





Abstract
Gastro-oesophageal reflux disease (GERD) is a common disorder in Western countries, and its relationship to airways disorders (e.g. asthma) has been well established. Lung diseases other than asthma have also been associated with GERD, but the nature and scope of this relationship has not been fully defined. Diseases that have been associated with GERD include bronchiolitis syndromes, idiopathic pulmonary fibrosis, scleroderma and nontubercular mycobacterial infection.
Diagnostic evaluation centres upon proving both reflux and pulmonary aspiration, which may be accomplished in some cases by lung biopsy. However, in many cases a compatible clinical and radiographic picture coupled with proof of proximal reflux by combined oesophageal probe testing may suffice for a provisional diagnosis and allow institution of anti-reflux measures.
Proton-pump inhibitors are the medications of choice for GERD; other interventions shown to reduce reflux are weight loss, elevation of the head of the bed and avoidance of recumbency after meals. However, acid suppression therapy does not address non-acid reflux that may be important in disease pathogenesis in select patients, and lifestyle modifications often fail.
Laparoscopic fundoplication is the procedure of choice for medically refractory GERD with excellent short-term results with respect to respiratory symptoms associated with GERD; however, long-term studies document a significant percentage of patients requiring ongoing acid suppression therapy.
Chest physicians generally acknowledge a link between oesophageal disorders and respiratory disease; however, this relationship is complex and may manifest in a variety of clinical entities. A comprehensive, recent article has documented a causal link between gastro-oesophageal reflux disease (GERD) and asthma, chronic cough and posterior laryngitis [1], but in contrast the nature and scope of the relationship between other lung diseases and GERD has not been fully evaluated. This article will review the current knowledge of these disorders.
DEFINITION AND EPIDEMIOLOGY
GERD is defined as “a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications” [2]. This definition serves to differentiate normal individuals with occasional symptomatic reflux from patients with either life-altering symptoms (including extra-oesophageal complaints) or asymptomatic reflux that produces mucosal injury and risk for neoplasia. GERD is a common disorder affecting up to 20% of individuals in Western countries [3]. Risk factors for GERD include hiatus hernia, obesity, older age, alcohol and tobacco use, and male sex [4]; in addition, obstructive sleep apnoea may also confer a risk independent of that due to obesity [5]. Given the obesity epidemic and the aging of the population [6] this prevalence figure is likely to increase.
The high prevalence of GERD contrasts with the rarity of non-asthmatic lung diseases, such as idiopathic pulmonary fibrosis (IPF), which as a group have a poorly defined epidemiology. A recent study [7] using a US healthcare claims database reported the prevalence of IPF as 16.3 and 42.7 per 100,000 persons, using narrow and broad diagnostic criteria, respectively. Despite studies showing a strong association between GERD and respiratory complaints [2, 8, 9], the development of parenchymal lung disease appears to be an exceptional event. One reason for this disparity is that occult microaspiration, the pathological link between GERD and lung disease, occurs in only a minority patients with GERD. Moreover, this appears true even in select patients with extra-oesophageal complications, as shown by two nuclear scintigraphy studies that demonstrated microaspiration in only 5–15% of patients with documented GERD-related cough [10, 11]. In contrast, patients with severe lung disease often have unrecognised pathological reflux. In one study of 65 consecutive IPF patients, 87% had pathological gastro-oesophageal reflux (GER) [12], another study reported GERD in 48–76% of patients following lung transplantation [13–15]. Microaspiration is more likely in the setting of impaired swallowing mechanism and depressed alertness, conditions more prevalent in the elderly, as suggested by one study [16] which showed an association of bilateral chest radiography scarring with pH probe-proven GERD in elderly patients referred for evaluation of gastrointestinal symptoms.
There are also no long-term longitudinal studies of patients with GERD assessing whether parenchymal lung disease develops over time. The few studies attempting to document lung function abnormalities in patients with GERD have been inconclusive. Spechler et al. [17] randomised 207 patients with complicated GERD to different treatment groups and assessed lung function after 1 yr; there were no important differences. Schachter et al. [18] studied 147 obese patients undergoing weight reduction surgery, identifying a reduced diffusion capacity of the lung for carbon monoxide (DL,CO) in those with severe GERD compared to those without GERD. However, the GERD patients were sleepier and older, suggesting that pulmonary vascular disease due to sleep apnoea could have accounted for the difference in DL,CO.
MECHANISMS OF RESPIRATORY DISEASE IN GERD
The lung and oesophagus share a common embryological derivation and innervation by the vagus nerve. The upper oesophageal sphincter lies immediately posterior to the larynx, and the oesophagus runs adjacent to the trachea in the thorax, forming the posterior wall of this structure. GER is a well-documented event in normal individuals, resulting from transient lower oesophageal sphincter relaxation (TLESR). Physiological TLESRs tend to occur after meals, result in brief oesophageal acid contact times and produce no mucosal injury [19, 20]. In contrast, patients with GERD have more frequent TLESR, longer oesophageal acid time and lower oesophageal sphincter (LES) incompetence (prolonged low LES pressure), with the latter phenomenon correlating with endoscopically graded severity of mucosal injury [21]. GER is more likely to be present in several clinical settings (table 1⇓).
Conditions associated with gastro-oesophageal reflux (GERD)
The first clinical setting is primary lung disease, where the thoracic cavity pressure is negative in relation to the abdominal cavity and varies during the respiratory cycle. As such, pre-existing LES incompetence may be worsened by factors producing an increased trans-diaphragmatic pressure gradient, as may occur with lung disease (e.g. increased negative intra-thoracic pressure during inspiration). Moreover, studies of asthmatics undergoing methacholine challenge reveal that bronchospasm increases both TLESR frequency and GER [22, 23].
The second clinical setting is increased intra-abdominal pressure. Conditions that increase intra-abdominal pressure (e.g. obesity, pregnancy and massive ascites) have the potential to increase GER.
The final clinical setting is conditions affecting the intrinsic oesophageal musculature, such as primary myopathic disease, scleroderma, and certain drugs which may adversely affect LES function, thus producing or exacerbating GER.
There are two mechanisms by which GER produces lung disease: 1) reflex neural mechanisms occurring during reflux events limited to the lower oesophagus (distal GER); and 2) direct effect from gastric contents refluxed above the upper oesophageal sphincter (proximal GER) producing upper airway injury and, if aspirated into the tracheobronchial tree, lung disease. A large body of research has examined the relationship between GERD and asthma, and while laryngeal irritation due to proximal GER produces cough and laryngospasm, distal GER alone may also produce functional changes in the respiratory tract. Animal [24] and human studies [25] confirm that distal GER may increase airways resistance and promote airway inflammation by releasing pro-inflammatory mediators [25]. Field et al. [26] also showed that oesophageal acid increases minute ventilation, suggesting another mechanism for respiratory symptoms in GERD patients. Notwithstanding these functional changes, without aspiration parenchymal pathology does not occur.
Normal individuals aspirate small volumes of oral secretions during sleep [27] without sequelae, and this occult aspiration occurs more often in the setting of depressed consciousness [28]. Proximal GER creates the potential for aspiration, the outcome of which varies with the chronicity of the events and the volume and nature of the aspirate. Acute pneumonitis results from aspiration of a large volume of acidic fluid [29], and animal studies have shown this to be a biphasic process [30, 31]: initial chemical injury followed by an inflammatory phase [32–34]. Food particles and low pH act synergistically to produce a more severe injury with a different cytokine profile from that generated by acid alone [35, 36]. In contrast, repeated instillation of small amounts of partially digested vegetable matter with a neutral pH produces a foreign body reaction involving cell-mediated immunity. This latter response results in a pathological pattern of nodular granulomas, giant cells and bronchiolitis with alveolar organisation [37, 38]. Lung disease resulting from GER-related recurrent microaspiration may differ pathologically from the nodular granulomatous pattern if foreign material is absent from the aspirate and, thus, definitive diagnosis by lung biopsy may be difficult. Additionally, the relative importance of non-acid reflux in the development of GERD-related lung disease is currently unresolved, as constituents of gastric juice such as bile acids and pepsin may cause epithelial damage. Bile acids have been identified in the sputum of patients with GERD [39] and have been shown to induce in vitro production of transforming growth factor (TGF)-β1 by human epithelial cells. As TGF-β is important in the fibroproliferative process of IPF [40], this mechanism may factor into the fibroblast proliferation of this disease. Clarifying the pathogenesis of non-acid reflux is important given that proton-pump inhibitors (PPIs), the commonest treatment for GERD, have no effect on non-acid reflux.
CLINICAL SYNDROMES
Lung diseases that have been associated with GERD include nodular granulomatous bronchiolar disease, bronchiolitis obliterans with organising pneumonia (BOOP), IPF and scleroderma, bronchiolitis obliterans following lung transplantation, and nontubercular mycobacterial (NTM) lung infection. Acute lung injury resulting from large volume aspiration of gastric contents (aspiration pneumonitis) is a distinct clinical syndrome [29] which should be differentiated from the more insidious microaspiration-related diseases discussed below.
Nodular granulomatous bronchiolar disease
Patients with neurological disorders (e.g. stroke and Parkinson's disease) and oesophageal diseases (e.g. achalasia) commonly have repeated occult aspiration. Previous autopsy studies [38, 41–43] document a nodular granulomatous process with foreign body reaction in patients with neurological impairment and/or oesophageal disease who aspirated gastric contents containing partially digested vegetable matter, a condition termed lentil pneumonitis [44, 45]. In the study by Knoblich [38] >1,500 autopsies were reviewed and 41 cases of this lesion were found, noting that the diagnostic finding of vegetable matter was often initially missed. More recently, Matsuse et al. [46] analysed >3,000 autopsies from two hospitals in Tokyo, Japan and revealed 31 cases with a similar pathological lesion, which they termed diffuse aspiration bronchiolitis. Medical records in these patients documented a high incidence of cough, sputum production and dyspnoea, in addition to underlying neurological disorders, dementia and oropharyngeal dysphagia. Only half of these patients had documented emesis or gross aspiration.
Foreign material aspiration is required for the development of this lesion, and while most patients with this disorder have obvious neurological compromise or derangement of the swallowing mechanism, some patients apparently only have GERD as the predisposing factor. Barnes et al. [47] reported four patients aged 41–59 yrs with pathologically proven diffuse aspiration bronchiolitis. None of the patients had a disorder associated with altered sensorium and two patients had video fluoroscopy showing no evidence of aspiration; three of these patients had GERD. Mukhopadhyay and Katzenstein [48] reported 59 cases referred for pathological consultation ultimately diagnosed as aspiration-related lung disease. Of these, 10 patients had illicit and/or prescription narcotic drug use as the predisposing factor to aspiration, and 11 had a variety of oesophageal disorders, including three with hiatal hernia. Case reports also describe this disorder in ambulatory patients with dementia who were not suspected of chronic aspiration [49, 50], and in one patient who was found to irrigate her nasal cavity with green tea [51].
BOOP
BOOP has been sporadically reported secondary to occult aspiration related to GER [49, 52], but is rarely mentioned as a condition associated with GERD [53–55]. Sadoun et al. [56] reported a series of five patients with biopsy-proven refractory BOOP who had sustained resolution with therapy solely for GERD. In contrast to patients with nodular granulomatosis, pathognomonic findings of aspiration are absent as there is no identifiable foreign matter in the pathology sections, making the differentiation from other causes of BOOP difficult [57]. Findings suggestive of this condition include multicentric and migratory infiltrates, but an anatomic preference for dependent lung segments has not been evident in the few cases reported. Along these lines, Marumo et al. [58] studied 16 patients with recurrent respiratory symptoms identified from a large group of patients having total gastrectomy. These patients had prominent nocturnal reflux symptoms with productive cough, often followed by morning fever, and many had been evaluated for fever of unknown origin. Although no lung biopsies were performed, these patients are similar to others with BOOP in association with GERD, as they had clinical and laboratory findings of inflammation and chest radiography showing small and multifocal airspace infiltrates without regional preference. The recognition of GERD as a possible aetiological factor in BOOP has important implications, as the usual therapy, corticosteroids, may increase reflux [59].
Fibrosing lung diseases
The classic fibrosing lung disease, IPF, is strikingly similar to the lung involvement occurring in scleroderma. Patients with both disorders present with dyspnoea, inspiratory rales, finger clubbing, exercise-induced hypoxaemia, interstitial and fibrotic radiographic changes, and nonuniform collagen deposition, fibroblastic foci and honeycomb changes on lung pathology [60]. Lung fibrosis in these diseases progresses to death within 3–5 yrs in most patients. Recurrent microaspiration has been identified as a potential risk factor for IPF [61] and is postulated as important in the pathogenesis of scleroderma pulmonary fibrosis and IPF based on the observation of frequent oesophageal dysfunction in both diseases [62, 63]. Oesophageal dysfunction occurring in interstitial lung diseases other than IPF and scleroderma is less well studied, but has been reported [64, 65], suggesting that GERD in fibrotic diseases results from nondisease specific changes in pulmonary mechanics and trans-diaphragmatic pressure gradient.
Scleroderma lung fibrosis
Studies evaluating the role of oesophageal reflux in the development of scleroderma pulmonary fibrosis are limited to small case series employing a variety of indices of oesophageal function. Johnson et al. [66] studied 13 patients with scleroderma, all of whom had abnormal LES function and biopsy evidence of GERD. 10 of these patients had a reduced DL,CO, which was inversely correlated with GERD severity as judged by reflux score, and two had proven aspiration by scintigraphic study. Denis et al. [67] studied 24 scleroderma patients revealing reduced lung compliance in those with impaired oesophageal peristalsis and LES function. Another series of 43 patients [68] demonstrated a correlation between abnormal oesophageal motility and poorer lung function. Kinuya et al. [69] evaluated 47 scleroderma patients showing that higher oesophageal retention of a nuclear tracer (a marker of impaired peristalsis) was correlated with impairment in both DL,CO and forced vital capacity. Marie et al. [70] studied 43 scleroderma patients with oesophageal manometry showing that, although the patients did not differ with respect to disease duration, systemic disease manifestations or inflammatory markers, more severe oesophageal dysfunction was correlated with interstitial changes as shown by high-resolution computed tomography (HRCT) and reduced DL,CO, with a trend toward lower lung volumes. Savarino et al. [71] studied 40 consecutive scleroderma patients with combined oesophageal pH and impedance testing. HRCT evidence of pulmonary fibrosis was found in 18 out of 40 patients, and this group had significantly lower LES pressure, more oesophageal acid exposure, more total and proximal reflux events (both acid and non-acid), and a higher percentage of proximal reflux episodes as compared to those without fibrosis. In contrast, one study of 47 patients found that the presence of proximal reflux was not correlated with lung function, although DL,CO was reduced in patients both with and without reflux [72]. These studies, limited as they are, support the premise that recurrent aspiration plays a role in the progression of scleroderma lung fibrosis, although the association of pulmonary and oesophageal dysfunction could simply reflect a more advanced stage of disease.
IPF
Similar to scleroderma, patients with IPF have a high prevalence of GERD [12, 65, 73–75], leading to the hypothesis that recurrent occult microaspiration may drive the ongoing inflammation characteristic of this disease. This should not be confused with acute exacerbation of IPF (progression of symptoms over weeks with radiographic airspace disease), as biopsies may also reveal organising pneumonia with underlying UIP in this syndrome [76, 77]. Mays et al. [73] reported 131 patients with radiographic pulmonary fibrosis, of which six had recurrent aspiration as their primary diagnosis. 63 were ultimately diagnosed as “idiopathic” fibrosis, and 79% of this group had symptoms of GERD. Additionally, eight patients in this group had surgical lung biopsy showing diffuse fibrosis with areas of bronchiolar damage. Savici and Katzenstein [78] reported surgical lung biopsy findings in six patients with recurrent acute respiratory distress syndrome of unclear aetiology. In addition to the expected finding of alveolar damage, focal acute inflammation and organising pneumonia were also seen. Five of these patients had GERD and four out of the five patients had a history of chronic narcotic use, suggesting a combination of reflux and aspiration; one patient developed chronic lung disease requiring home oxygen therapy.
Recognition of GERD as a potential aetiological factor has important treatment implications, especially since corticosteroids may worsen GERD and continue to be widely used for therapy of IPF despite a lack of definitive clinical trials [61]. Trials of therapy for GERD in patients with established IPF are limited to one retrospective case series [79] of four patients with IPF and documented GERD who were only treated with PPI, these patients stabilised or improved over a 2–3-yr period. Current evidence linking GERD and IPF in a causal relationship is lacking, the hypothesis infers microaspiration from the finding of proximal reflux. However, scintigraphic studies in patients with upper airway complaints [10, 11] suggest that this may be a false assumption as only a minority of patients with proximal reflux aspirate. As such, the question of whether GERD initiates the fibrotic process, participates in driving already established fibrosis or is an innocent bystander remains unresolved.
Bronchiolitis obliterans in lung transplant recipients
Bronchiolitis obliterans syndrome (BOS) is a disease of small airways reflecting chronic allograft rejection and ultimately occurs in about two-thirds of lung transplant patients surviving past the initial post-operative period. BOS manifests clinically as progressive dyspnoea, cough and recurrent infection, with the characteristic finding of progressive airflow limitation on pulmonary function testing. It has been increasingly recognised that GERD, present in 48–76% of patients post-transplantation [13–15], may be a key factor in the development and progression of BOS [80]. Factors predisposing to GERD-related lung disease in this population include gastroparesis [81], vagus nerve dysfunction, a high incidence of post-operative oropharyngeal dysphagia [82], and depressed cough reflex due to the lack of innervation of the allograft [83]. Most lung transplant patients with GERD lack classic symptoms [14], and although acid suppression therapy is frequently given to this patient group, non-acid reflux is present in up to 50% as documented by the finding of bile acids in lung lavage samples [13], a finding associated with BOS in one study [84]. Supporting the aetiological role of GERD in a subset of BOS patients, Davis et al. [85] reported their experience with 43 BOS patients undergoing oesophageal fundoplication, showing lung function improvement (and BOS stage) in 16 cases. In another article, Cantu e al. [15] compared early fundoplication in 14 patients (within 3 months of transplant) with 62 patients undergoing a later operation (mean almost 2 yrs after transplant), suggesting that early surgery may prevent BOS.
NTM infection
NTM infection of the lung may produce a clinical picture of nodular bronchiectasis in nonsmokers [86], and this disease has been associated with oesophageal disorders [87–89]. A recent paper from Korea described 58 HIV-negative patients (86% female) with nodular bronchiectasis due to NTM who had 24-hr oesophageal pH probe evaluation [90]. Pathological acid reflux was identified in 15 (26%) patients, a figure substantially higher than the <5% prevalence reported in Eastern Asia. Moreover, only four (27%) out of the 15 patients had symptoms of GERD. Thomson et al. [91] conducted a case–control study of a cohort of 58 HIV-negative patients with NTM in Australia showing that compared to controls, NTM patients used more acid-suppressing medications and were more likely to have clinically diagnosed GERD and aspiration.
The nature of the linkage between NTM lung infection and GERD is speculative, it is unclear whether acid-suppressing medications predispose to NTM infection or if medication use is simply a marker of severe GERD. There is data that Mycobacterium avium is naturally resistant to acidic pH [92] and in vitro growth is not affected by PPI [93], suggesting that medical therapy of GERD may not be the key factor in pathogenesis.
EVALUATION
Key elements to making the diagnosis of GERD-related lung disease are documenting proximal reflux and aspiration, otherwise there is little established dogma regarding the preferred diagnostic algorithm. As previously discussed, reflux and aspiration warrant consideration in the work up of various lung diseases; however, it must be recalled that GERD is a common condition that may coexist with lung disease by chance alone. Features suggesting a linkage between lung disease and GERD include a suggestive medical history, a compatible radiological picture and certain lung pathological features.
Complaints suggesting the possibility of GERD-related lung disease are nonspecific, including recurrent cough and fever, migratory pulmonary opacities, recurrent pneumonia, and/or exertional dyspnoea with cough. Particular attention should be paid to complaints associated with GERD (e.g. heartburn, waterbrash, change in voice quality and globus sensation) and aspiration (e.g. reported aspiration, dysphagia, cough occurring with oral ingestion, neurological disease and use of sensorium-altering substances). Patients with the latter symptoms should undergo a formal evaluation by a multidisciplinary dysphagia team, which should include a modified barium swallow test [94]. Identifying the origin of the aspiration (e.g. oropharyngeal versus gastro-oesophageal) is crucial for formulating management plans, a previously unrecognised swallowing disorder should be addressed prior to more invasive testing.
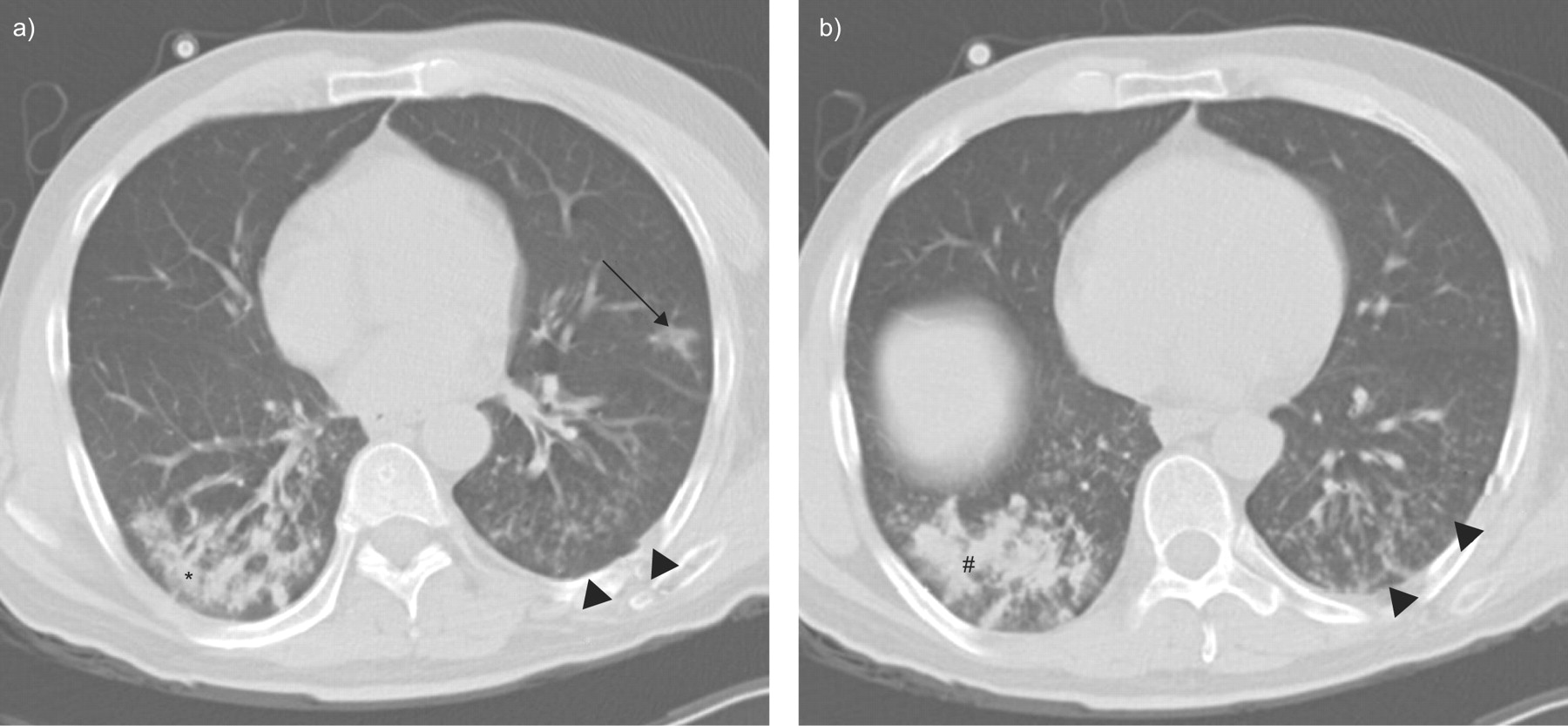
Clinical impression should dictate the pace of evaluation but, generally speaking, chest HRCT scanning is a reasonable starting point in patients with suggestive symptoms. Well-recognised disease-HRCT patterns (e.g. sarcoidosis) should result in evaluation according to published guidelines [95], but certain patterns may be indicative of recurrent aspiration, including multifocal ground-glass opacities, tree-in-bud changes, and ill-defined centrilobular nodules (fig. 1⇓) [50, 96]. In addition, abnormal oesophageal imaging, such as the finding of a dilated oesophagus with an air–fluid level or a large hiatus hernia, support a higher likelihood of proximal reflux. If clinical suspicion remains after assessing the history and HRCT, the clinician must decide whether to proceed directly to lung biopsy based on the likely yield and morbidity of the procedure.

{kind=link}
Computed tomography scan from a male with aspiration revealing nodular airspace infiltration (#), focal ground-glass opacification (arrow) and centrilobular nodules with tree-in-bud changes (arrowheads).
Bronchoscopy with transbronchial biopsy can potentially prove recurrent aspiration if vegetable matter with foreign body reaction is discovered, and can also diagnose other GERD-related conditions, such as NTM infection. Biopsies obtained via bronchoscopy are limited in size and sampling errors are not infrequent, select patients should be considered for surgical lung biopsy with multiple lobe sampling. Nonetheless, even surgical biopsies may not yield diagnostic pathology as in reported cases of GERD-related idiopathic BOOP [49, 52, 56, 57], where microaspiration is presumably devoid of particulate matter. Moreover, elderly and debilitated patients who are at highest risk for foreign material aspiration are often poor candidates for lung biopsy.
Clinical scenarios where biopsy is not the first option and/or the pathology is not definitive should lead to evaluation of GERD (table 2⇓) [97–108]. Combined multi-channel oesophageal impedance and pH-metry probe is the test of choice, detecting both acid and non-acid reflux with high sensitivity and specificity [99], as well as identifying proximal reflux with the potential for aspiration. Other testing modalities have variable utility. Upper gastrointestinal endoscopy can detect mucosal changes diagnostic of GERD (high specificity), and it is important in the evaluation of potentially pre-cancerous lesions associated with chronic reflux, but endoscopy is only ∼50% sensitive for the diagnosis of GERD [97, 109]. Barium oesophagram is a modality limited by poor sensitivity and is not recommended for routine diagnosis [97]. Oesophageal manometry provides information on LES pressure and motility, but as most patients with GERD have normal resting LES tone, this is not recommended during initial evaluation [97]. Nuclear gastro-oesophageal scintigraphy is the only noninvasive test that can provide definitive evidence of GER and pulmonary aspiration. Patients ingest a radiolabelled liquid in the evening with immediate gamma camera scanning to exclude oropharyngeal aspiration, followed by repeat scanning the following morning [66, 110–113]. Identification of tracer in the lungs proves reflux and aspiration with high specificity; however, the sensitivity of this method has not been formally established, being limited by the intermittency of aspiration events and the possibility of tracer clearance (e.g. coughed out) prior to the morning scan.
Tests for gastro-oesophageal reflux disease (GERD) and pulmonary aspiration
Visualisation of the respiratory mucosa may support the diagnosis of oesophageal reflux if posterior laryngeal inflammation and/or contact granulomas of the vocal cords are seen [114]; however, findings are often nonspecific as shown by one laryngoscopic study of normal volunteers where 86% had at least one sign associated with reflux [100]. Bronchoscopy has the advantage of allowing lung biopsy and bronchoalveolar lavage (BAL); the latter technique is useful in excluding infectious agents such as NTM. Lipid-laden macrophages in BAL fluid have been associated with chronic aspiration. This has been formalised as the lipid-laden macrophage index (LLMI) based on the semi-quantitative grading of 100 consecutive BAL-obtained macrophages stained for fat [101]. Most reports describing the LLMI are small case series involving children, with reported sensitivity of 57–100% and specificity of 57–89% [101–107]. Rosen et al. [108] recently reported a series of 50 children undergoing bronchoscopy and combined oesophageal pH and impedance monitoring, and found no correlation between the LLMI and reflux events, endoscopic oesophagitis or response to fundoplication. Other BAL markers of aspiration, bile acids and pepsin, have been identified in patients with GERD and lung disease [115–118], but currently these markers have not been adequately studied as routine diagnostic tests.
Patients with IPF and BOS following lung transplantation have a high prevalence of asymptomatic GERD, and the issue of when to test is unclear. Practice guidelines recommend treating IPF patients for symptomatic GERD [95], but as the role of GERD in driving the disease progression is unresolved [61], it seems reasonable to consider oesophageal probe testing in patients with these diagnoses, especially with features pointing to the possibility of GERD and microaspiration.
MANAGEMENT
There are no large, well-performed trials of the treatment of GERD-related lung disease. Evidence-based practice dictates using best available information for clinical decision-making [119], which in GERD-related lung disease comes from small trials, expert opinion, case reports and extrapolation of data from larger trials addressing other GERD-related complications (e.g. chronic cough). Moreover, as proving microaspiration can be difficult, empirical medical treatment may be warranted in some patients. GERD-related lung disease should improve and/or resolve if reflux and microaspiration is corrected, provided the disease has not advanced to the point of irreversible fibrosis. As such, it is imperative that patients be closely followed to ensure therapeutic effectiveness in addition to standard evaluation of lung disease progression.
General therapeutic goals for patients with GERD-related lung disease include minimising gastric acidity, decreasing oesophageal reflux, enhancing gastric motility and, where relevant, improving swallowing function. PPIs are the agents of choice for treatment of GERD, and anti-reflux medical therapy improves GERD-related chronic cough in 70–100% of patients [120]. Two recent meta-analyses concluded that although PPIs improved cough scores in patients with GERD, there was insufficient evidence to universally recommend PPIs for treatment of either cough [121] or laryngitis/hoarseness due to proximal reflux [122]. The Oporto consensus [99] stated that “reflux is best detected by impedance and its acidity characterized by pH-metry”; thus, one reason for failure of PPI therapy is that these drugs do not address non-acid reflux, which may be important in extra-oesophageal symptom production and lung disease pathogenesis. Moreover, the optimal PPI dose and schedule is uncertain, repeat oesophageal probe testing while receiving treatment should be strongly considered as standard acid suppression therapy was shown to be inadequate in 63% of IPF patients by pH-metry [65]. PPIs are generally safe medications, theoretical concerns regarding the development of gastrointestinal malignancy and predisposition to community-acquired pneumonia with long-term use have not been validated [123, 124].
The approach to patients with persistent symptoms related to GERD despite adequate oesophageal acid control is unclear. Considerations in this group should include pro-kinetic therapy, lifestyle intervention and, ultimately, surgical treatment. Pro-kinetic agents have the conceptual advantage of decreasing both acid and non-acid reflux and may be helpful in patients with proven motility disorders. Nevertheless, they have been relegated to a role secondary to PPIs in GERD management [109, 120], and there has been little formal study in patients with extra-oesophageal symptoms. Older pro-kinetic drugs, metoclopropamide and bethanechol, have frequent side-effects, and cisapride has been withdrawn or restricted in most countries. Domperidone (unavailable in the USA) has been used in the treatment of gastroparesis [125] and as part of a treatment regimen in two small studies of asthmatics with GERD [126, 127], but it may prolong the QTc interval [128]. Finally, baclofen reduces the frequency of TLESR in GERD patients [129, 130] but, to date, has not been well studied in clinical trials.
Lifestyle modifications are attractive to the clinician as they are low cost, relatively risk free, specifically address GERD risk factors, and have been recommended by practice guidelines for treatment of GERD-related cough [120]. However, in practical terms, many patients find these unacceptable or unattainable, and none of these modifications have been specifically evaluated in patients with GERD-related lung disease. Interventions advocated to reduce total reflux time and GERD symptoms include elevating the head of the bed during sleep, avoidance of the right lateral decubitus position and recumbency 3 hr after meals, smoking and alcohol cessation, dietary restrictions and weight loss [109]. A systematic review [131] revealed that elevation of the head of the bed, sleeping in the left lateral decubitus position and weight loss were effective for patients with GERD with moderate strength of evidence; none of the other interventions had significant support from well-performed clinical trials. Weight loss is universally advocated, but the few studies that have evaluated medical weight loss and GERD have yielded conflicting results [132]. However, two well-performed studies did show reduced acid reflux as assessed by pH probe in patients who lost weight [133, 134], and the lack of benefit in other investigations may have been due to the presence of hiatus hernia (unlikely to be effected by weight loss) in study patients [132]. Although seemingly obvious, smoking cessation should be strongly recommended to patients due to its association with both lung disease and GERD. In addition, avoidance of high-fat and high-calorie meals, caffeine, chocolate, mints, citrus, alcohol and tomatoes have been advocated without substantial supporting evidence. Drugs that can lower LES pressure include calcium-channel blockers [135], anticholinergic medications [136], benzodiazepines [137] and theophylline [138], and corticosteroids may worsen GERD [59]; as for dietary recommendations, avoidance of these agents may be helpful. Obstructive sleep apnoea may be an independent risk for GERD [5], and screening for sleep apnoea should be performed as the application of positive airway pressure with sleep decreases nocturnal reflux [136]. Finally, patients with disordered swallowing should be managed in consultation with a dysphagia specialist [137].
Surgical treatment of GERD should be reserved for medically refractory patients, but it must be noted that there are no controlled trials demonstrating efficacy in patients with GERD-related lung disease. As such, the decision to recommend surgery must take into account local expertise and the likelihood of operative morbidity in patients with substantial lung function impairment. Laparoscopic fundoplication is the preferred surgical approach for most patients as it reliably decreases oesophageal acid contact time, increases LES pressure, improves oesophageal symptoms, and decreases proximal reflux [138–142]. Available evidence suggests that fundoplication improves respiratory symptoms in most patients in the short term and has the potential to improve lung function in those with parenchymal lung disease. However, the response of respiratory complaints is less predictable than oesophageal symptoms [143]. The failure of acid suppressant medication to relieve respiratory complaints in patients with proven GERD may be due to non-acid reflux. In this context surgery is an attractive option as it corrects both acid and non-acid reflux [144, 145]. Reports of carefully selected patients undergoing laparoscopic fundoplication document that cough and other respiratory symptoms improve in >80% of patients and completely resolve in >60% [138, 146–148]. There are few studies on the response of parenchymal lung disease to surgical therapy of GERD. Linden et al. [149] performed laparoscopic fundoplication in 19 patients with end-stage lung disease and GERD awaiting lung transplantation; there was a modest improvement in supplementary oxygen requirement but no difference in pulmonary function or six-min walk distance. However, the advanced stage of disease may have precluded a better outcome. Fundoplication in lung transplantation patients with GERD has the potential to improve pulmonary function and delay or prevent BOS. Davis et al. [85] reported 43 patients having laparoscopic fundoplication showing a 24% improvement in forced expiratory volume in 1 s after surgery (1.87 L versus 2.19 L; p = 0.00002). The benefit was greatest in patients with earlier stage BOS and relatively preserved lung function. A subsequent paper from this group [15] compared early fundoplication in 14 patients (within 3 months of transplant) to 62 patients having the operation later (almost 2 yrs after transplant), showing that 100% of the early surgery group remained free from BOS, suggesting that early surgery may prevent BOS in patients with GERD.
Morbidly obese patients with GERD and lung disease may be candidates for bariatric surgery if medical weight loss attempts fail. In this setting, laparoscopic Roux-en-Y bypass appears to be the favoured procedure, resulting in sustained weight loss, improved GERD symptoms, and it has been reported to benefit GERD patients <100 lbs overweight [150]. In contrast, the commonly performed adjustable gastric band procedure may increase GERD [151, 152]. In a series of 152 obese patients (mean body mass index 48 kg·m−2) with chronic GERD undergoing laparoscopic Roux-en-Y bypass, >80% had GERD symptom resolution 6 months after surgery, and there was a significant decrease in patient-reported laryngitis, wheezing and aspiration [153].
Lastly, enthusiasm for surgical treatment of GERD should be tempered by long-term follow-up data showing persistent GERD symptoms and medication use in many patients [154]. Spechler et al. [155] reported 10-yr outcomes in patients randomised to surgical or medical management of GERD as part of the VA Cooperative study, showing that while 92% of medically managed patients continued to use anti-reflux medications, 62% in the surgery arm also required medical therapy.
CONCLUSION
GER and aspiration should be strongly considered as possible aetiological factors in a variety of lung diseases including bronchiolitis syndromes, pulmonary fibrosis and NTM infection. In addition to clinical suspicion, HRCT is important in suggesting these diagnoses. Evaluation strategies should focus on proving proximal reflux and pulmonary aspiration. Lung biopsy, oesophageal probe, direct airway visualisation, upper gastrointestinal endoscopy and nuclear scintigraphic studies are all potentially useful modalities, but all have significant limitations, and the diagnostic approach should be tailored to the individual patient. Treatment consists of acid suppression and lifestyle modifications; refractory cases should be considered for laparoscopic fundoplication, understanding that a significant percentage will nonetheless require long-term acid suppression therapy.
Statement of interest
None declared.
Provenance
Submitted article, peer reviewed.
- Received April 17, 2009.
- Accepted May 3, 2009.
- © ERSJ Ltd
References









