





Abstract
There is a strong clinical rationale for combination therapy in pulmonary arterial hypertension (PAH), as several pathological pathways have been implicated in its pathogenesis and no single agent has yet been shown to deliver completely satisfactory results. Registry data indicate that use of combination therapy is in fact common in existing clinical practice, even though support has been largely empirical or derived from small-scale observational studies. Data from large, adequately powered, randomised controlled trials of combination therapy in PAH are now emerging and suggest that combination therapy may be clinically beneficial. Studies of bosentan in combination with prostanoids and phosphodiesterase (PDE)-5 inhibitors show consistent evidence of improvements in exercise capacity compared with placebo. Similar improvements have been observed with PDE-5 inhibitors in combination with prostanoids. The appropriate timing of combination therapy requires further evaluation but goal-oriented therapy using combinations of oral and inhaled drugs has been shown to provide acceptable long-term results in patients with advanced PAH. Monitoring should be performed regularly and be based on repeatable, noninvasive, measurable parameters that have prognostic value.
- Combination therapy
- endothelin receptor antagonists
- phosphodiesterase type-5 inhibitors
- prostanoids
- pulmonary arterial hypertension
Pulmonary arterial hypertension (PAH) is a devastating disease with a traditionally poor prognosis [1]. The progressive increase in pulmonary vascular resistance (PVR) that characterises PAH results in extensive structural changes in the heart, limits exercise capacity and, eventually, leads to right ventricular failure and death [2]. PAH can be idiopathic, or associated with other diseases, such as systemic rheumatic or connective tissue diseases, congenital heart defects, portal hypertension and HIV infection, or occur following treatment with anorexigens [2]. Despite its varying aetiology, all patients with PAH show similar obstructive pathological changes in the small pulmonary arteries and arteriolae, suggesting a common, underlying pathobiology [3].
Although the pathogenesis of PAH remains to be fully elucidated, it is thought to arise, at least in part, from disturbances in the normal balance between endogenous vasoconstrictors, such as endothelin, and vasodilators, such as prostacyclin and nitric oxide, in response to endothelial dysfunction or injury [4, 5]. These discoveries have led to the development of therapies targeted at the prostacyclin-, nitric oxide- and endothelin-mediated pathways, with treatments designed to promote vasodilation and inhibit cell growth, e.g. with prostanoids, phosphodiesterase (PDE)-5 inhibitors and endothelin receptor antagonists (ERAs).
Targeted therapies constitute a major advance in the treatment of PAH, with single-treatment regimens leading to disease stabilisation and functional improvement in significant numbers of patients. A recent meta-analysis including 23 randomised controlled studies has also shown improvements in survival and a reduction in the hospitalisation rate [6]. Nonetheless, despite these advances, PAH remains a progressive, debilitating disease with high mortality. Thus, there is still a need for further treatment options in those patients who do not stabilise on monotherapy and for those who show initial symptomatic improvements but later regress [7]. Combination therapy using drugs targeted at the different pathways implicated in pulmonary vascular dysfunction is a logical, increasingly used option in the management of PAH, albeit largely empirically based [6, 8]. In this review, we will discuss the rationale for using combination therapy in PAH, examine the growing body of evidence to support its clinical use, and consider which patients might benefit most.
RATIONALE FOR COMBINATION THERAPY
Although treatable, PAH is still an incurable disease. Given the malignant nature of PAH, there is a case for taking an aggressive approach towards treatment. Certainly, this approach has been successfully employed in the treatment of other serious diseases, such as congestive heart failure [9], HIV infection [10] and cancer [11], where use of combination therapy is routine. Moreover, with evidence to suggest that at least three separate pathways are involved in the pathogenesis of PAH, there is a sound rationale for the concomitant use of two or more drugs in the treatment of PAH. To date, no single agent has been shown to deliver completely satisfactory improvements in patients in World Health Organization (WHO) functional class III/IV who have a poor prognosis despite targeted monotherapy. Obviously any clinical benefit to be derived from combining two or more drugs has to be considered in light of the risk of drug–drug interactions and the possible increased risk of side-effects.
CURRENT DATA ON COMBINATION THERAPY
Drug therapy for PAH, which presently includes prostanoids, ERAs and PDE-5 inhibitors, is recommended in treatment guidelines for most patients with PAH [12–14]. However, these guidelines primarily focus on the use of monotherapy in patients with advanced disease (WHO functional class III/IV); combination therapy warranted little mention in early treatment algorithms where it was seen primarily as reserve therapy before recourse to lung transplantation. Now, however, as data from clinical trials designed to evaluate the efficacy and safety of combination therapy has become available, this approach may be revised.
ERA plus prostanoids
The BREATHE-2 trial (Bosentan Randomised Trial of Endothelin Antagonist Therapy for PAH) was the first randomised, double-blind, placebo-controlled study to explore the potential clinical benefits of simultaneously combining bosentan with epoprostenol in treatment of severe PAH (WHO functional class III/IV) [15]. Of the 33 patients enrolled, those in the combined treatment arm showed a trend, albeit not statistically significant, towards improvements in cardiopulmonary haemodynamics compared with those on epoprostenol alone. The subsequent STEP study (Safety and Pilot Efficacy Trial in Combination with Bosentan for Evaluation in Pulmonary Arterial Hypertension) in 67 PAH patients (mostly WHO functional class III) showed that the addition of inhaled iloprost to stable bosentan monotherapy resulted in significant improvements in functional class, haemodynamics and time to clinical worsening when compared with placebo [16]. Change from baseline in 6-min walking distance (6MWD) also showed greater improvement in patients receiving combination therapy compared with placebo recipients (p = 0.051). Combination therapy proved both efficacious and well tolerated; syncope was notably less frequent and severe in the combination treatment arm than that reported in the AIR (Aerosolised Iloprost Randomised) study, possibly because of background bosentan therapy.
The potential benefits of combining bosentan with the long-acting prostacyclin derivative treprostinil have been investigated in two recently published studies [17, 18]. In an open-label study in 12 patients with symptomatic PAH despite bosentan treatment, the addition of inhaled treprostinil led to significant improvements in 6MWD and functional class (nine out of 11 patients improved from WHO functional class III to II), as well as haemodynamics and time to clinical worsening [17]. Significant improvements in exercise capacity from inhaled treprostinil as add-on therapy to bosentan (or sildenafil) have since been confirmed in the large, randomised, double-blind, placebo-controlled TRIUMPH I (Treprostinil Inhalation Used for the Management of Pulmonary Hypertension) study [18]. Of the 212 (90%) patients who completed 12 weeks of combination therapy, median 6MWD increased by 20 m compared with placebo (p<0.0006). This was consistent with other studies, and combination treatment was well tolerated.
ERA plus PDE-5 inhibitors
Both bosentan and PDE-5 inhibitors are administered orally, making concomitant administration simple and convenient. Evidence that bosentan in combination with sildenafil may benefit patients with mildly symptomatic disease (WHO functional class II) emerged from the EARLY (Endothelin Antagonist Trial in Mildly Symptomatic PAH patients) trial that included a subgroup of patients treated with sildenafil [19]. As patients in this randomised, double-blind, placebo-controlled trial were stratified according to sildenafil use at baseline, concomitant treatment with bosentan could be assessed prospectively. Results showed that, compared with placebo, treatment with bosentan produced significant haemodynamic improvements (reductions in PVR) and prevented clinical deterioration, including in the subgroup of sildenafil-treated patients. Haemodynamic improvement was also observed in COMPASS-1 (Haemodynamic effects of a single dose of sildenafil in symptomatic patients on bosentan treatment for pulmonary arterial hypertension), a prospective, open-label, noncomparative, pharmacodynamic study, in which 45 patients with PAH received single-dose sildenafil on stable bosentan therapy. Here, acute administration of sildenafil produced significant reductions in both PVR (fig. 1⇓) and total pulmonary resistance [20]. Importantly, this trial demonstrated that the pharmacokinetic interaction between bosentan and sildenafil may be of no clinical relevance and, moreover, that there is a favourable acute pharmacodynamic effect when these drugs are co-administered.

Reduction in mean pulmonary vascular resistance (PVR) in 37 subjects following acute sildenafil administration to ongoing bosentan therapy in the COMPASS-1 (Haemodynamic effects of a single dose of sildenafil in symptomatic patients on bosentan treatment for pulmonary arterial hypertension) study at baseline-2 (mean 889, 95% CI 656–1,121) and 60 min after sildenafil (mean 778, 95% CI 561–995) (per-protocol set). Mean per cent change -15%; 95% CI -21– -10; p<0.0001. Data taken from [20].
More recently, data were reported from the PHIRST-1 study (Tadalafil in the Treatment of Pulmonary Arterial Hypertension), a randomised, double-blind, placebo-controlled trial in 405 patients with PAH treated with tadalafil [21]. Among this patient population, ∼53% (n = 216) of patients received tadalafil or placebo in addition to bosentan. Overall, significant improvements in 6MWD and a significant delay in time to clinical worsening were observed in the 40-mg tadalafil dose group, accompanied by improvements in health-related quality of life (HRQoL). In a subgroup analysis, an improvement in exercise capacity was observed in patients who received tadalafil in addition to background bosentan therapy.
PDE-5 inhibitors plus prostanoids
As discussed previously, results from the TRIUMPH I study showed that addition of inhaled treprostinil to ongoing sildenafil (or bosentan) therapy led to significant improvements in exercise capacity in patients with advanced PAH (WHO functional class III/IV) [18]. Recently published data from the large randomised, double-blind, placebo-controlled PACES (Pulmonary Arterial Hypertension Combination Study of Epoprostenol and Sildenafil) trial confirm these findings. This study of 267 patients showed that addition of sildenafil to stable intravenous epoprostenol resulted in a significant improvement in 6MWD compared with placebo (fig. 2⇓) and, furthermore, was accompanied by positive changes in haemodynamics, time to clinical worsening and HRQoL [22]. Combination treatment was generally well tolerated with the benefits being considered to outweigh the increased rates of headache and dyspepsia seen in the combination treatment arm.

The effect of sequential addition of sildenafil to first-line epoprostenol on exercise capacity measured using 6-min walk distance (6MWD) in the PACES clinical trial (Pulmonary Arterial Hypertension Combination Study of Epoprostenol and Sildenafil). ▪: epoprostenol plus sildenafil; •: epoprostenol plus placebo. #: placebo-adjusted increase of 28.8 m, 95% CI 13.9–43.8; p<0.001. Reproduced from [22] with permission of the publisher.
Data from large, adequately powered, randomised controlled trials of combination therapy in PAH are only now being published, with further combination treatment studies still in the pipeline. Nonetheless, they point towards encouraging results and augment earlier findings from a number of small studies and case reports, the vast majority of which support the view that combination therapy is beneficial in patients who fail to respond to an initial course of monotherapy or begin to deteriorate while on monotherapy (table 1⇓) [16, 23–45]. In fact, as data from the large REVEAL Registry (Registry to Evaluate Early and Long Term PAH Disease Management) demonstrate, combination therapy is commonly used in clinical practice despite the relative lack of supporting data.
Summary of combination therapy studies in pulmonary arterial hypertension(PAH) involving small numbers of patients and case reports
WHEN SHOULD COMBINATION THERAPY BE CONSIDERED?
At present there is no known cure for PAH, thus current therapy aims to improve and/or stabilise haemodynamics, symptoms such as dyspnoea, exercise capacity, HRQoL, morbidity (including hospitalisation) and survival [12]. Naturally, these goals will depend on the stage of disease at diagnosis, with prevention of disease progression being the goal in early-stage disease versus clinical improvement in advanced stages. Other factors to take into account include the patient's physical and mental state, underlying disease and comorbidities, as well as the patient’s priorities and wishes.
As it is important to set treatment goals that are known to be associated with improved outcome, follow-up parameters should not only be repeatable, noninvasive and assessable, but also of prognostic importance. Useful parameters include: 6MWD; cardiopulmonary exercise testing (peak oxygen uptake (V′O2)); haemodynamics (cardiac index and right atrial pressure); and possibly biomarkers, such as brain natriuretic peptide (BNP) and N-terminal pro-BNP. Pulmonary arterial pressure is not considered a suitable follow-up parameter because it correlates poorly with disease severity and is, therefore, of limited prognostic value [12].
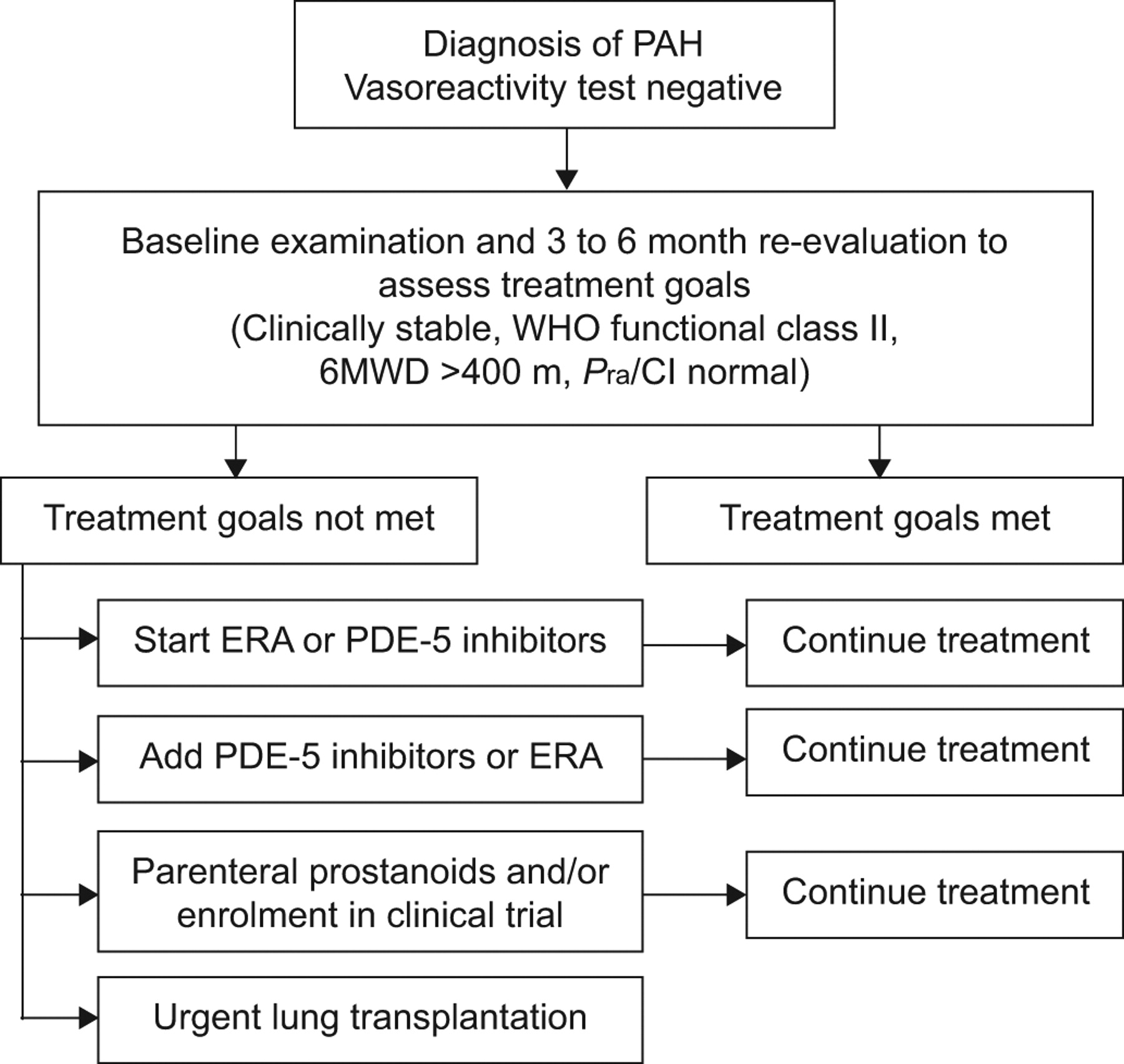
A study using a goal-orientated approach to therapy, whereby patients in whom pre-defined treatment goals were met continued with bosentan while patients who did not meet the treatment goals were successively given sildenafil and then inhaled iloprost, has been shown to provide acceptable long-term results in patients with advanced PAH [7]. In this study, in which treatment goals were a 6MWD of >380 m, a peak V′O2 of >10.4 mL·min−1·kg−1 and a peak systolic blood pressure of >120 mmHg during exercise, survival (primary end-point) was significantly better over 3 yrs compared with both historical controls and expected survival estimates (fig. 3⇓), with combination treatment also reducing the need for i.v. prostanoids or lung transplantation. A suggested treatment algorithm based on the results of this study is illustrated in figure 4⇓. In addition to the treatment goals suggested in the algorithm, haemodynamic goals such as a cardiac index >2.4 L·min−1·m−2 and a right atrial pressure <10 mmHg assessed by follow-up right heart catheterisation are considered appropriate in other treatment centres; in younger patients a treatment goal for 6MWD of >500 m may also be considered. The algorithm posits that combination therapy should be initiated when no improvement is apparent after 3–6 months of initial treatment, when pre-defined treatment goals have not been met after 3–6 months, or when the patient worsens. Currently, combination therapy appears best suited to patients with suboptimal response to therapy, such as those in WHO functional class III/IV who fail to improve on initial therapy and those in WHO functional class II who fail to stabilise.

Kaplan–Meier survival estimates for goal-oriented therapy compared with historical treatment and expected survival. ––––: treatment group, 2002–2004; ········: historical control group, 1999–2001; ▪: expected survival. Treatment group versus historical control group, p = 0.011; treatment group versus expected survival, p<0.001 for all time-points. Reproduced from [7] with permission from the publisher.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
An example of an algorithm for goal-oriented therapy in pulmonary arterial hypertension (PAH). WHO: World Health Organization; 6MWD: 6-min walk distance; Pra: right atrial pressure; CI: cardiac index; ERA: endothelin receptor antagonist; PDE: phosphodiesterase. Reproduced from [7] permission from the publisher.
An emerging and fascinating concept relates to the use of first-line combination therapy with two drugs in PAH patients as compared to initial monotherapy. This hypothesis was tested in the BREATHE-2 trial, but the small sample size of the study did not allow a definitive conclusion [15]. The appropriate design to assess the efficacy of this strategy appears to be a three-arm study, comparing combination therapy with two arms of monotherapy using the single compounds.
CONCLUSIONS
The chronic and rapidly progressive nature of PAH provides a strong rationale for use of combination therapy; indeed, combination therapy is now recommended in new treatment guidelines. Experience to date with combination therapy is encouraging, with multiple combinations proving effective and, importantly, well tolerated. The appropriate timing of combination therapy and whether it should be simultaneously or sequential requires further evaluation. A goal-oriented approach to combination therapy seems to be appropriate given the current available data on efficacy and safety. Patients with PAH should, therefore, be reassessed every 3–6 months and the addition of a new therapy considered when treatment goals have not been met. Controlled clinical trials are underway that will provide important answers to the long-term safety and efficacy of combination therapy in PAH.
Statement of interest
N. Galiè has participated in advisory board activities for Actelion, Pfizer, United Therapeutics, Eli Lilly, Bayer Schering, Encysive and GlaxoSmithKline. He has been a paid lecturer for Actelion, Pfizer, Bayer Schering, and GlaxoSmithKline. His Institute has received grant support from Actelion, Pfizer, United Therapeutics, Eli Lilly, Bayer Schering, Encysive, and GlaxoSmithKline. G. Simonneau has received consulting and lecture fees and research support from Actelion Pharmaceuticals, Bayer Schering, GlaxoSmithKline, Eli Lilly and United Therapeutics.
Provenance
Publication of this peer‐reviewed article was supported by Actelion Pharmaceuticals Ltd, Switzerland (unrestricted grant, European Respiratory Review issue 113).
Acknowledgments
We received editorial assistance from Elements Communications Ltd (Westerham, UK), supported by Actelion Pharmaceuticals Ltd (Allschwil, Switzerland).
- Received June 11, 2009.
- Accepted June 24, 2009.
- © ERSJ Ltd
References









