





Abstract
This review is the summary of a workshop on the role of distal airways in chronic obstructive pulmonary disease (COPD), which took place in 2009 in Vence, France.
The evidence showing inflammation and remodelling in distal airways and the possible involvement of these in the pathobiology, physiology, clinical manifestations and natural history of COPD were examined. The usefulness and limitations of physiological tests and imaging techniques for assessing distal airways abnormalities were evaluated.
Ex vivo studies in isolated lungs and invasive measurements of airway resistance in living individuals have revealed that distal airways represent the main site of airflow limitation in COPD. Structural changes in small conducting airways, including increased wall thickness and obstruction by muco-inflammatory exudates, and emphysema (resulting in premature airway closure), were important determinants of airflow limitation. Infiltration of small conducting airways by phagocytes (macrophages and neutrophils), dendritic cells and T and B lymphocytes increased with airflow limitation. Distal airways abnormalities were associated with patient-related outcomes (e.g. dyspnoea and reduced health-related quality of life) and with the natural history of the disease, as reflected by lung function decline and mortality.
These data provide a clear rationale for targeting distal airways in COPD.
- Airway inflammation
- airway remodelling
- alveoli
- bronchioles
- chronic obstructive pulmonary disease
- distal airways
Chronic obstructive pulmonary disease (COPD) is characterised by airflow limitation that is progressive and poorly reversible. In the late 1960s, using retrograde airway catheterisation in isolated lungs from normal subjects and COPD patients, Hogg et al. [1] reported that distal airways were the main site of airflow limitation. Further evidence came from studies using fibreoptic bronchoscopy with an intrabronchial catheter for invasive measurement of airways resistance in living humans. Yanai et al. [2] have shown that distal airways resistance was significantly increased in patients with chronic airflow obstruction, including COPD subjects. Despite recognition that distal airways are important in the pathophysiology of COPD, current inhaled therapies mostly deposit in proximal airways [3]. A hypothesis is that the limited efficacy of current inhaled therapies in modifying the natural history of COPD [4–6] is related, at least in part, to their lack of action at the main site of airflow limitation (distal airways).
This article is a summary of a workshop on the role of distal airways in COPD, which took place in November 2009 in Vence, France. Data obtained during the workshop were updated with articles published in 2010. First, we reviewed data exploring structural abnormalities and inflammatory changes in distal airways. Then we examined the usefulness of physiological tests and imaging in assessing distal airways in COPD subjects. We also examined the relationship between distal airways impairment and patient-related outcomes, decline in lung function and survival in subjects with COPD. Finally, we reviewed the limited numbers of studies that have been performed on the effects of: 1) oral therapies, and 2) inhaled therapies with extrafine particles that deposit in both proximal and distal airways, on distal airways abnormalities.
INVESTIGATING STRUCTURAL ABNORMALITIES AND INFLAMMATION IN DISTAL AIRWAYS
In humans, conducting airways divide into 24 generations, including the trachea. Distal airways are usually defined as non-cartilaginous conducting airways with an internal diameter <2 mm (approximately corresponding to eight generations of airways down to terminal and respiratory bronchioles) and alveoli. A more detailed description of the anatomy of distal airways can be found in a review article by Burgel et al. [7]. Inflammatory changes and structural abnormalities in distal airways of COPD patients have proven difficult to explore due to their localisation deep within the thoracic cavity. Strengths and weaknesses of various methods for assessing these changes will be discussed later.
Pathologic examination of airway tissues obtained at autopsy or at surgery has provided a major source of information for assessing structural changes and inflammation in distal airways of COPD patients. Interpretation of data obtained at autopsy is subject to caution because some of the changes observed may have occurred post mortem and because careful clinical characterisation of patients is usually not available. Data obtained in patients undergoing surgical lung resection for lung cancer may be biased by the presence of cancer and are limited to COPD subjects with moderate airflow limitation. More recently, with the development of lung volume reduction surgery (LVRS) for severe emphysema, Hogg et al. [8] were able to study subjects with more severe COPD, but from a predominant emphysema phenotype. This approach provided correlation between structural abnormalities and airflow limitation. The limitations are obviously a specific phenotype that may not represent most subjects with severe COPD, and are due to the fact that these studies are, by nature, cross-sectional. Nevertheless, landmark studies comparing pathological findings to physiological measurements have had a determinant impact on our current understanding of the pathobiology of distal airways involvement in COPD [8, 9].
Fibreoptic bronchoscopy is less invasive than surgery and may be repeated overtime. Transbronchial biopsies, which are necessary to sample distal airways, may result in serious adverse effects (pneumothorax and haemoptysis), especially in COPD subjects. Bronchoscopy is a procedure which is not used in the understanding of structural abnormalities in distal airways of COPD subjects. Endobronchial biopsies are safer to perform, but it has not been firmly established whether data observed in biopsies of proximal airways mimic findings in distal airways. Bronchoalveolar lavage (BAL) is useful in sampling inflammatory cells in distal airways [10], even if extensive emphysema may be associated with a low BAL fluid recovery [11]. Various mediators (e.g. cytokines, chemokines, lipid molecules and oxidants) can be measured in BAL, although it is not possible to distinguish the site of production of these molecules (e.g. bronchioles versus alveoli versus recruited inflammatory cells). Fluorescence micro-imaging of the alveolar ducts and sacs during bronchoscopy enables accurate exploration of the distal lung in vivo [12]. Using a 1.4-mm miniprobe introduced into the bronchoscope working channel and advanced distally to the alveoli, Thiberville et al. [12] were able to obtain acinar micro-imaging from individual acini within the lungs and identify structural abnormalities in airway walls, as well as recruited inflammatory cells. Although fascinating, the overall contribution of this technique to the understanding of distal airways abnormalities in COPD remains to be established.
Investigators have developed less invasive techniques to examine inflammatory changes in COPD. Induced sputum is a simple, reproducible and noninvasive method to assess airway inflammatory cells and mediators [13]. Unfortunately, induced sputum predominantly explores the proximal airways. Overall, we cannot identify products originating from proximal versus distal airways. Exhaled nitric oxide (NO) has been proposed to monitor inflammatory changes in asthmatic airways, and cigarette-smoke exposure reduces exhaled NO [14]. However, exhaled NO at constant expiratory flow is not selective for distal versus proximal airways. Analysis of the relationship between exhaled NO and expiratory flow allows derivation of the alveolar NO concentration, which is more closely related to abnormalities in distal airways. However, no difference in alveolar NO concentrations was found between smokers and COPD subjects, suggesting that cigarette-smoke exposure is the main determinant of reduced alveolar NO in COPD, thus limiting the usefulness of this technique [15]. Analysis of exhaled breath condensate, including PH measurement, has been proposed for various biomarkers in COPD subjects but the reproducibility is problematic and the findings are not selective for distal versus proximal airways [16].
Structural abnormalities in COPD distal airways
Structural abnormalities are found in small conducting airways (bronchioles <2 mm in diameter), alveoli and adjacent pulmonary arteries (fig. 1).

Representative photomicrograph of small airways abnormalities in a subject with chronic obstructive pulmonary disease. A narrowed small conducting airway with thickened airway wall (W) is shown. The airway lumen (L) is filled with mucins and inflammatory cells. The arrowheads indicate loss of alveolar attachments. Scale bar = 50 μm.
Small conducting airways
Small conducting airways are a major site of airflow limitation in subjects with COPD [1]. Resistance to airflow varies with the fourth power of the airway radius. Factors that reduce airway radius, including increased thickness of the airway walls (which contain epithelium, lamina propria, airway smooth muscle and adventitia) and luminal obstruction by muco-inflammatory exudates, are independent determinants of airflow limitation in COPD subjects [8].
The airway epithelium is morphologically abnormal in small conducting airways of COPD subjects. Increased epithelial thickness, probably related to squamous metaplasia and goblet cell hyperplasia, is a characteristic finding in COPD subjects with severe airflow limitation (Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage III and IV) [8]. Squamous metaplasia has been described in proximal [17] and distal [9] airway epithelium of smokers. In proximal airway epithelium, squamous metaplasia was correlated with the intensity of active tobacco smoking (packs per day) [17] and was present in 46% of active smokers versus 23% of ex-smokers [18], suggesting a closer relationship with active smoking than cumulative smoking. In a seminal study, Cosio et al. [9] have reported an increase in the extent of squamous metaplasia in small conducting airways with lung function deterioration (decreased forced expiratory volume in 1 s (FEV1)). These data have been recently confirmed by Araya et al. [19] who reported increased epithelial immunostaining for involucrin (a marker of squamous metaplasia) in 22 COPD subjects compared with 12 nonsmokers. Goblet cell hyperplasia is usually observed in the epithelium of proximal airways in (ex-) smokers with COPD [20, 21]. In the epithelium of small conducting airways, goblet cell hyperplasia has been reported in some studies [22–25], but was not found in others [26–28]. We have suggested that these inconsistent findings may be related to rapid secretion of mucus within the airway lumen, resulting in its disappearance from the epithelium [29].
Small airway epithelium may play various important roles in COPD pathophysiology. First, increased epithelial thickness, which contributes to airway wall thickness and reduced airway radius, is associated with airflow limitation in COPD subjects [8]. Secondly, Araya et al. [19] recently suggested that squamous airway epithelium promoted peribronchiolar fibrosis via an increased secretion of interleukin-1β which activated αv-β8 integrin on fibroblast, resulting in increased transforming growth factor (TGF)-β secretion and fibrosis. Thirdly, secretion of epithelial mucins (i.e. MUC5AC and MUC5B [26]) from hyperplastic goblet cells probably contributes to lumen obstruction by muco-inflammatory exudates [8]. Finally, small airway epithelium may promote the recruitment of neutrophils, macrophages and T lymphocytes via the secretion of specific chemoattractants [30–33].
Peribronchiolar fibrosis also contributes to the increased airway wall thickness in small conducting airways [9, 28, 34]. Mechanisms leading to peribronchial fibrosis are not clearly delineated. Chronic smoke exposure in guinea pigs is associated with increased airway wall thickness and increased amounts of thick collagen fibres in the walls of the small airways [35]. A hypothesis generated from animal models is that cigarette smoke drives small airways remodelling by induction of pro-fibrotic growth factors (e.g. connective tissue growth factor, platelet-derived growth factor-β and TGF-β1) the airway wall [36, 37]. These growth factors, which have also been found in small airways of COPD subjects using microarray analyses [38, 39], may contribute to peribronchial fibrosis.
Abnormalities in airway smooth muscle are less marked in the small airways of COPD subjects than in asthmatics [40]. Hogg et al. [8] reported only a modest increase in smooth muscle volume in the airway wall of COPD subjects with severe airflow limitation. Corsico et al. [41] studied pathological changes in medium and small airways in relation to lung function tests in 22 non-asthmatic subjects undergoing lung resection. The authors reported that total airway wall thickness was significantly correlated with FEV1/forced vital capacity (FVC), reactivity to methacholine (R2 = 0.26) and slope of linear regression of FVC against FEV1 values recorded during the methacholine challenge. No significant correlation was found between airway smooth muscle thickness and lung function measurements [41].
Obstruction of small conducting airways by muco-inflammatory exudates has been initially identified using autopsy tissues [42]. However, it has long been considered as a post mortem artefact. It is only recently that Hogg et al. [8] reported that obstruction with muco-inflammatory exudates was independently associated with airflow limitation in COPD subjects undergoing lung resection. Caramori et al. [26] confirmed that mucus exudates were found in the small conducting airways of living COPD subjects.
Alveoli
Destruction of alveolar walls is the hallmark of emphysema. Loss of alveolar attachments is associated with destabilisation of small conducting airways, leading to premature airway closure during expiration and airflow limitation. Multiple mechanisms have been implicated in the pathogenesis of alveolar destruction: protease-antiprotease imbalance, resulting in proteolytic degradation of alveolar extracellular matrix by neutrophil and macrophage proteases, has been suggested [43, 44]. More recently, abnormalities of survival programmes in alveolar epithelial cells and/or endothelial cells have been reported. The implication of premature cellular senescence [45], increased apoptosis [46–50], and autoimmunity [51, 52] has been suggested. Regardless of the mechanisms, loss of elastic fibres is an important feature of alveolar abnormalities in COPD subjects, leading to emphysema. Importantly, Black et al. [53] have recently reported a similar loss of elastic fibres in small conducting airways of COPD subjects, suggesting that small conducting airways may also disappear. A major question resulting from these findings relates to the number of small conducting airways in COPD subjects [54, 55]. Hogg et al. [55] have reported preliminary data using micro-computed tomography (CT) in isolated lungs and suggested a reduction in the number of small conducting airways in subjects with centrilobular emphysema. Decreased numbers of small conducting airways may contribute to increased resistance in small airways because mathematical computation indicates that a 50% reduction in the number of small conducting airways will result in a two-fold increase in resistance.
Pulmonary arteries
Structural abnormalities are not limited to small conducting airways and alveoli, but also extend to small pulmonary arteries (diameter <500 μm). Abnormalities in pulmonary arteries were long considered a consequence of hypoxaemia, occurring only in subjects with very severe disease. However, smooth muscle cell proliferation, and elastin and collagen deposition were found in the thickened intimas of pulmonary arteries in moderate COPD patients and in smokers with normal lung function, suggesting that these abnormalities may originate at an early stage in cigarette smoke-induced respiratory disease [56]. Abnormalities in pulmonary arteries may result in gas exchange impairment [57] and, in a minority of subjects, in pulmonary hypertension [58].
DISTAL AIRWAYS INFLAMMATION IN COPD
Cigarette smoke triggers an inflammatory response that involves innate immune mechanisms in all subjects and may involve adaptive immune response in a subset of susceptible subjects [52]. Thus, increased inflammatory cells are found in both proximal and distal airways of COPD subjects [59]. Hogg et al. [8] have studied a large number of subjects with COPD (n = 159) and reported that the percentage of small conducting airways containing neutrophils, macrophages, CD4+ and CD8+ T lymphocytes, B lymphocytes and lymphoid follicles increased with the severity of airflow limitation (as assessed by GOLD stages).
A limited number of studies suggest that inflammatory cell recruitment is associated with structural abnormalities. Saetta et al. [44] reported that the loss of alveolar attachments in small conducting airways correlated with leukocytes infiltration, suggesting that leukocyte-derived proteases were involved in alveolar disruption. Turato et al. [60] performed a pathological study comparing inflammatory infiltrates in distal airways to radiological emphysema and lung function measurements in subjects with severe COPD (n = 9) and smokers with normal lung function or mild airflow limitation (n = 9). The authors reported that increased number of leukocytes (mainly CD4+ and CD8+ T lymphocytes) correlated with reduced expiratory flow, lung hyperinflation, carbon monoxide diffusion impairment and radiological emphysema, suggesting a role for this inflammatory response in the clinical progression of the disease [60].
Neutrophils are recruited in the distal airways of smokers and COPD subjects, as reported in many studies using BAL or immunocytochemistry [8, 61]. O'Donnell et al. [62] reported that neutrophil counts in induced sputum were significantly associated with high-resolution CT indices of distal airways dysfunction (expiratory/inspiratory mean lung density ratio), but not with the severity of emphysema. Neutrophils have also been implicated in mucus hypersecretion in conducting airways [63], including small conducting airways [25].
Large numbers of macrophages were found in distal airways of COPD subjects [64] and these macrophages may exhibit distinct phenotypes. Frankenberger et al. [65] reported that 46% of macrophages isolated from induced sputum were small macrophages, whereas these cells represented only 7% of macrophages in healthy subjects. Small sputum macrophages had a pro-inflammatory phenotype characterised by increased CD14 and human leukocyte antigen-DR expression and by higher levels of tumour necrosis factor-α secretion [65]. In contrast, Lofdahl et al. [10] reported lower alveolar macrophage expression of CD86 (a co-stimulation molecule) and CD11a (an adhesion molecule) in COPD, implying a reduced antigen-presenting function. Phenotypic modifications of macrophages in COPD will require further studies.
Natural killer cells, which belong to the innate immune response, were increased in proximal airways [66], but not in alveoli of COPD subjects [48]. Few studies exist on the presence and potential roles of these cells in the airways of COPD subjects.
Infiltration by T lymphocytes has been described in proximal airways [67], in small conducting airways [68] and in alveoli [64]. These lymphocytes were predominantly CD8+ T lymphocytes in both proximal [69] and distal airways [68, 70]. Careful examination of distal airways in COPD subjects has revealed that CD8+ T lymphocytes were present in small conducting airways, in alveoli and close to pulmonary arteries [70, 71]. Increases in both CD4+ and CD8+ T lymphocytes were reported in alveolar walls of COPD subjects [48, 64]. Using BAL fluid analysis, studies have confirmed that CD8+ T lymphocytes were increased in distal airways of COPD subjects [72]. CD8+ T-cells were mature cells characterised by a high CD45RA/CD45R0 ratio. Compared with never-smokers, smokers with normal lung function showed a prominent up-regulation of T-regulatory cells that was absent in patients with COPD [73]. Recruitment of CD8+ T lymphocytes may be triggered chemokines secreted by the epithelium of small conducting airways. Saetta et al. [32] reported that CD8+ T lymphocytes expressed CXCR3, a chemokine receptor, and that its ligand interferon-induced protein 10/CXCL10 was present in epithelium of small conducting airways in COPD subjects. Because expression of viral protein E1A in alveolar epithelial cells was associated with increased CD8+ T lymphocytes in distal airways, Retamales et al. [74] suggested that CD8+ T lymphocytes could be recruited in response to latent adenoviral infection. Infiltration of CD8+ T lymphocytes in distal airways may also be related to autoimmune mechanisms: recognition of an alveolar epithelial autoantigen by CD8+ T lymphocytes resulted in interstitial pneumonia and emphysema [75]. Accumulation of activated CD8+ T lymphocytes in distal airways of COPD subjects have been associated with various structural abnormalities, suggesting that these cells play major roles in COPD pathophysiology [76]. Thus, CD8+ T lymphocytes secrete proteases (e.g. granzyme and perforins), which were associated with alveolar disruption [77]. In addition, CD8+ T lymphocytes were associated with apoptosis of epithelial and endothelial cells [48], probably via activation of the Fas (CD95)/FasL pathway [78]. Finally, Kim et al. [79] have reported a correlation between CD8+ T lymphocytes and goblet cell hyperplasia in the epithelium of small conducting airways, suggesting a role for CD8+ T lymphocytes in mucus hypersecretion [79].
Dendritic cells are responsible for antigen presentation in small conducting airways, and provide a link between innate and adaptive immunity [59]. Early studies using BAL fluid analysis have shown increased CD1a+ (immature) dendritic cells in smokers (COPD subjects were not studied) [80, 81]. However, no difference in intraepithelial CD1a+ cells was found [81]. Recent studies have explored dendritic cells and their phenotypes in COPD subjects. Demedts et al. [82] reported a significant increase in dendritic cell numbers in the epithelium and adventitia of small conducting airways of COPD subjects compared with never-smokers and smokers without COPD. These authors found that dendritic cell numbers in epithelium and adventitia increased with airflow limitation [82]. Furthermore, lung expression of the dendritic cell chemokine CCL20 was increased in COPD subjects and dendritic cells expressed higher levels of CCR6 (the CCL20 receptor), suggesting a mechanism for dendritic cell recruitment in COPD [82]. A recent cross-sectional study indicated that COPD progression is associated with significant increases in co-stimulatory molecule expression by dendritic cells recovered from human surgical specimens, suggesting maturation of dendritic cells with disease progression [83]. In contrast, Tsoumakidou et al. [84] reported decreased numbers of (mature) CD83+ dendritic cells in small conducting airways and alveoli of COPD subjects. Mature dendritic cells also appeared to be decreased in proximal airways of COPD subjects [85] and in induced sputum of COPD subjects and current smokers without COPD [86]. Thus, further studies are required to clarify our knowledge of dendritic cell maturation and function in distal airways of COPD subjects.
Potential roles of mast cells and eosinophils in distal airways of COPD subjects have been seldom studied. Grashoff et al. [87] reported that intraepithelial mast cells were increased in small conducting airways of COPD subjects, suggesting a role for these cells in the pathogenesis of structural changes leading to airflow limitation. In a recent study, the authors reported that as COPD progresses to severe stages, mast cell populations in the lung undergo changes in density, distribution and molecular expression [88]. Eosinophilic infiltration was reported in proximal airways of COPD subjects during exacerbation [89], especially during virus-induced exacerbations [90], and was also found in proximal airways of COPD subjects with chronic cough and sputum production [91]. In small conducting airways, eosinophilic inflammation was low under stable condition in 15 COPD subjects [87]. Whether eosinophilic inflammation in distal airways is present in COPD subjects with specific phenotypes or during exacerbations is unknown.
PULMONARY FUNCTION TESTS
Spirometry and body plethysmography
The definition of airflow obstruction usually relies upon a post-bronchodilator FEV1/FVC <70% [92]. However, FEV1/FVC provides little information on distal airways [93] and investigators have tried to establish other markers of distal airways impairment using spirometry and/or body plethysmography.
Forced expiratory flow between 25% and 75% of FVC (FEF25–75%) has long been considered a marker of distal airways impairment in COPD subjects [94]. However, the measurement is highly variable, even among normal individuals [95, 96], and lower limit of normal (LLN) decreases with age, as residual standard deviation of predicted values remains constant. Furthermore, this measurement has been shown to correlate poorly with distal airways abnormalities [96, 97]. FEF25–75% is dependent on FVC and, thus, should be interpreted only when FVC is normal. Hansen et al. [95] proposed the use of forced expiratory volume in 3 s (FEV3)/FVC and compared its utility to FEV1/FVC in measuring the effect of smoking on airflow. The authors also calculated the fraction of the FVC that had not been expired during the first 3 s of the FVC (1−FEV3/FVC) to identify the growing fraction of long time-constant lung units [95]. Data were obtained in 3,570 current smokers and 5,938 adult never-smokers, which allowed the mean and LLN values of FEV3/FVC in never-smokers to be established. When associated with older age, FEV3/FVC decreased and 1−FEV3/FVC increased as FEV1/FVC decreased. The LLN of FEF25–75% markedly decreased with age and its use was associated with an unacceptably large number of false-negative results and false-positive results. The authors suggested that 1−FEV3/FVC was useful to characterise distal expiratory obstruction, whereas FEF25–75% should be abandoned [95].
Lung hyperinflation is defined as an abnormal increase in the volume of air remaining in the lungs at the end of spontaneous expiration. The hallmark of COPD is expiratory airflow limitation that results in delayed emptying of the lung and, presumably, in progressive lung hyperinflation. Although no longitudinal study has assessed the natural history of hyperinflation [98], older data suggest that hyperinflation occurs early in the course of COPD [99, 100]. Thus, many COPD subjects have some degree of hyperinflation of the lungs, which is not detected if lung volumes are not measured [101]. Hyperinflation is characterised by an increase in residual volume (RV), functional residual capacity (FRC), end expiratory lung volume (EELV) during exercise or total lung capacity (TLC) and is associated with a decrease in inspiratory capacity (IC; TLC–EELV). These changes are related to: 1) the reduction in lung elasticity related to decrease in elastic recoil (static component), and 2) the increase in airways resistance (dynamic component) resulting in airflow limitation. These mechanisms usually coexist as indicated by a pathological study that found a correlation between the degree of emphysema and small airways thickening in subjects with predominant centrolobular emphysema [102]. Increase in RV was shown to correlate with the degree of inflammation in distal airways [60]. Lung hyperinflation correlates better with dyspnoea and health status than FEV1 and is responsible for excessive loading and functional weakness of inspiratory muscles [103, 104]. FEV1 is an insensitive marker for bronchodilator responsiveness in COPD subjects. Newton et al. [105] studied the acute effects of the short-acting β-agonist salbutamol on flow and volume in subjects with various levels of static hyperinflation. Results indicated that salbutamol reduced hyperinflation even when FEV1 did not improve, and the most impressive results were observed in subjects with the most severe hyperinflation [105]. These data suggested effects of bronchodilators were more closely related to decrease in hyperinflation than to changes in airway resistance [105]. Another possibly important point relates to the relationship of FVC to hyperinflation. Sorkness et al. [97] studied a large cohort of subjects with asthma and found that RV/TLC correlated well with FVC. Although similar data would have to be reproduced in COPD subjects, these data suggests that FVC reduction could be used as a surrogate marker for hyperinflation in the absence of plethysmographic lung volume measurement.
Hyperinflation increases during exercise or hyperventilation and this so-called dynamic hyperinflation may even occur in COPD subjects without hyperinflation at rest. In healthy subjects, EELV and IC remained unchanged during maximal exercise [106]. O'Donnell et al. [106] performed incremental cycle exercise tests in 105 COPD subjects (mean FEV1 37% predicted) and studied the relationships between resting lung volumes and dynamic hyperinflation. During exercise, 80% of patients showed significant dynamic hyperinflation above resting values, which correlated best with IC at rest [106]. Exercise induced dynamic hyperinflation was also found in patients with GOLD stage I COPD and dyspnoea [107]. It was further reported during the 6-min walk test (6MWT) [108, 109]. Reduction in IC during the 6MWT correlated with dyspnoea measured using the modified Medical Research Council (MRC) scale or Borg scale [109]. Treatment with the long-acting β-agonist (LABA) salmeterol for 2 weeks reduced dynamic hyperinflation during exercise and decreased respiratory discomfort, thereby increasing exercise endurance [110]. 6 weeks of treatment with the long-acting antimuscarinic (LAMA) tiotropium was also associated with sustained reductions of lung hyperinflation at rest and during exercise, resulting in improvements in both exertional dyspnoea and exercise endurance [111].
Measurement of total pulmonary resistance is best obtained using an invasive technique that involves an oesophageal balloon to measure pleural pressure. Noninvasive measurement of airway resistance (Raw), which represents the main component of total pulmonary resistance, can be performed using body plethysmography. Airway conductance (Gaw; 1/Raw) and specific airway conductance (sGaw; Gaw/TLC), which is independent of lung volume, can be calculated. Raw is elevated and the predictive value of sGaw was similar to FEF25–75% in lung transplant recipients who subsequently developed bronchiolitis obliterans syndrome [112]. However these variables do not specifically reflect abnormalities in distal airways.
Forced oscillations and impulse oscillometry
Forced oscillation technique consists of applying periodic pressure variations (in the form of random noise or short impulses) during normal tidal breathing, causing variations in respiratory flow. The relationship between pressure variations and flow variations (measured at the mouth) can be used to measure respiratory resistance and respiratory reactance, the real and imaginary part of the pressure–flow relationship, respectively. Reactance is determined jointly by the elastic properties that dominate at low frequencies and the inertial forces that become more important as frequency increases, resulting from the acceleration of the air in the system [113]. The pressures exerted by oscillation frequencies >15 Hz are absorbed before reaching the small conducting airways, whereas for frequencies <10–15 Hz, the oscillation pressures penetrate into the peripheral lung. Therefore, it has been suggested that low-frequency resistance (≤10 Hz) preferentially assesses the small conducting airways, and high-frequency resistance (>16 Hz) representative of the proximal airways. While the location of the transition between the proximal and the small conducting airways has not been clearly determined anatomically, experimental and clinical data are suggestive of distal airways impairment leading to predominant increase in low-frequency resistance [114].
In normal subjects, respiratory resistance (Rrs) is independent of oscillation frequency while respiratory reactance (Xrs) varies with oscillation frequency, being negative at low frequencies where the elastic component predominates, and becoming positive at high frequencies where the inertance phenomenon predominates. The frequency at which reactance is zero (where its two forces cancel out) is called the resonant frequency. In normal subjects it is between 7 and 12 Hz, and it increases in patients with airflow obstruction. Simultaneous application of different frequency components (i.e. the use of composite signals such as pseudorandom noise signals), is preferred [113]. This multifrequency forced oscillation method applies frequencies to the subject that are both above and below the resonant frequency, providing calculated measurements of Rrs and Xrs at different frequencies. Unlike in normal subjects where Rrs is independent of the frequency, if the airways are obstructed Rrs increases at low-oscillation frequencies and increases less at high-oscillation frequencies. In this way, airway obstruction generates a negative frequency dependence of Rrs which is thought to be partly due to heterogeneity in airway obstruction and/or distal airway obstruction. Low-frequency reactance more specifically explores the compliance of distal airways. A strong correlation has been found between total reactance and transpulmonary resistance measured by oesophageal manometry [115].
Resistance and reactance parameters were analysed in a cohort of 79 COPD patients in relation to their GOLD stage [116]. An increase in Rrs (extrapolated to 0 Hz) was observed from stage 1, while moderate to severe stages were distinguished more clearly by Xrs than by Rrs. In the study reported by Kolsum et al. [117], Xrs (5 Hz) and resonant frequency proved to be more closely correlated with other functional parameters than Rrs (5 Hz). An interesting point here is that the fall in FEV1 over 1 yr correlated with a fall in Xrs (5 Hz). Kanda et al. [118] also found a link between COPD stage and Rrs, Xrs and resonant frequency.
The forced oscillation technique was recently used to specifically assess expiratory flow limitation, which is a key element in COPD pathophysiology since it induces dynamic hyperinflation [119]. Dellaca and co-workers [120, 121] validated their application of the forced oscillations in comparison with oesophageal pressure and the reference negative expiratory pressure technique. In patients with an expiratory flow limitation, Xrs (5 Hz) values fall on expiration as the oscillation signal cannot exceed the “choke point”. The same method can also be used to assess the impact of a bronchodilator on expiratory flow limitation [122]. Fall in Xrs during expiration was recently shown to differentiate asthma from COPD, although whole breath values were similar [123]. Finally, it was recently shown that “distal” oscillometry parameters (R5Hz-R20Hz and X5Hz), measured at baseline breathing and at an elevated respiratory rate (40 breaths·min−1), correlated perfectly with the fall of dynamic compliance at 60 breaths·min−1, a reference invasive technique used to assess the distal airways [124]. Impulse oscillometry is also useful for evaluating responses to short- and long-acting bronchodilators and here it is suggested to be more sensitive than spirometry in comparing drugs [125, 126]. The clinical relevance of oscillometry parameters in COPD was recently analysed by Haruna et al. [127]. Dyspnoea (MRC) in particular was more closely correlated with R(5Hz)–R(20 Hz) and X(5Hz) parameters than with FEV1. To date, there are no published data in COPD on oscillometric changes induced by anti-inflammatory drugs (e.g. inhaled corticosteroids), yet the impact of inflammation on reactance is demonstrated by data recently obtained in COPD exacerbations. During the recovery of exacerbations in 39 COPD patients, the most significant physiologic changes were found on oscillometric parameters, particularly Xrs (5 Hz), Xrs (5 Hz) during inspiration (-27%) and Xrs (5 Hz) during expiration (-37%). In contrast, changes in Rrs component were not significant. Similar findings were demonstrated by Stevenson et al. [128]. In addition, patients improving their Xrs (5 Hz) were also those with FEV1 and IC increase [128]. Finally, expiratory flow limitation can be detected noninvasively with impulse oscillometry by the fall in expiratory reactance with respect to inspiratory reactance. In a recent study by Dellaca et al. [122], flow limitation detected by this criterion was shown to disappear after bronchodilator administration in eight out of 20 flow-limited patients at baseline. The obvious advantage of this noninvasive method should prompt other studies to determine its clinical relevance in COPD, both for therapeutic assessments and follow-up.
Nitrogen washout tests
Nitrogen washout tests are simple, noninvasive tests aimed at quantifying the efficacy of mixing between inspired and lung resident gases, which have the potential to investigate distal airway function. Single breath washout is an old technique that consists of analysing nitrogen concentration in exhaled air after a single inspiration of 100% oxygen. Increase in closing volume (CV; phase IV) or in closing capacity (CC+RV) and increase in phase III slope (alveolar slope) have been associated with abnormalities in distal airways [9, 99, 129], and correlated with the severity of airflow limitation in COPD subjects [130]. Cosio et al. [9] reported a greater sensitivity of phase III slope over FEF25–75% in smokers with mild inflammatory changes in small airways. The phase III slope of the washout reflects concentration differences that are being generated even in normal lungs, owing to the presence of structural heterogeneity in both the conductive and acinar lung zones. During a washout test, conductive and acinar airways are intrinsically linked to convective and diffusive gas transport, respectively, and the resulting quasi-static diffusion front of inspired gas functionally separates these two compartments [131].
A multiple breath nitrogen washout (MBW) offers the possibility to quantify both conductive and acinar ventilation heterogeneity because the phase III slope, when normalised for the decreasing mean expired nitrogen concentration, increases as the MBW progresses. Because conductive heterogeneity produces a normalised slope (Sn), which increases steadily as a function of lung turnover (tidal volume to FRC ratio), and acinar heterogeneity produces a horizontal Sn asymptote within the first lung turnovers, the Sn versus lung turnover plot can be readily decomposed in its conductive and acinar components [132]. The index of conductive ventilation heterogeneity (Scond) is computed as the rate of rise of Sn versus lung turnover between 1.5 and 6 lung turnovers. The index of acinar ventilation heterogeneity (Sacin) is then determined as the Sn value of the first breath minus the conductive ventilation contribution to the Sn increase of the first breath. In smokers and COPD patients, considerable increases in both Sacin and Scond have been observed [133, 134], with very limited reversibility of either Sacin or Scond in COPD patients [134, 135]. In smokers without COPD a sustained reversibility on Scond could be obtained with smoking cessation [136].
The most important advantage of the MBW indices Scond and Sacin is their sensitivity to the distal airways and their link to distinct anatomical locations. However, one important limitation should be borne in mind, and this applies to many other emerging “distal airways indices”: if changes occur in the distal airways, these indices will change, yet, the reverse may not necessarily be true. For instance, the standard single breath phase III slope is potentially sensitive to structural changes in the distal airways, yet it is impossible to infer from an increased phase III slope whether distal airways are uniquely responsible for it. The same holds for Scond which, from a theoretical point of view, can be generated at the very first branching generation of the conductive airway tree, and is potentially sensitive to the small conductive airways but also to its larger counterparts. It is by combining the various distal airway tests with overlapping information content that it is possible to gain confidence that Scond seen in COPD, at least partly, stem from the small conductive airways. This limitation does not apply to Sacin, since it offers a more unambiguous reflection of the distal airways, namely those in the acinar lung zone. Indeed, a Sacin increase necessarily implies that acinar structure has somehow been modified, as is observed in the case of COPD patients with emphysema [133]. A secondary advantage of the MBW test in the particular case of COPD with emphysema relates to the fact that in these patients, ventilation heterogeneity is also responsible for the underestimation of carbon monoxide diffusion capacity measurement [137], an effect that can be quantified and corrected.
Besides also offering FRC computation of the ventilated airspaces, the MBW test can be used to estimate the volume of trapped gas above the tidal volume range by including five oxygen inspirations to TLC at the end of a MBW test [138]. This measure of trapped gas in the tidal volume range could be useful in smokers or COPD patients, since the early data about the relationship of the single breath washout test with histomorphometry [9] did indicate that small conducting airway closure was one of the functional hallmarks of the disease.
An important limitation of the MBW analysis is that if conductive ventilation is so heterogeneous that one part of the lung is entirely washed out well within the first six lung turnovers, and in effect no longer participates in the mixing process, the analysis can no longer provide reliable estimates of Scond and Sacin. In that case both conductive and acinar ventilation heterogeneity produce a horizontal Sn asymptote and it is no longer possible to distinguish between both. Even then, the Sn value after, for example, six lung turnovers can still be used as a measure of overall lung ventilation heterogeneity, very similar to the information that is contained in the so-called lung clearance index that is regaining popularity for studies in cystic fibrosis patients [139]. Finally, an advantage of the MBW is that the measurements are performed in a near-physiological breathing range in terms of volume and flow. While being relatively easy for a patient to perform with respect to the functional information that can be gained, the limited availability of nitrogen measurement and analysis currently impairs its widespread use.
In conclusion, accurate assessment of distal airways function can be obtained using noninvasive techniques, but these techniques are not widely available. To date, measurement of lung hyperinflation is the most useful variable for indirect assessment of distal airways function in multicenter studies. MBW may well be the most sensitive and specific technique, but is limited to a few experienced centres. Forced oscillation technique is rather simple and has the potential to provide specific data on distal airways function, but further studies will be necessary to validate its usefulness.
IMAGING OF DISTAL AIRWAYS IN COPD
Imaging techniques such as CT, magnetic resonance imaging (MRI), scintigraphy and position emission tomography have been used to assess distal airways involvement in COPD subjects. Their major benefit is to provide a regional analysis of the lung as opposed to the global assessment obtained by pulmonary function tests. CT has been by far the most commonly evaluated and MRI is probably the most promising.
Computed tomography
At present, CT is the reference technique for the anatomical diagnosis of emphysema and is able to distinguish between various subtypes, namely centrilobular (fig. 2a and b), panlobular and subpleural [140]. Assessment of wall thickening of large- and medium-size airways, which are increased in smokers, can be obtained simultaneously [141]. Investigators have proposed that both emphysema and airway changes can be used to characterise clinically relevant phenotypes in COPD subjects [142]. Although visual subjective grading has yielded good correlation between CT and pathological measures of the extent of emphysema, objective CT densitometric analysis have been demonstrated to be more accurate and suitable for follow-up [143]. Since distal airspace destruction is characterised on CT by low-attenuation coefficients, analysis of the distribution of attenuation coefficients allows quantifying pulmonary emphysema. Due to isometric submillimetric acquisition obtained using multidetector-CT technology, quantification of emphysema using attenuation curves is achievable on any CT scan and fully automatic quantification measurement is easy to perform using commercially available software. Quantitative CT assessment of emphysema has been validated by CT-pathological correlations [144] and there are two types of methods for quantification: 1) the density mask technique which is defined as the percentage of the total lung volume that contains voxels with attenuation values below a predefined threshold (usually 950 Hounsfield Units (HU)), and 2) the percentile method is defined as the value (HU) at which a predefined percentage (5%, 10% or 15%) of the voxels have a lower attenuation value [140]. Considering COPD, it has been shown that measurement of attenuation values at inspiration was able to separate patients with GOLD stages I and II whereas the most severe GOLD stages III and IV were better differentiated by measurement of attenuation values at expiration [145].
{kind=link}
{kind=link}
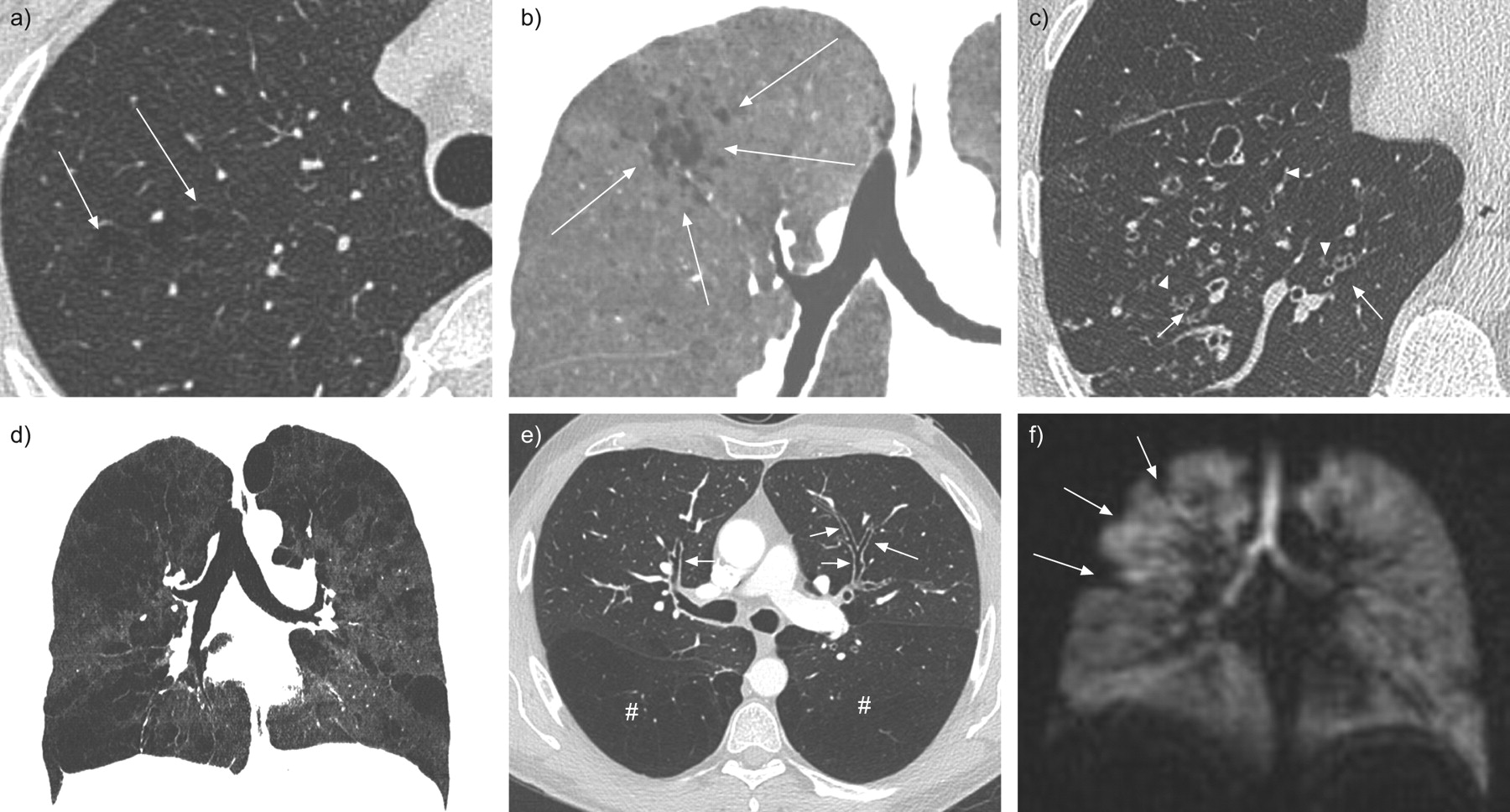
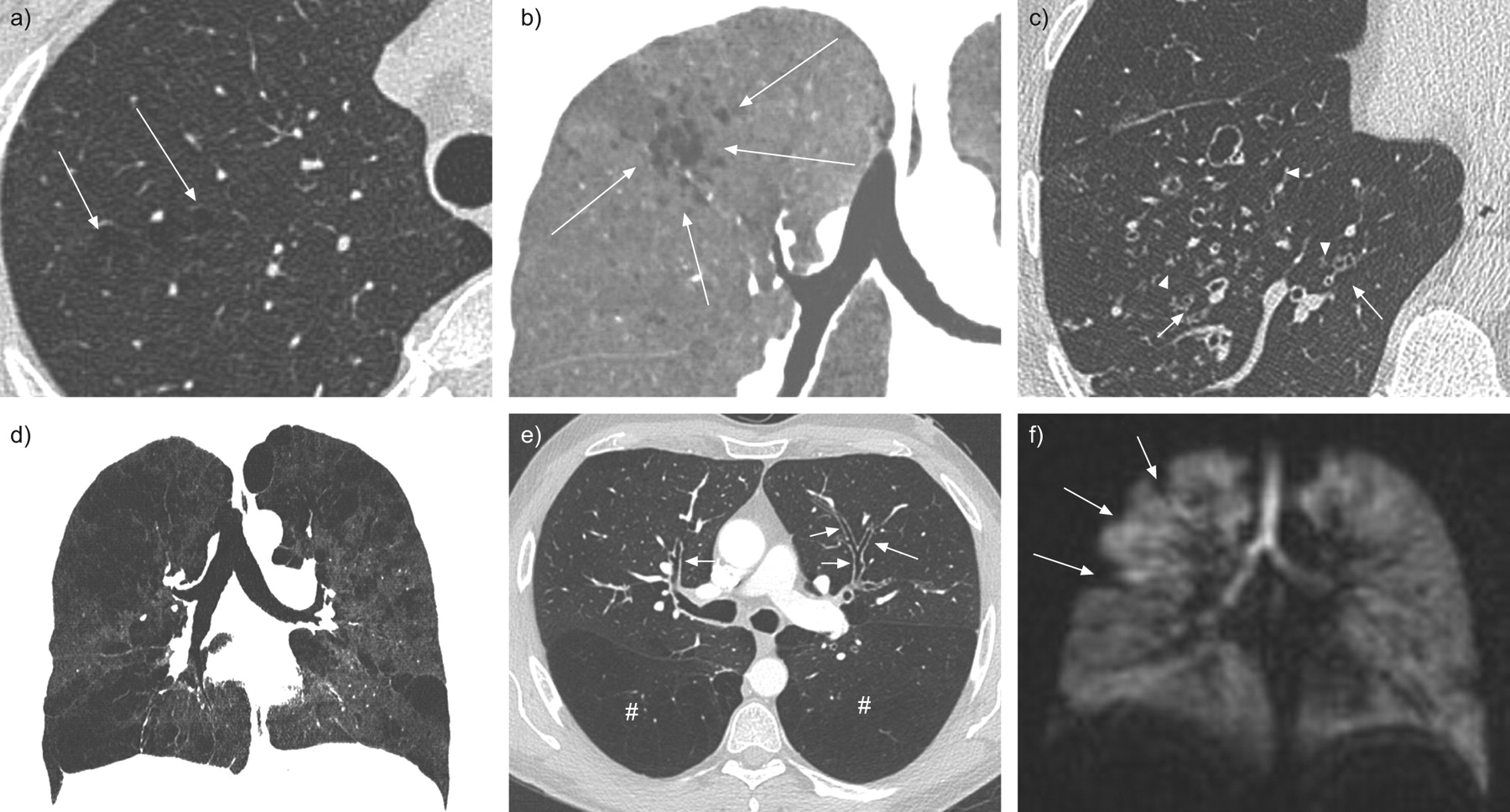
Representative computed tomography (CT) and magnetic resonance imaging (MRI) images showing small airways abnormalities. a) Axial CT image in a 45-yr-old smoker showing areas of low attenuation (arrows) related to early centrilobular emphysema. b) Coronal minimum intensity projection (minIP) image (5 mm thick) in the same subject showing the same lesions with a better conspicuity (arrows). c) Axial CT image in a 56-yr-old smoker with Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage III chronic obstructive pulmonary disease (COPD). Small airways findings are seen as multiple small micronodules, with some of them showing a typical branched (tree-in-bud) pattern (arrows). Dilated bronchiolectases (arrowheads) are present in the right lower lobe. d) Coronal minIP inspiratory image (5 mm thickness) of a 63-yr-old smoker with GOLD stage III COPD showing multiple areas of hypoattenuation of various size throughout the lung consistent with a mosaic pattern. There is no visual mean for separating emphysema from hypoattenuation areas related to small airways involvement. e) Axial CT image of a 52-yr-old smoker with GOLD stage II COPD showing areas of hypoattenuation in both the upper segments of the lower lobes (#) and thickened large airways (arrows). f) Coronal MRI images after inhalation of hyperpolarised 3He in a 42-yr-old COPD subject showing the heterogeneous distribution of gas within airspaces. Peripheral areas of hypointensity (arrows) are probably related to emphysema or areas of obstructed small airways. (MRI images provided by Y. Cremilleux, Universitie de Lyon, Lyon, France; personal communication).
Small airway disease can be detected on CT by the presence of few centrilobular nodules or/and branching lines, reflecting either reversible or irreversible pathological changes in small conducting airways (fig. 2c). In addition, these pathological changes, when below the spatial resolution of CT, may induce decreased lung attenuation called mosaic pattern on inspiratory CT images and air trapping on expiratory images. Areas of hypoattenuation on expiratory CT scans are likely to reflect the presence of obstruction and fibrosis of small conducting airways, but may also be the result of the loss of alveolar attachment to the airways, directly related to emphysema (fig. 2d). Therefore, differentiating air space enlargement (emphysema) and air trapping is not reliably achievable on CT images when assessed visually. Nevertheless, it has been suggested that evaluation of air trapping can be obtained by discarding voxels < -950 HU, considered as representing emphysema, and by calculating the relative volume changes of voxels of values between -950 HU and -860 HU between inspiration and expiration, which is thought to represent air trapping. Changes of volume in this subgroup of voxels have been shown to correlate closely with airway dysfunction in COPD regardless of the degree of emphysema [146].
Since airway wall thickening in large and medium airways has been demonstrated to reflect histological small airway changes in COPD [147], it is not surprising that objective quantitative measurements of large and intermediate airways in smokers reflect functional obstruction. The use of dedicated software on CT images enable authors to show that airway wall thickening occurred downward starting at the fourth generation of bronchi [148].
Several clinical studies have included CT measurements of emphysema and/or conducting airways abnormalities for defining COPD phenotypes (fig. 2e). Quantification and description of the site of emphysema may help in the diagnosis of disease severity and therapeutic management [149].
Limitations of CT scans include its relatively high cost and radiation exposure which may increase the incidence of cancer in young adults. Nevertheless, it is possible to reduce radiation exposure by performing low-dose CT scans, which are reliable for quantitative analysis [150]. Another limitation that may be important in multicenter studies is that technical aspects of scanners (manufacturers, X-ray tubes, etc.) may affect data and a lack of consensus related to the technical aspects of CT for quantitative CT analysis of lung and bronchi remains.
MRI
Proton (1H) MRI has long been considered challenging to use for the analysis of lung parenchyma because alveolar air contains low proton density. Furthermore, the multitude of air–tissue interfaces within the lung creates significant magnetic field distortions [140]. In COPD subjects, these limitations were even more problematic because of the reduction in lung tissue, hyperinflation and hypoxic vasoconstriction. However, recent progress in MRI technology has revealed new promises for this harmless technology which requires no radiation exposure. Indeed, assessment and localisation of lung hyperinflation are easily achievable and analysis of lung biomechanics can be obtained using dynamic data of thoracic wall and diaphragmatic motion.
Contrast-enhanced MRI using gadolinium contrast media with quantification of perfusion parameters has been shown to correlate with worsening of airflow limitation on pulmonary function test and emphysema index on CT. Regional heterogeneity of emphysema on CT matched with the decreased perfusion on MRI [151]. Although MRI spatial resolution is less than spatial resolution of CT, temporal resolution is excellent and MRI can be repeated several times without increasing radiation exposure.
Studies of ventilation parameters using MRI require an inhaled contrast agent and a multinuclei MRI. Polarised 3He is most interesting for airway imaging due to its physical properties and absence of diffusion. Images of ventilation heterogeneity at rest can be obtained in COPD subjects [152] (fig. 2f), whereas a single inhalation of 3He results in a homogeneous signal in normal subjects. Dynamic images can also be obtained during breathing and this allows the separation of emphysema from air trapping. The main limitations of 3He are its availability and cost, which preclude its large scale use. However, the recent PHIL study has indicated that the use of hyperpolarised 3He-MRI is possible and produced useful and reproducible data in a multicenter study [153]. Oxygen-enhanced MRI is easier to perform than 3He-polarised MRI. However, signal increased by only 15% compared with 1H-MRI even with ventilation using 100% inspiratory oxygen fraction (Fi,O2) [154]. Furthermore, oxygen is diffused through alveoli and images can be considered a mix of ventilation and perfusion rather than only ventilation. The most recent and probably the most promising MRI method for functional analysis of the lung is the so-called Fourier-transform 1H method implemented on a clinical 1.5T whole-body MRI scanner. The acquisition is free breathing and is not dependent on intravenous or inhalative contrast agents. A Fourier analysis is used to calculate perfusion- and ventilation-weighted images based on intensity changes in corresponding lung areas with respect to the cardiac and respiratory frequencies. The described method has been applied in preliminary studies on volunteers and patients showing clinical relevance to obtain noncontrast-enhanced perfusion and ventilation data [155].
CLINICAL MANIFESTATIONS ASSOCIATED WITH DISTAL AIRWAY IMPAIRMENT
As discussed previously, small conducting airways contribute little to airflow resistance in normal subjects. Thus, abnormalities in these airways cause few changes in usual pulmonary function tests and limited clinical manifestations until most of the airways are obstructed. It is predicted that obstruction of 75% of all small conducting airways is required before significant airflow limitation can be detected by routine pulmonary function tests [9]. Because COPD is a slowly progressive disease, these findings may explain why early symptoms develop slowly and are often neglected by patients.
An interesting approach to examine the roles of distal airways in subjects with COPD is to focus on patients with airflow limitation (reduced FEV1/FVC) but normal FEV1 in whom airflow limitation is mostly related to changes in distal airways. Roche et al. [156] evaluated respiratory symptoms in a large population of subjects recruited in health prevention centres. These authors found significant dyspnoea (defined by an MRC dyspnoea grade ≥1) in ∼30% of subjects with airflow limitation and FEV1 between 80% and 100% pred [156]. Two recent physiological studies may help to explain this surprising finding. The first by Ofir et al. [107] examined ventilatory constraints during exercise in 21 symptomatic smokers with GOLD stage I COPD (FEV1/FVC 60±6% pred, post-bronchodilator FEV1 91±7% pred) compared with 21 healthy sex- and age-matched controls with normal spirometry. Subjects with GOLD stage I COPD had evidence of distal airways abnormalities characterised by a very low FEF25–75% (34±12% pred), a marked increase in specific Raw (290±97% pred) and increased CC/TLC ratio. All subjects were submitted to incremental cycle exercise and COPD subjects had significant reduction in peak oxygen consumption and power output; dyspnoea ratings were also higher for a given work rate and ventilation in COPD subjects [107]. Compared with normal subjects, COPD subjects had increased ventilatory demand, ascribed to greater ventilation/perfusion abnormalities, and increased EELV during exercise, corresponding to dynamic hyperinflation [107]. Dyspnoea intensity increased as a function of each of these independent variables, suggesting a role for distal airways in dyspnoea pathophysiology [107]. Secondly, O'Donnell et al. [157] studied the acute effects of ipratropium bromide (a short-acting anticholinergic) on exercise limitation in 16 subjects with GOLD stage I COPD with rather similar characteristics to those of Ofir et al. [107]. Following a cross-over design, subjects performed pulmonary function tests and cycle exercise at 80–85% of maximal work capacity 2 h after nebulised ipratropium bromide (0.5 mg) or placebo [157]. The authors reported that ipratropium bromide induced modest but consistent improvement in FEV1 (+5% pred, RV (-12% pred) and specific Raw (-81% pred) [157]. A fall in dyspnoea intensity was observed at higher submaximal ventilatory levels and correlated with the concurrent decrease in EELV [157]. Collectively these studies suggest that distal airways abnormalities could be responsible for exercise dyspnoea in subjects with mild COPD. However, it should be emphasised that COPD is a heterogeneous disease [158] and that these physiological studies were performed in small numbers of selected subjects and would need to be confirmed in larger studies.
Chronic cough and sputum production are present in many COPD patients even among GOLD I subjects [159]. Expectoration is considered a manifestation of mucus hypersecretion that may originate from both proximal and distal airways [160]. Limited data are available on the relationship between symptoms of cough and sputum production and morphological changes that characterise mucus hypersecretion. Saetta et al. [25] found increased numbers of goblet cells in the epithelium of small conducting airways in COPD subjects with chronic cough and sputum production compared with asymptomatic healthy nonsmokers. No significant difference in goblet cell numbers was found between these symptomatic COPD subjects and asymptomatic smokers. Caramori et al. [26] compared mucin expression in the small conducting airways in 20 smokers (COPD n = 9) and six nonsmokers with normal lung function. When the subjects were grouped according to the presence (n = 15) or absence (n = 11) of chronic bronchitis, no difference in mucin expression was found. Furthermore, studying patients with severe emphysema undergoing LVRS (n = 101), Hogg et al. [161] reported that chronic cough and sputum production were not associated with the presence of muco-inflammatory exudates in the lumens of small conducting airways. Collectively, these data suggest that mucus hypersecretion in small conducting airways is not associated with cough and sputum production. Further studies in less selected groups of COPD subjects may be necessary to confirm these findings.
Health-related quality of life (HRQoL) is an important outcome in COPD subjects. In the Wellington Respiratory Survey, Weatherall et al. [162] compared HRQoL (measured using the St George's Respiratory Questionnaire) and spirometry in >700 subjects selected from a population-based study. Airflow limitation (diagnosed by a post-bronchodilator FEV1/FVC <0.7) was associated with clinically significant changes in health status [162]. Importantly, HRQoL was significantly altered in COPD subjects with airflow limitation but FEV1 >80%, indicating that many subjects with predominant distal airway impairment have reduced HRQoL.
Association of distal airway impairment with mortality has been suggested by the results of large epidemiological studies involving GOLD I subjects. For example, mortality was increased in GOLD I subjects compared with subjects with normal lung function in the Copenhagen City Heart Study [163]. A more direct relationship between distal airways abnormalities and mortality is provided by data obtained by histomorphometric measurement of small conducting airways in GOLD III and IV COPD subjects (n = 101) undergoing surgery (LVRS) [161]. The authors grouped these subjects according to quartiles of luminal obstruction by mucus exudates (quartile 1: smallest luminal occlusion; quartile 4: greatest luminal occlusion) in small conducting airways [161]. Subjects in quartile 1 had a median survival of 48 months, whereas subjects in quartile 4 had a median survival of 92 months [161]. These differences persisted after adjustments for important covariates (FEV1, age, dyspnoea and HRQoL) [161].
THERAPIES TARGETING DISTAL AIRWAYS IN COPD
Strategies for targeting both proximal and distal airways in COPD subjects include the delivery of oral medications or inhaled medication using extrafine particles, which are known to deposit in both proximal and distal airways as opposed to non-extrafine particles that deposit predominantly in proximal airways.
Oral drugs
Few oral drugs are currently available for the treatment of COPD [6]. Although theophylline is recommended in the GOLD guidelines and has been advocated by some authors [164], its use is not current practice in most industrialised countries. Roflumilast is a novel phosphodiesterase 4 inhibitor that has been shown to induce a modest increase in FEV1 and to reduce COPD exacerbations in specific subgroups of COPD subjects [165, 166]. However, no data was found on the effects of roflumilast on distal airways. The BRONCUS (Bronchitis Randomized On N-acetyl cysteine Cost Utility Study) study examined the effects of treatment with N-acetyl cysteine (600 mg·day−1) versus placebo for 3 yrs [167]. The rate of decline in FEV1 and the rates of exacerbations were not different between groups [167]. Secondary analysis revealed that FRC was reduced (-0.374 l) in the N-acetyl cysteine group, a finding suggestive of an effect on hyperinflation [167]. In a randomised, double-blind, cross-over study that included 24 moderate-to-severe COPD subjects, Stav et al. [168] evaluated the effects of a 6-week treatment with N-acetyl cysteine (1,200 mg·day−1) versus placebo on lung hyperinflation at rest and after exercise. The authors reported that IC and FVC were higher especially after exercise following N-acetyl cysteine treatment; furthermore, RV/TLC was reduced and endurance time was longer after N-acetyl cysteine treatment. The authors suggested that N-acetyl cysteine treatment in subjects with COPD has a beneficial effect on physical performance, probably due to a reduction in air trapping. No clear explanation is available for these surprising findings.
Inhaled drugs
Inhaled drugs are the cornerstone of therapy for COPD subjects [92]. Current inhaled drugs include LABA, LAMA and inhaled steroids in combination with LABA. Sturton et al. [169] have tested in vitro the bronchodilatory effects of salbutamol and various LABA in human precision-cut lung slices of small conducting airways contracted with carbachol. These data confirmed that functional β2 receptors exist in small conducting airways. M3 muscarinic receptors, which are the targets of LAMA, are also present on smooth muscle in small conducting airways [170], and glucocorticoid receptors are expressed in distal airways [170]. Thus, all currently available inhaled drugs may have effects on distal airways if they can reach them.
Currently available inhaled drugs are marketed in non-extrafine formulations with particles of 3–5 mm mean median aerodynamic diameter which deposit predominantly in proximal airways. These inhaled drugs have beneficial effects on various clinical outcomes (e.g. dyspnoea, exacerbations and health status) in COPD subjects [4, 5], but little data is available on their effects on distal airways. In a small study involving 18 subjects, Tantucci et al. [171] reported that in COPD subjects in whom salbutamol had no effect on FEV1, salbutamol significantly increased IC and decreased FRC. Duranti et al. [172] confirmed that salbutamol increased IC and reduced FRC without significant changes in TLC in stable COPD subjects. Furthermore, the LABA salmeterol reduced airway resistance measured by impulse oscillometry in COPD subjects [125] and reduced hyperinflation during exercise [110]. Several studies have shown that tiotropium, a LAMA, reduced hyperinflation at rest [173] and during exercise [111].
For targeting distal airways, a strategy consists of inhaled medication using extrafine particle formulations, which deposit both in proximal and distal airways and, thus, may have greater effects on distal airways. Few randomised controlled clinical studies were performed using extrafine formulations of inhaled particle in COPD subjects. Corda et al. [174] evaluated the effects of extrafine hydrofluroalkane-beclomethasone (BDP) (800 μg·day−1; 16 weeks) versus placebo on lung function and exercise tolerance in COPD patients with α1-antitrypsin deficiency, when added to salmeterol and oxitropium bromide. Extrafine BDP resulted in a significant increase in FEV1, FVC, IC and distance covered, and dyspnoea perceived during a shuttle walk test [174]. The authors suggested that extrafine BDP decreased airway narrowing, mostly in the small airways, further reducing dynamic hyperinflation [174]. However, no comparison with non-extrafine inhaled steroids was available in this study.
Calverley et al. [175] have recently performed a double-blind, double-dummy, randomised, active controlled, parallel group, 48-week study involving over 700 COPD subjects (mean FEV1 1.14l; 42% pred). The authors compared the effects of an inhaled extrafine pressurised metered-dose inhaler formulation of BDP/formoterol 400/24 μg·day−1 versus budesonide/formoterol dry powder inhaler (DPI) 800/24 μg·day−1 (noninferiority) and versus formoterol DPI 24 μg·day−1 (superiority) [175]. The co-primary end-points were changes from baseline to 48 weeks in pre-dose morning FEV1 and mean rate of COPD exacerbations. In terms of FEV1 improvement, BDP/formoterol was shown to be comparable to budesonide/formoterol and superior to formoterol (0.077l versus 0.080l versus 0.026l; from baseline respectively) [175]. The authors reported no differences among groups for exacerbations, which occurred at an unexpected low rate in this study probably due to restrictive inclusion criteria [175]. Only subjects treated with extrafine BDP/formoterol had significant improvement in pre-dose FVC (+90 mL versus baseline; p<0.005), whereas no significant improvement was observed with budesonide/formoterol DPI (+50 mL versus baseline; p = 0.152) or with formoterol DPI (+20 mL versus baseline; p = 0.582) [175]. The greater improvement in FVC obtained with extrafine BDP/formoterol is consistent with a more efficient distal deposition, because FVC correlated strongly with RV/TLC and has been proposed as a surrogate marker of hyperinflation [97]. At the end of the study the change in the distance covered in the 6MWT was highest, although not statistically significant, in the patients receiving extrafine BDP/formoterol followed by budesonide/formoterol and then formoterol alone. On average, the improvement with extrafine BDP/formoterol was above the threshold of 37 m [175], which has been recently described as clinically relevant [176]. The tolerance of extrafine BDP/formoterol was comparable to comparators. Further studies will be necessary to understand all aspects of effects associated with extrafine BDP/formoterol in COPD subjects.
CONCLUSION
We found compelling evidence that distal airways are the major site of airflow limitation in COPD subjects. Structural abnormalities and inflammatory changes in distal airways increase with more severe bronchial obstruction. Distal airways abnormalities are associated with dyspnoea and reduced health status even in GOLD I subjects, where damage to distal airways is believed to be predominant. Mucus plugging in small conducting airways is an important determinant of mortality in GOLD III and IV subjects. These findings provide a strong rational for clinical trials using inhaled therapies with extrafine particles that will, unlike usual (larger) inhaled particles, deposit in both proximal and distal airways. Distal airways abnormalities are found early in the course of COPD and this provides a rational for early therapy targeting these airways. Such studies will have to include clinical end-points (e.g. exacerbations) and should include assessments of distal airways using physiological tests (e.g. forced oscillation) and/or imaging techniques (e.g. CT scan and/or MRI).
Acknowledgments
Author affiliations are as follows. P-R. Burgel and D. Dusser: Hôpital Cochin, AP-HP, Université Paris Descartes, Paris, France; A. Bourdin: Hôpital Arnaud de Villeneuve, CHU Montpellier, Montpellier, France; P. Chanez: Hôpital Ste-Marguerite, AP-HM, INSERM UMR 6020, Université de la Méditerranée, Marseille France; F. Chabot and A. Chaouat: Hôpital de Brabois, CHU de Nancy, Nancy, France; T. Chinet: Hôpital Ambroise Paré, AP-HP, Boulogne, France; J. de Blic: Hôpital Necker-Enfants Malades, AP-HP, Université Paris Descartes, Paris, France; P. Devillier: Hôpital Foch, UPRES EA 220, Université Versailles Saint-Quentin, Suresnes, France; A. Deschildre: Unité de pneumologie pédiatrique, Hôpital Jeanne de Flandres, CHRU Lille, Lille, France; A. Didier: Hôpital Larrey, Université de Toulouse, Toulouse, France; G. Garcia: Hôpital Antoine Béclère, AP-HP, Clamart, France; G. Jebrak: Hôpital Bichat, APHP, Paris, France; F. Laurent: CHU de Bordeaux, Université Victor Segalen Bordeaux 2 INSERM U855, Bordeaux, France; H. Morel: CH Broussais, Saint-Malo, France; T. Perez and I. Tillie-Leblond: CHRU de Lille, Hôpital Albert Calmette, Lille, France; C. Pilette: Cliniques Universitaires St-Luc et Institut de Recherche Expérimentale et Clinique, Université catholique de Louvain (UCL), Brussels, Belgium; N. Roche: Hôpital de l'Hôtel-Dieu, AP-HP; Université Paris Descartes, Paris, France; S. Verbanck: University Hospital, Vrije Universiteit Brussel, Brussels, Belgium.
Footnotes
Provenance
Publication of this peer-reviewed article was supported by Chiesi SA, France (article sponsor, European Respiratory Review issue 119).
Statement of Interest
D. Dusser received fees for consultancy, advisory board participation or lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis and Nycomed. Industry-sponsored grants for education were received from GlaxoSmithKline and Boerhinger-Ingelheim. The present article is the result of a workshop organised with the support of Chiesi for which honorarium were received as speaker. P-R. Burgel received fees for advisory board participation or lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis and Nycomed. The present article is the result of a workshop organised with the support of Chiesi for which honorarium were received as speaker. A. Bourdin received a €1,500 fee for speaking from Chiesi during a workshop in 2009 and 2010. P. Chanez has provided consultancy services for Almirall, BI, Centocor, GlaxoSmithKline, MSD, AstraZeneca and Novartis, Teva, Chiesi, and Schering Plough. He has served on advisory boards for Almirall, BI, Centocor, GSK, AstraZeneca, Novartis, Teva, Chiesi, Schering Plough and MSD. He has received lecture fees from Almirall, BI, Centocor, GSK, AstraZeneca, Novartis, Teva, Chiesi, Schering Plough and MSD. He has received industry-sponsored grants from Almirall, BI, Centocor, GSK, AstraZeneca, Novartis, Teva, Chiesi and Schering Plough. F. Chabot has received fees for speaking from Chiesi. Travel to the ERS and SPLF Congresses were funded by Altana, Boehringer Ingelheim, Chiesi and GSK. T. Chinet has received reimbursements for attending meetings and symposia and/or fees for speaking from Chiesi, Pfizer, Boehringer Ingelheim, Novartis, AstraZeneca and GSK. J. de Blic has received consulting fees from Merck, GSK, Chiesi, Stallergenes and ALK; lecture fees from Merck, Chiesi, GSK, Stallergènes and ALK; and has received grant support from GSK. Travel to the ERS and ATS Congresses were funded by GSK and Chiesi. P. Devillier has received fees for speaking or for participating in research boards from Almirall, AstraZeneca, Bioprojet Pharma, Boehringer Ingelheim, Chiesi, GSK, Merck Sharp and Dohme, Nycomed, Sanofi-Aventis, Schering-Plough and Stallergènes. He has received grants for research in fundamental pharmacology from Boehringer Ingelheim, Pierre Fabre, Novartis, Nycomed and Servier. A. Deschildre has relationships with drug companies including GSK, MSD and Novartis, relationships include consultancy and membership of scientific advisory boards. Travel to the ERS and ATS Congresses was funded by GSK. A. Didier has a consulting arrangement with GSK, Stallergenes, ALK, Novartis, MSD and Chiesi, and has received honoraria from AstraZeneca and Schering-Plough. G. Jebrak has received a fee for speaking during a meeting about the subject prior to publication. F. Laurent has received fees for speaking and reimbursement for attending a symposium from Chiesi. H. Morel has received reimbursement for attending a symposium from Boehringer Ingelheim, Chiesi and Novartis. T. Perez was a paid speaker for GSK, AstraZeneca, Novartis, Boehringer Ingelheim and Chiesi, and a consultant for Novartis, Nycomed, Chiesi. He also received funding for clinical research by Boehringer Ingelheim. C. Pilette's travel and accommodation to the “Small airways in COPD” meeting in Vence (France) was funded by Chiesi. I. Tillie-Leblond has received reimbursement for attending a symposium, fees for speaking, funds for research and fees for consultancy from AstraZeneca, GSK, Chiesi, Novartis and Boehringer Ingelheim. N. Roche has received fees for speaking, organising education or consulting from Altana Pharma, Nycomed, AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, MEDA, Mundipharma, Novartis, Pfizer and Teva.
- Received December 2, 2010.
- Accepted December 19, 2010.
- ©ERS 2011
REFERENCES










Jump To
- Article
- Abstract
- INVESTIGATING STRUCTURAL ABNORMALITIES AND INFLAMMATION IN DISTAL AIRWAYS
- DISTAL AIRWAYS INFLAMMATION IN COPD
- PULMONARY FUNCTION TESTS
- IMAGING OF DISTAL AIRWAYS IN COPD
- CLINICAL MANIFESTATIONS ASSOCIATED WITH DISTAL AIRWAY IMPAIRMENT
- THERAPIES TARGETING DISTAL AIRWAYS IN COPD
- CONCLUSION
- Acknowledgments
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics