





Abstract
Thoracoscopy is an old but still very valuable technique for the evaluation of pleural pathology and, especially for the further investigation of the aetiology of pleural fluid. It remains of great importance, since it is able to not only provide an exact diagnosis, but also can have therapeutic potential. In this review, the differential diagnostic aspects of transudate versus exudate are further elaborated, and the role of thoracoscopy is compared to closed pleural biopsy and image guided biopsy.
Thoracoscopy is not new; this year we will celebrate the Centennial of Thoracoscopy, as the first thoracoscopic procedure was performed by the Swedish internist H.C. Jacobaeus in 1910. Today, thoracoscopy is still a valuable tool in the diagnosis and treatment of pleural diseases. In this review, we will discuss the diagnostic and therapeutic aspects of thoracoscopy in patients with pleural effusion. Thoracoscopy has a place in the diagnosis and treatment of other diseases, such as pneumothorax, palmary hyperhidrosis and empyema. These diseases will not be discussed here.
DIAGNOSTIC ASPECTS OF THORACOSCOPY
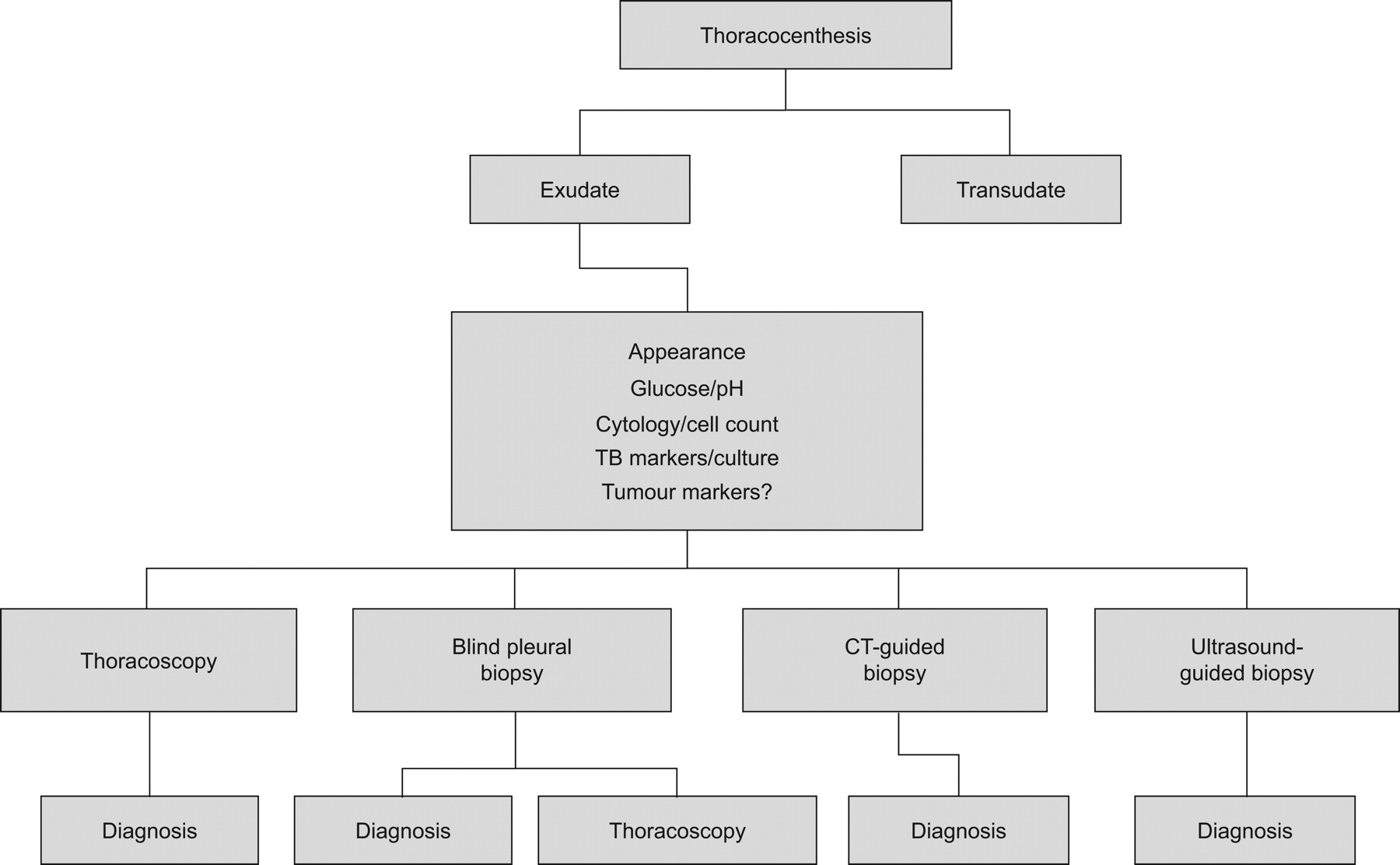
The flow chart of the work-up of pleural effusion is presented in figure 1. Thoracocenthesis is the first procedure to be performed in a pleural effusion of >1 cm diameter in lateral decubitus position [1]. The most important step in narrowing the differential diagnosis is to distinguish a transudate from an exudate. To do this, Light's original citeria (ratio of pleural fluid/serum protein >0.5, ratio of pleural fluid/serum lactate dehydrogenase (LDH) >0.6 or pleural fluid LDH more than two-thirds of the upper limit of normal serum value) are still appropriate [1].

{kind=link}
The diagnostic work-up of pleural effusion. CT: computed tomography.
If the protein level is >35 g·L−1, the effusion is most likely an exudate [2]. In borderline exudates (protein level >25 but <35 g·L−1) Light's criteria may misclassify transudates in up to 20% of cases, especially in patients with congestive heart failure who have been on diuretics. To discriminate true transudates from pseudo-exudates, measurement of the pleural protein gradient or the pleural fluid albumin gradient can be applied: if serum protein level minus pleural protein level is >3.1 g·dL−1, or serum albumin level minus pleural albumin level is >1.2 g·dL−1, it is a transudate [1]. In recent studies, measurement of pro-B-type natriuretic peptide (pro-BNP) in pleural fluid and serum appeared to be promising in the diagnosis of transudates in patients with chronic heart failure. In case of possible misclassification by the use of Light's criteria, measurement of pro-BNP level may appear to be a better tool to differentiate a transudate from a pseudo-exudate [3–6].
In the case of an exudate, and benign or non-conclusive cytology, infection, pulmonary embolism and abdominal disease should be considered. If these diseases have been ruled out or are very unlikely, the exudate is caused by malignant disease, tuberculosis or the exudate is idiopathic.
In the past, it has been stated that a malignant pleural effusion can also occur as a transudate [7]. This is most likely due to imperfect application of the diagnostic rules, or comorbid conditions like hypoalbuminaemia, cirrhosis with ascites or chronic heart failure.
ANALYSIS OF AN EXUDATE
In the case of a proven exudate with non-conclusive cytology after (repeated) thoracocenthesis, an additional procedure to obtain pleural histology tissue is the next step. This can be done with a minimal invasive procedure in four ways: closed pleural biopsy (CPB; Abrams biopsy), thoracoscopy, ultrasound (US)-guided biopsy, and computed tomography (CT)-guided biopsy. A comparison of these techniques is summarised in table 1.
CPB (ABRAMS BIOPSY)
CPB is an old technique. In patients with pleural effusion, a blind biopsy of the parietal pleura can be obtained. In malignant pleural disease, the additional diagnostic yield of CPB after thoracocenthesis is limited to 7% [8].
The diagnostic yield of CPB is better in areas with high incidence of tuberculosis (TB), as has been demonstrated by Diacon et al. [9]. In their study, the diagnostic yield of the combination of TB culture and histology reached 79%, with a sensitivity of 93%, if combined with serum adenosine deaminase level and lymphocytosis of the pleural fluid (lymphocytes/neutrophils >0.75). In a prospective study in the UK, Maskell et al. [10] compared CPB with CT-guided pleural biopsy. The results for the CT group were: sensitivity 87%, specificity 100% and negative predictive value 80%. In the CPB group the results were: sensitivity 47%, specificity 100% and negative predictive value 44%.
In conclusion, CPB should no longer be used in a setting where image-guided pleural biopsies can be obtained. Use of CPB is only indicated in areas with high incidence of TB and limited medical resources [9].
CT- VERSUS US-GUIDED PLEURAL BIOPSY
There are no comparative studies of the diagnostic yield of CT- and US-guided biopsy; the diagnostic sensitivity of both techniques is high (>83%) [11]. The characteristics of each procedure are summarised in table 1.
THORACOSCOPY VERSUS IMAGE-GUIDED PROCEDURES
The diagnostic yield of thoracoscopy is high; it is reported to be >90% in the majority of studies (table 2). Although it is a more invasive procedure compared with image-guided pleural biopsy, the big advantage of thoracoscopy is the possibility to perform a therapeutic intervention in the same session as the diagnostic biopsy of the pleura.
The possible therapeutic procedures during thoracoscopy are: 1) removal of (septated) pleural effusions; 2) talc poudrage (under visual control if preferred); and 3) drain positioning under visual control.
Thoracoscopy is the preferred procedure if no clear target lesion is visible on the CT scan, and in patients with large or recurrent effusions, in whom drainage and pleurodesis is indicated. Image-guided pleural biopsy may be the procedure of choice in elderly, unfit patients with small pleural effusions. The diagnostic work-up of a pleural effusion is summarised in figure 1.
HOW TO DEAL WITH UNDIAGNOSED PLEURAL EFFUSION
After a complete work-up of pleural effusion including thoracoscopy, a specific diagnosis may not be available in a considerable amount of cases (table 2).
This condition is described as “idiopathic pleuritis”, “unspecific pleuritis”, “nonspecific pleuritis” or “pleuritis with indeterminate cause”. This specific problem has been retrospectively addressed by four studies, three of which included thoracoscopy in the work-up, and one thoracotomy [19, 22–24]. The results of these studies are summarised in table 3.
In our study of 208 patients with a nonspecific pleuritis after thoracoscopy, 85% followed a benign course during follow-up [23]. A “wait and see” approach is therefore justified in the majority of these patients. An extended video-assisted thoracoscopic surgery procedure is indicated in case of a difficult thoracoscopy with adhesions and layers of fibrin, especially if there is a clinical suspicion of mesothelioma. Otherwise, the patients should be monitored with regular chest radiography. In case of a persistent or increasing pleural effusion, thoracocenthesis should be repeated. If the analysis of the pleural fluid is showing a lymphocytosis or increased LDH, the thoracoscopy should be repeated [23].
CONCLUSIONS
Thoracoscopy is an old, safe and simple procedure. Any pulmonologist who deals with pleural disease nowadays should be able to perform thoracoscopy. The diagnostic yield of pleural effusions under CT or US guidance is only slightly inferior to thoracoscopy (85% versus >90%). Thoracoscopy is the preferred procedure if no clear target lesion is visible on the CT scan. Also, thoracoscopy is preferred if removal of pleural effusion and/or pleurodesis is indicated, because during thoracoscopy the diagnostic and therapeutic procedure can be performed in the same session.
Footnotes
Provenance
Publication of this peer-reviewed article was supported by GlaxoSmithKline, Belgium (principal sponsor, European Respiratory Review issue 117).
Statement of Interest
None declared.
- Received May 25, 2010.
- Accepted May 26, 2010.
- ©ERS 2010
References









