agents [143–146] - Table 4. Diagnostic criteria for chronic necrotising aspergillosis
Diagnostic criteria Characteristics Clinical Chronic (>1 month) pulmonary or systemic symptoms, including at least one of: weight loss, productive cough or haemoptysis No overt immunocompromising conditions (e.g. haematological malignancy, neutropenia, organ transplantation) Radiological Cavitary pulmonary lesion with evidence of paracavitary infiltrate New cavity formation, or expansion of cavity size over time Laboratory Elevated levels of inflammatory markers (C-reactive protein, plasma viscosity or erythrocyte sedimentation rate). Isolation of Aspergillus spp. from pulmonary or pleural cavity, or positive serum Aspergillus precipitin test. Exclusion of other pulmonary pathogens, by results of appropriate cultures and serological tests, that are associated with similar disease presentation, including mycobacteria and endemic fungi Adapted from [186].
- Table 5. Diagnostic criteria for allergic bronchopulmonary aspergillosis
Asthma Immediate skin reactivity to Aspergillus Serum precipitins to Aspergillus fumigatus Increased serum IgE and IgG to Aspergillus fumigatus Total serum IgE >1000 IU·mL−1 Current or previous pulmonary infiltrates Central bronchiectasis Peripheral eosinophilia (1000 cells·μL−1) lg: immunoglobulin. Adapted from [231, 233].









