





Abstract
Paradoxical reaction (PR) in tuberculosis (TB) is common and may affect up to 25% of patients. PR has the potential to cause significant morbidity and, on occasion, death. Although PR has been recognised for some time, the pathophysiology, especially in HIV-negative patients, is not well understood.
We present two cases of PR in HIV-negative patients with TB presenting as significant airway obstruction secondary to a florid endobronchial component.
These cases demonstrate that PR should be considered in all patients presenting with airway symptoms who have started TB treatment. The outcomes of the cases illustrate the need for wider recognition of this condition and more research to characterise patients who may be at risk, in order to gain a greater understanding of the mechanisms involved and to make or predict this diagnosis earlier.
Paradoxical reaction (PR) in tuberculosis (TB) is defined by a clinical or radiological worsening of pre-existing tuberculous lesions or the development of new lesions, in patients receiving anti-tuberculous medication who initially improved on treatment. This syndrome has been recognised for some time and, although it is often self-limiting, its potential to cause serious morbidity and, on occasion, death, is increasingly being recognised. Although the exact mechanisms are not understood it is most likely that PR is due to an abnormal immune response or reconstitution of the immune system. For this reason PR is more commonly seen in HIV co-infected individuals [1]. We describe two cases of severe PR in HIV-negative patients, both presenting with a florid endobronchial element.
PR is a diagnosis of exclusion, and poor compliance, drug resistance, progression of original disease and secondary diagnoses should be ruled out. The incidence, timing and clinical spectrum of PR varies widely between previous studies and the phenotype and risk factors associated with this syndrome are not well understood. In HIV-negative patients with pulmonary TB in Taiwan, the incidence of PR was 2.4% [2]. However, in a different group of HIV-negative patients with lymph node TB, the incidence was 23% [3]. This difference may be a result of many factors including the site of disease and the patient population. The most common manifestations are worsening of the original lesions (75%), especially in central nervous system (CNS) disease. When new lesions are seen these are again commonly CNS lesions, followed by new pleural disease (including effusions) and then skin and lymph node lesions [4]. We believe that both our cases are secondary to a PR on the basis of the exclusion of other diagnoses, adequate adherence to therapy and the observed marked responses to corticosteroids.
CASE 1
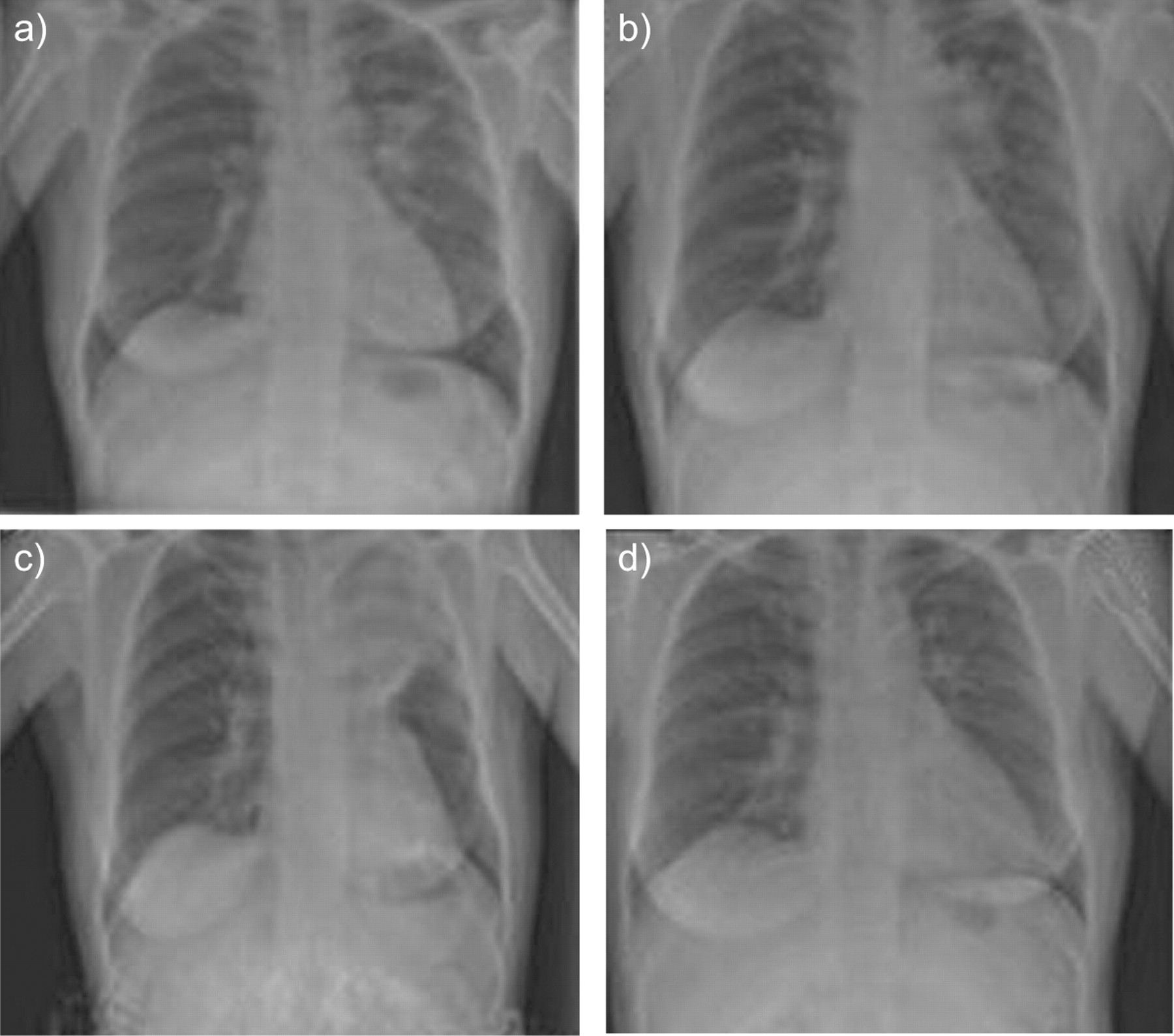
A 48-yr-old Bangladeshi female initially presented to the Ear, Nose and Throat clinic (St Mary’s Hospital, London, UK) with left-sided cervical lymphadenopathy. She also complained of a chronic dry cough, but no other systemic or pulmonary symptoms. Following a chest radiograph she was referred to the chest clinic. The radiograph showed left peri-hilar shadowing (fig. 1⇓), but examination of the chest was normal and she was not producing any sputum. She had a 21-mm reaction to 2 tuberculin units of RT23 intradermally. She went on to have a bronchoscopy and macroscopically the endobronchial tree was normal; however, fully sensitive TB was cultured from the lavage fluid. HIV serology was negative.

Results of a chest radiograph performed in case 1 from a) July 2006, b) October 2006, c) November 2006 and d) January 2007.
She was started on standard quadruple therapy and the cervical lymphadenopathy improved. She complied well with medication and there were no complications. As a result, she was stepped down to dual therapy 2 months later.
However, 4 months after starting treatment she attended the clinic feeling increasingly unwell and with mild shortness of breath. A chest radiograph was performed which showed worsening of the hilar lesions (fig. 1b⇑). A computed tomography (CT) scan was organised (fig. 2⇓), which showed left upper lobe peribronchial lymphadenopathy. When she re-attended the clinic she was complaining of wheeze. A plain chest film showed collapse of the left upper lobe (fig. 1c⇑).

A computed tomography scan performed in case 1 showing left upper lobe peribronchial lymphadenopathy.
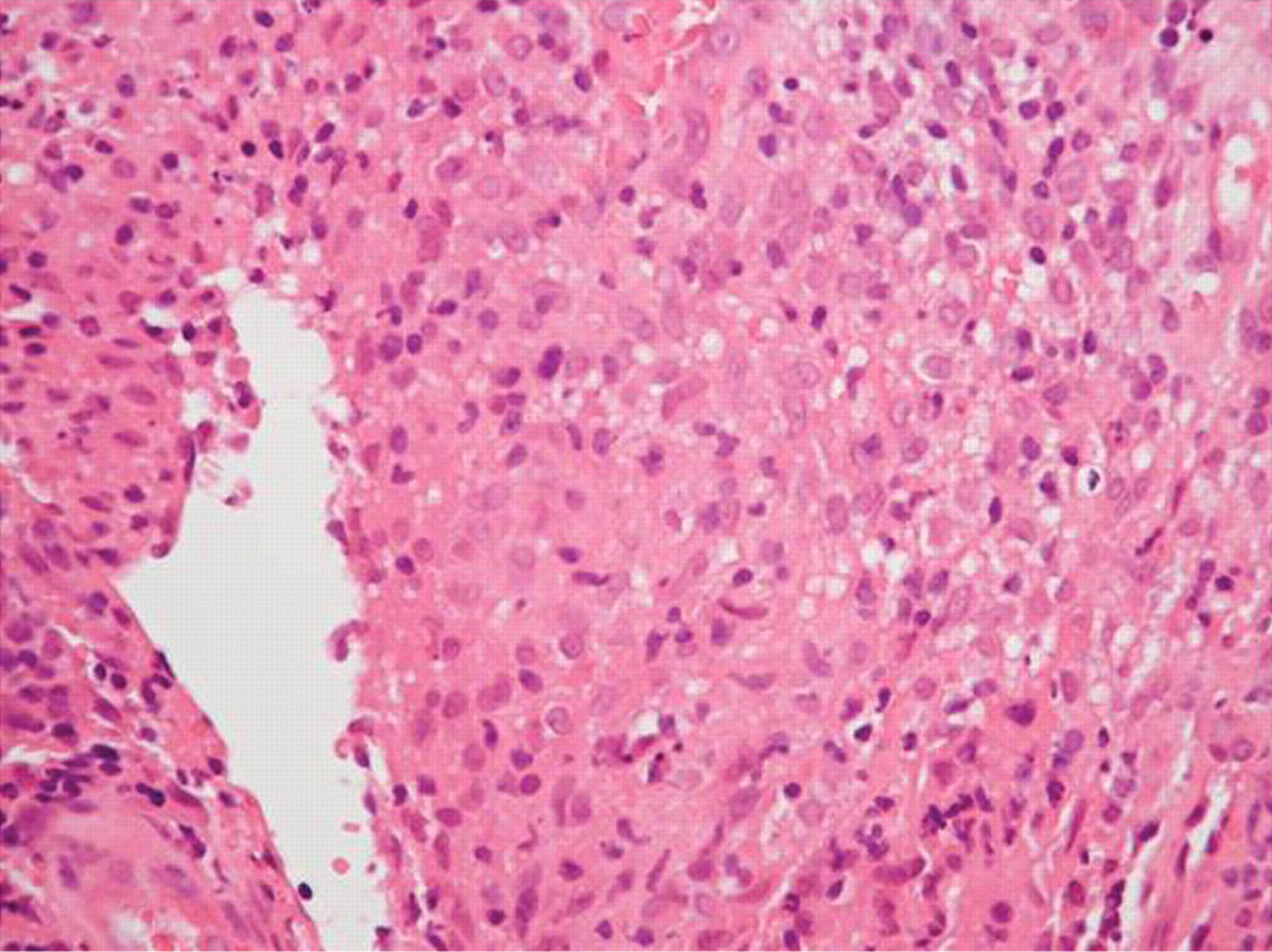
At this stage her compliance was readdressed but confirmed as good and she proceeded to a further bronchoscopy. At this time, a number of small nodular lesions were seen endobronchially throughout the bronchial tree, and the left upper lobe main bronchus was completely occluded (fig. 3⇓). Histology of these lesions revealed bronchial mucosa with loose inflammatory tissue and marked chronic inflammation with sheets of histiocytes. Small vague granulomas were seen but staining was negative for alkali and acid-fast bacteria and fungi (fig. 4⇓). The final culture was negative for TB and other infections.

a) Nodular lesion in the right main bronchus adjacent to the main carina. b) Left upper lobe bronchus obstructed by lesion, but patent when washed.
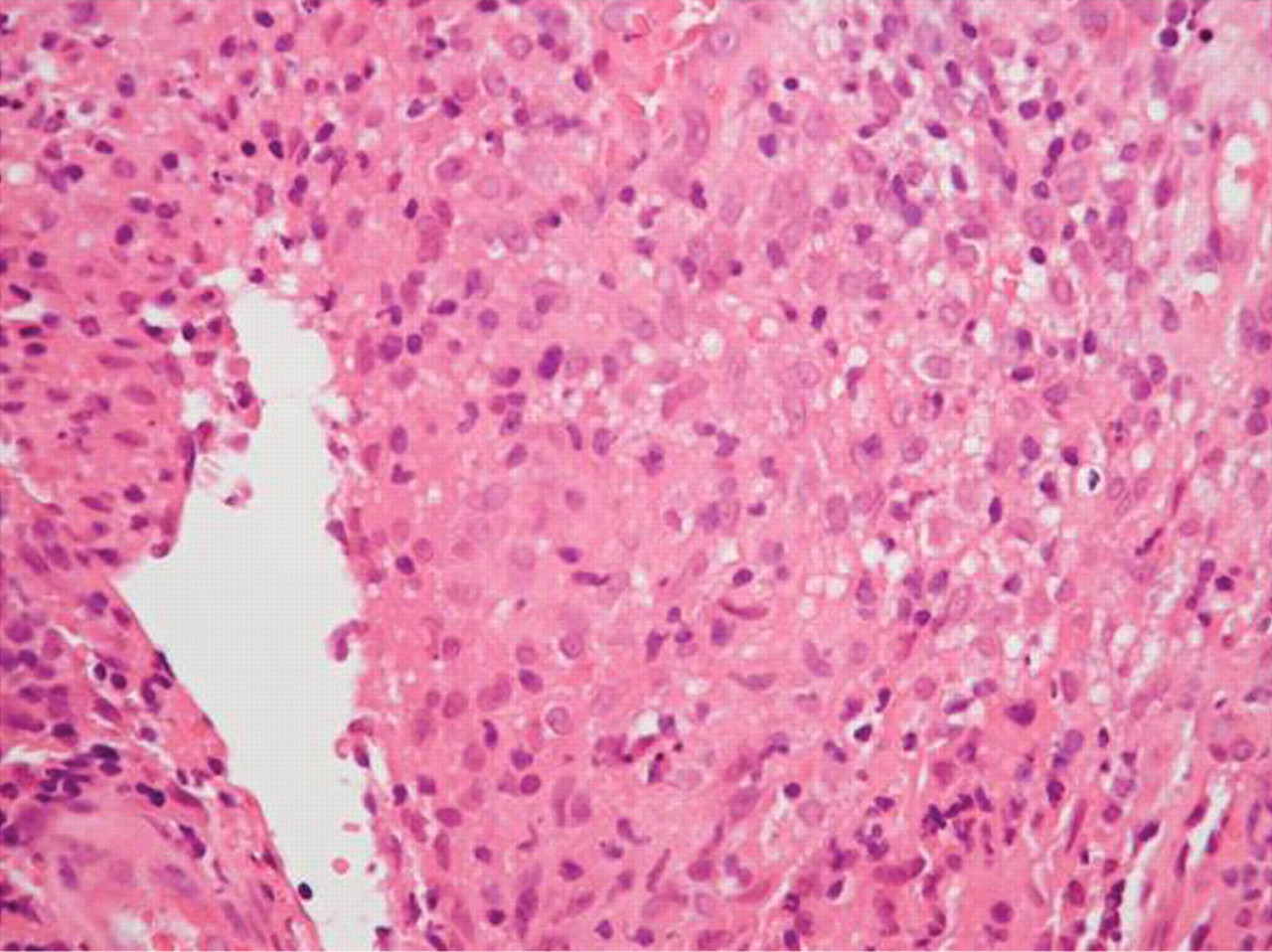
Endobronchial biopsy of case 1 showing loose inflammatory tissue and marked chronic inflammation with sheets of histyocytes. Small vague granulomas can be seen but staining was negative for alkali and acid-fast bacteria and fungi.
A diagnosis of PR was made and the patient was started on prednisolone. Her symptoms resolved rapidly and a chest radiograph 2 months after initiation of steroids was normal (fig. 1d⇑). She completed anti-tuberculous therapy and was also weaned off her steroids without any further complications.
CASE 2
A 33-yr-old Egyptian male presented to the Emergency Department (St Mary’s Hospital) with a history of 15 kg weight loss, night sweats and a productive cough. Radiology and sputum culture confirmed a diagnosis of miliary TB. A lumbar puncture was performed but was culture negative, indicating lack of CNS involvement. He was started on quadruple therapy and when full cultures became available, fully sensitive TB was confirmed. HIV serology was negative.
He had an unsettled initial admission with systemic upset, bilateral pleural effusions and development of deep vein thrombosis and pulmonary embolism. Eventually, 6 weeks following diagnosis he was discharged on quadruple therapy and warfarin. He was then seen in clinic and stepped down to dual therapy. He remained well, but despite pyridoxine he developed mild peripheral neuropathy.
3 months later the patient was admitted as an emergency with left upper quadrant pain and fever. He was systemically unwell with raised inflammatory markers. His haemoglobin had dropped to 8.9 g·dL−1 and he had an INR of 3.2. He was treated for community acquired pneumonia but continued to deteriorate. The pain worsened and he became heamodynamically unstable. Repeat blood investigations at this time revealed a haemoglobin level of 4.3 g·dL−1 and an INR of 5.7. Following initial resuscitation, an urgent CT abdomen was arranged. This revealed a grade 2 splenic rupture and the patient was taken to theatre. A laparotomy was performed and 4 L of blood were in the abdomen. A splenectomy was performed and 12 units of blood were required to resuscitate him. Following surgery he had a difficult recovery with common femoral vein thrombosis and was readmitted following discharge with bowel obstruction secondary to adhesions.
Histology results from the spleen showed multiple large caseating granulomas, one of which had breeched the splenic capsule. Numerous acid-fast bacilli were seen in the necrotic granulomas. There was also marked granulomatous inflammation next to the site of haemorrhage, and it was felt that this episode could be explained by the raised INR in the presence of the high granulomatous load in the spleen. The histology also showed a marked lack of giant cells within the granulomas, perhaps suggesting an impaired immune reaction.
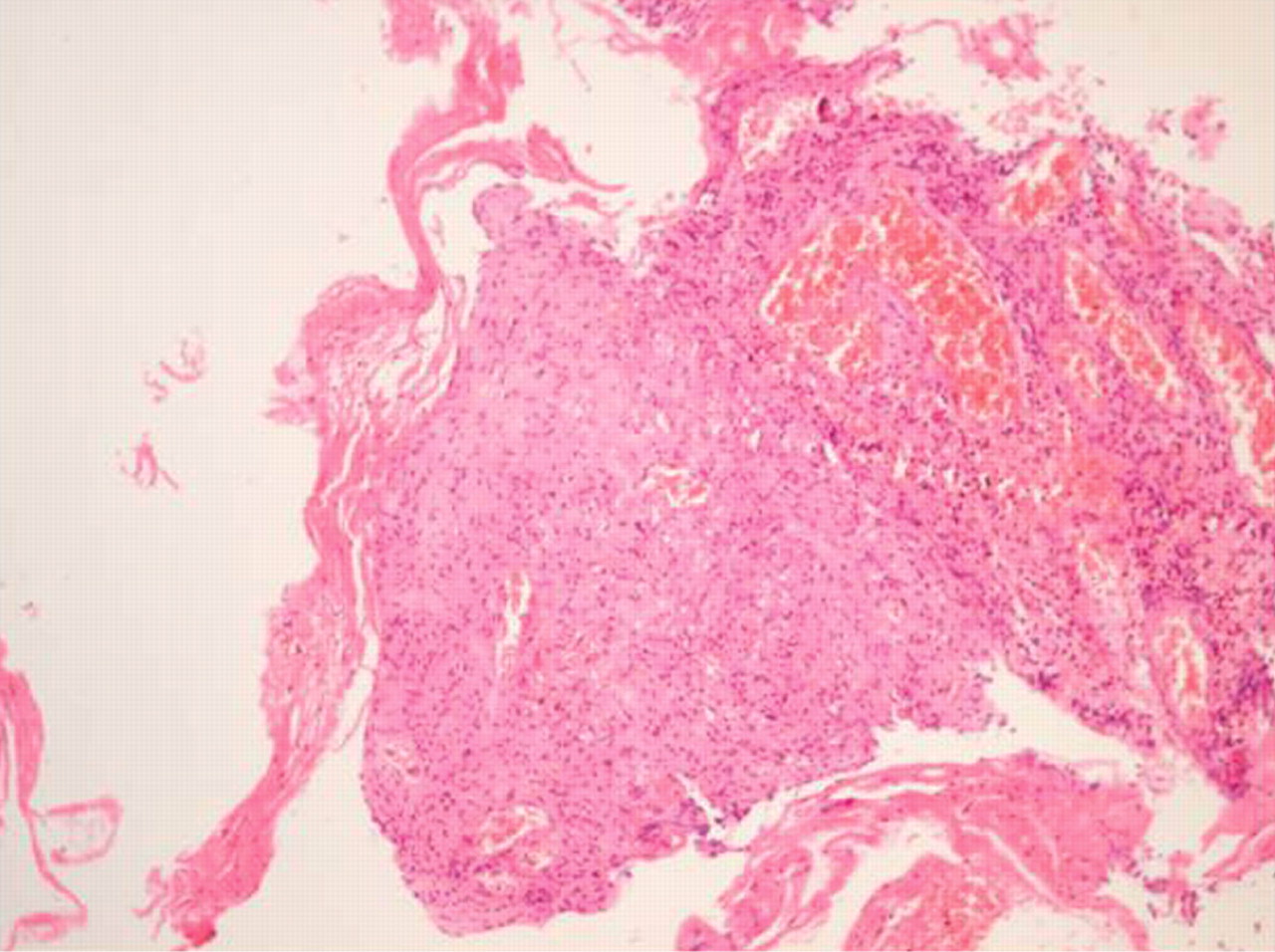
He was discharged as being well, but when seen in clinic there were new infiltrates on the chest radiograph. 9 months following the initial diagnosis he presented with rapid onset of severe shortness of breath and stridor. At the time, CT showed mediastinal lymphadenopathy (fig. 5⇓) and a bronchoscopy was performed which showed a nodular lesion in the mid trachea, causing a marked degree of upper airway obstruction (fig. 6⇓). This was biopsied and histology showed sheets of epithelioid macrophages without giant cells, mixed with other chronic inflammatory cells. Staining for alkali and acid-fast bacteria and fungi were negative and there was no evidence of invasive neoplasia. The final culture was negative (fig. 7⇓).

Computed tomography scan performed in case 2 showing mediastinal lymphadenopathy.

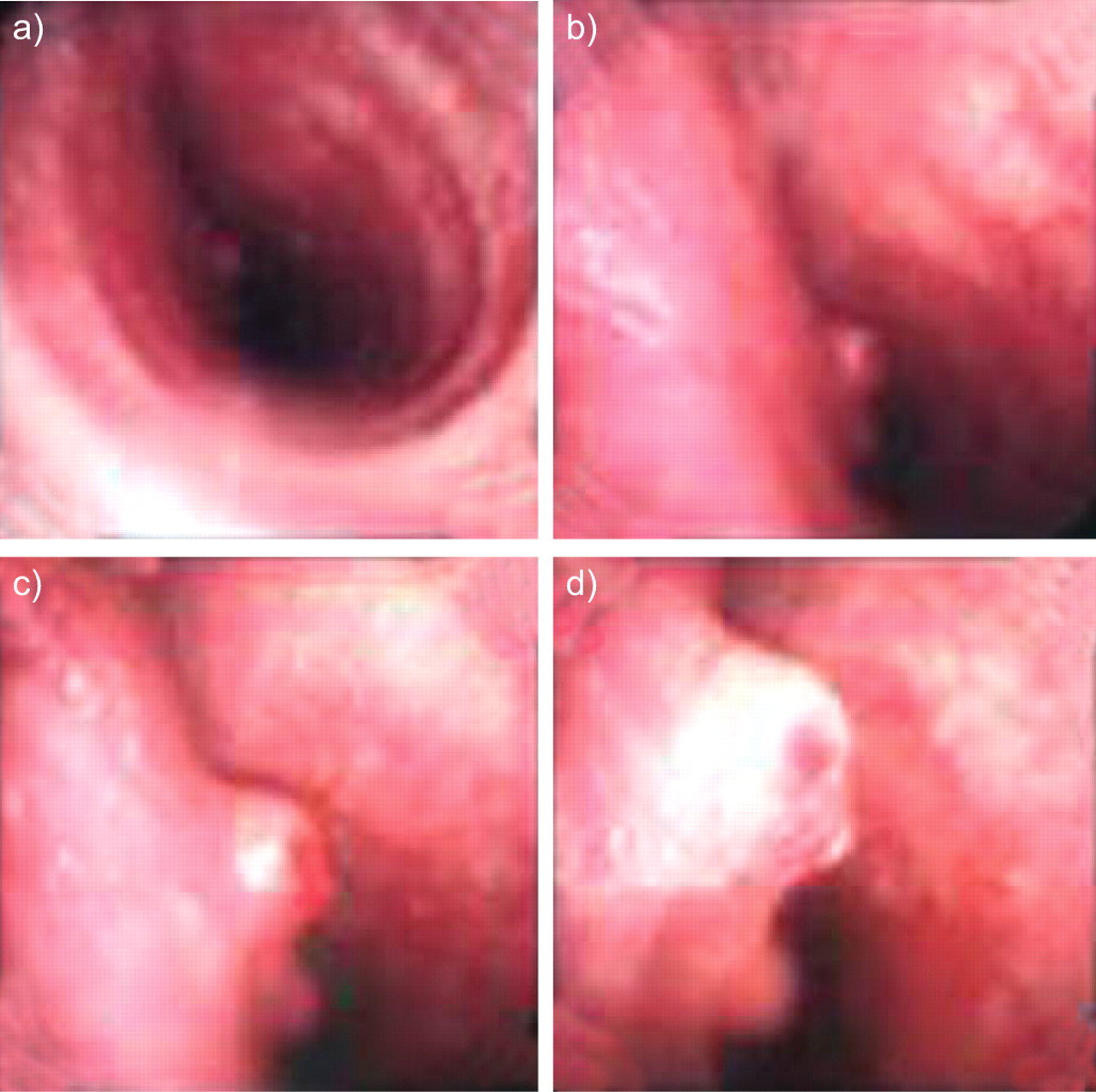
Bronchoscopy performed on case 2 showing the main trachea as seen moving distally.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Endobronchial biopsy from case 2 showing sheets of epitheloid macrophages without giant cells, mixed with other chronic inflammatory cells. Staining for alkali and acid-fast bacteria and fungi were negative. There was no evidence of invasive neoplasia and the final culture was negative.
At this stage, a diagnosis of PR was made and the patient was started on steroids. Follow-up imaging and bronchoscopy 8 weeks later were normal and the patient remains well and free from all treatment.
DISCUSSION
These cases serve to illustrate the importance of PR and the potential to cause significant airway obstruction. It is important to exclude other diagnoses and in both these cases compliance was good, no features of other infection or diagnoses were evident and the paradoxical lesions were negative for TB culture. Endobronchial lesions as seen in these cases are not well described in the literature. The histology in both cases clearly demonstrates a PR and this may represent erosion of mediastinal lymphadenopathy into the airways; in both cases lymphadenopathy was evident and adjacent to the areas of obstruction. It is important to also note that the obstructions were within the airway, i.e. endobronchial, rather than caused by extrinsic compression. Thus, we suggest that these cases represent either the development of a paradoxical mediasinal lymphadenitis with erosion or fistulation into the main airways, or a true de novo endobronchial paradoxical reaction. It is possible that the size of the lesions in our cases were only noted endobronchially, as they were of sufficient size to cause obstructive signs so it was essential to proceed to bronchoscopy whereas the true incidence of endobronchial PR may well be unrecognised in milder cases.
The mechanism for PR lesions is not known but such reactions are a common manifestation in the immune reconstitution syndrome in HIV infected patients who have recently commenced HAART (highly active anti-retroviral therapy). It is generally accepted that PR is due to an abnormality in the immune response and it is possible that the lack of giant cells seen in the splenic granulomas of the second patient reflected a relative lack of an initial immune response. However, there was no suggestion of a defined immune deficiency in either patient prior to treatment. Both cases were HIV negative and most studies of PR patients have not been able to define the exact phenotype of patients developing PR. A rise in lymphocyte count, a tuberculin conversion during treatment and disseminated disease may all be associated with the development of PR [1, 2, 4]. It is also recognised that cases of overwhelming or miliary TB can have poor skin reactivity to tuberculin skin tests in approximately half of such cases and, notably, our second case had miliary involvement.
In summary, we have presented two cases of airway related PR resulting in significant airway obstruction and, therefore, this presentation in any patient on anti-TB treatment should alert the clinician to the possibility of PR. The improved characterisation of individuals at risk from PR in non-HIV infected individuals may be important to allow for earlier identification of PR and potentially earlier intervention. In both our cases, oral steroids were clinically beneficial in terms of the airway manifestations.
Statement of interest
None declared.
Provenance
Submitted article, peer reviewed.
- Received June 9, 2009.
- Accepted July 3, 2009.
- © ERSJ Ltd









