





Abstract
The present article aims to define what tobacco control is both in Europe and around the world. The situation of tobacco control in Belgium will be compared to other European countries using the tobacco control scale (TCS). If countries demonstrating a high TCS score have lower tobacco smoking prevalence than countries with a low TCS, it is not known whether the decrease in smoking prevalence over several years is well correlated with the increase in TCS score in each country during the same period.
Moreover the article will raise the question of how far research will continue control into controlling the use of tobacco.
The remaining 20% of smokers in the best tobacco control scale countries who are still smoking are not similar to the 20% that are now ex-smokers. Indeed we are now facing the “hard core smokers”, who show great resistance to policy measures and be considered as ill individuals requiring specialised care rather than individuals with bad habits. The future tobacco control scale should place more importance on the quality of care and the implication of European countries providing improved access to this form of care and validated forms of treatment of this chronic, difficult to treat disease.
A DEFINITION OF TOBACCO CONTROL
The control of the 20th century “tobacco epidemics”, so called by the World Health Organization (WHO), needs a set of political measures aiming to curb the epidemics, which are still present in the 21st century, with an adequate strategy. The idea of building an international instrument was initiated in May 1995 at the 48th World Health Assembly.
In 1999 Dr Gro Harlem Brundtland, making global tobacco control a priority of WHO, started work towards building an international treaty, the Framework Convention on Tobacco Control (FCTC) [1].
The key elements of the treaty deal with: 1) advertising, sponsorship and promotion of tobacco products; 2) packaging and labelling of those products; 3) protection from exposure to tobacco smoke; and 4) illicit trade in tobacco products.
The ban of tobacco products from public use is not new: Pope Urban VII, in 1590, threatened to excommunicate anyone who “took tobacco in the porchway of or inside a church, whether it be by chewing it, smoking with a pipe or sniffing it in powdered form through the nose” [2].
The World Bank proposed six policies, some of which are also present in the FCTC [3]: 1) price increases through higher taxes on cigarettes or other tobacco products; 2) bans and/or restrictions on smoking in public places and workplaces; 3) better consumer information, including public information campaigns, media coverage and publicising research findings; 4) comprehensive bans on the advertising and promotion of all tobacco products, and on logos and brand names; 5) large, direct health warning labels on cigarette boxes and other tobacco products; and 6) treatment to help dependent smokers stop, including increased access to medications.
TOBACCO CONTROL TODAY IN BELGIUM AND EUROPE
Based on the six policies proposed by the World Bank, Joossens and Raw [4] have proposed a tobacco control scale (TCS) with a maximum score of 100. The scoring system gives a high value to the pricing (30 points) and a low score to health warning labels and to treatment to help dependent smokers (10 points). Bans on smoking in public and work places receive 22 points, whereas spending on public information is given 15 points, compared with a ban on advertising, which is given 13 points. The scoring system can be criticised but, at least, the merit of the instrument is its existence.
The reason for the high score given to pricing is illustrated by numerous studies in several countries, such the report by Townsend [5] in the UK, showing the opposing trends of cigarette price and consumption in the UK during the years 1970–1994: when the real average price progressively climbed from around £1.50 to £2.40, the consumption fell by 35%, which corresponds to a price elasticity of ∼0.5. One of the main supporters of a heavy taxation of tobacco products is F.J. Chaloupka, who has written a number of papers on the subject (summarised in the publications of ImpacTeen (www.uk.edu/org/impacteen), a foundation dedicated to youth health where he acts as director), and who stated that: higher taxes induce quitting, reduce consumption and prevent starting; and that a 10% price increase reduces demand by 4% in high-income countries and by double this percentage in youngsters and low-income countries [6].
The second highest score is given to smoking bans in public places and workplaces, which is also in accord with the scientific literature for three reasons: 1) the harmful effects of second-hand smoke [1]; 2) healthcare costs [7]; and 3) positive influence on quitting by smokers [8].
The work of Farelly et al. [8], concerning almost 98,000 indoor workers, concludes that a 6% reduction in prevalence of smoking in that population led to a 14% average fall in daily consumption among smokers and to a possible 10% reduction of prevalence if the ban was totally implemented everywhere.
The Cochrane Database on the subject in 2005 is less optimistic, as it states “conflicting evidence about whether they decrease prevalence of smoking or overall consumption of tobacco by smokers” [9].
If we go back to policy, and to the evolution of the TCS in Europe, it has evolved in the right way even within a short time of 2 yrs [10].
The total score for all 30 European countries improved from 47 to 52 between July 2005 and 2007. The main improvement comes from bans on smoking in public and work places, with 11 points in 2007 compared with eight in 2005, and ban on advertising, which climbs from nine to 11. The financial support for dependent smokers does not improve, with the score remaining at five.
The ranking for Belgium rose from 12th place to 8th. The UK has improved its overall score from 73 to 93; Ireland remains at 74 points, falling from first place to second in Europe.
Nevertheless, one question remains: is this ranking correlated with the decrease in smoking prevalence in each of the 30 countries? There is no clear answer because there is no standardised tool for measuring smoking prevalence. If we look to Ireland, a country with a very good position in tobacco control, a decrease in prevalence of smoking can be seen 3 months after March 2004, when the laws restricting tobacco use were fully implemented.
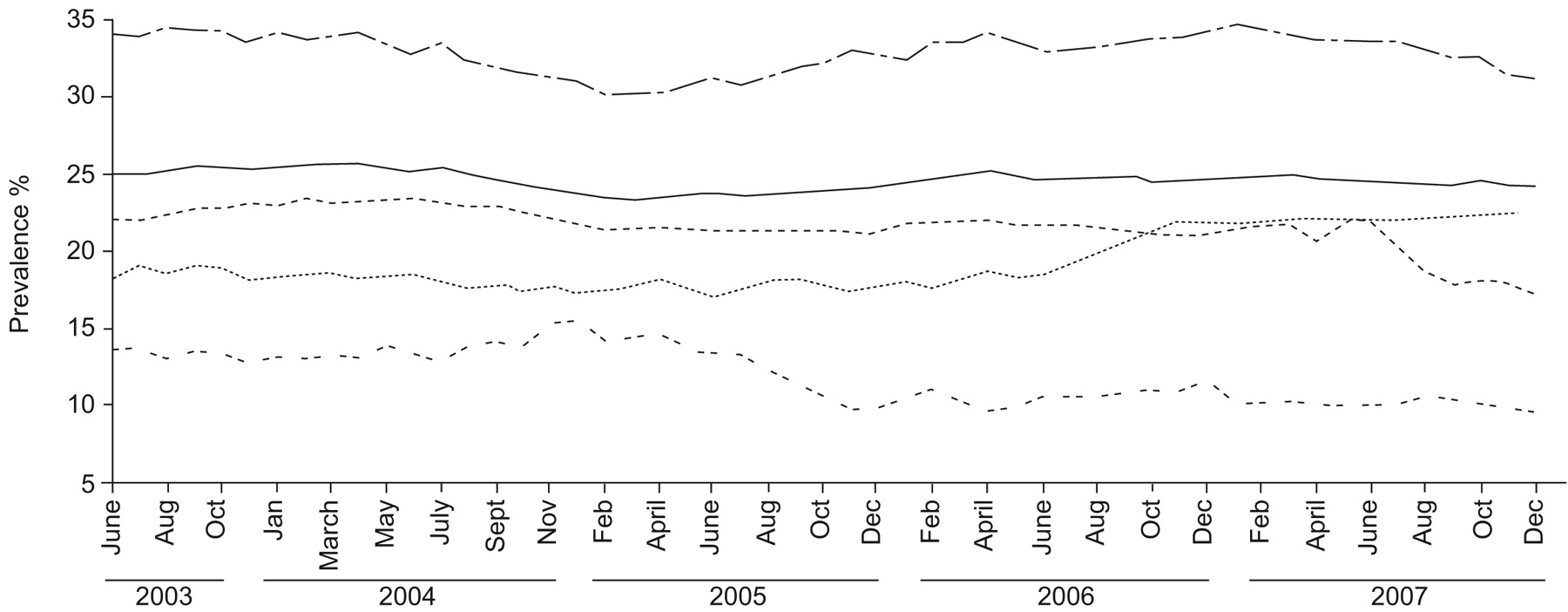
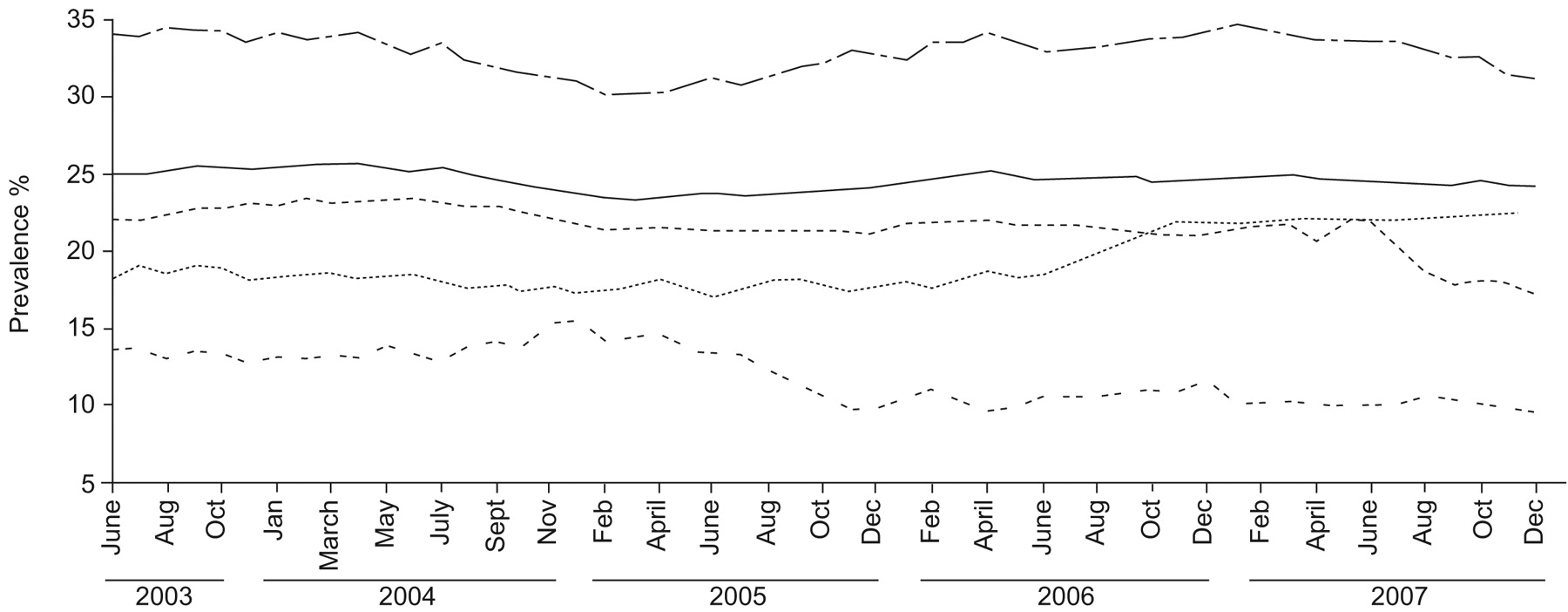
In this country we have, through the Office of Tobacco Control, a monthly record of cigarette smoking prevalence, which shows a trend towards an increase of this prevalence that began in April 2005 (fig. 1). A plateau is observed from February 2006 around a value of 24.5% smokers, with a slight trend towards a decrease since November 2007. There is a prevalence of 23.5% in July 2005 and of 24.5% in July 2007, the time when the TCS was determined. This seems to demonstrate a possible limit of the policy measures.
There is no doubt about the fact that countries with a good performance in the TCS score have a lower prevalence of smoking than the countries with a poor ranking. Nevertheless, it is not known if the policy of today will still be the policy for tomorrow, at least in the countries scoring highly in the TCS.
We are now more and more facing, indeed at least in the best performing countries, the hard core of smokers who will continue to smoke despite their intention to stop. In 2005, 68% of smokers in the UK said that they wanted to give up, but 56% said it will be difficult to go without smoking for a whole day. In Norway, a prosperous country that performs well in tobacco control, the number of daily smokers aged 16–74 yrs was still 25% in 2006, plus 11% occasional smokers [11].
The limits of the pricing policy have been mentioned in various studies, owing to the following reasons.
1) Smuggling, with the famous example of Canada where Native Americans smuggled tobacco products from the USA to Canada with some impunity through tribal sovereignty with participation of the tobacco industry [12]. This problem of smuggling led the government of Quebec to opt for a reduction of its taxes on tobacco in order to fight smuggling [13].
2) Purchase of tobacco via the internet [14].
3) Development of a “social market”, which allows youngsters to borrow cigarettes from their peers, a process which differs from the purchase of cigarettes by older youngsters for young adolescents who are not allowed to buy cigarettes because of legislation [15].
4) A set of strategies showing that price-sensitive smokers seek different ways of getting cigarettes at a low price, which may decrease future cessation efforts [16]. The study conducted in the USA [16] is confirmed with a peculiar intensity in the UK by another study, the International Tobacco Control Four Country Survey (ITC-4) [17]. The latter paper reports a level of 15% purchase of cigarettes from low/untaxed source in UK at the first wave of the survey, increasing to 20% at the second wave 7 months later.
Moreover, this subgroup of smokers is less prone to making a cessation attempt than the smokers buying full-price cigarettes. It is interesting to note, among the authors, F.J. Chaloupka, who has been very enthusiastic about pricing policy.
An older report from 1994 emphasises the problem of the failure of smoking cessation among the poorer in society; the Health Education Authority has shown that while smoking has halved among the better off families in the UK since the 1970s, there has been no change among those on low incomes, with the paradox that the pricing policy makes them poorer [18].
CONCLUSION
The pricing policy has its limits, at least among subgroups of population, chiefly the socially deprived, who are precisely the major victims of smoking dependence, and have the greatest difficulties in quitting. Therefore, the result of increasing the price of tobacco is to increase the poverty of the most deprived [19].
In the most developed countries, where the necessary steps to improve tobacco control have reached the desired level, we are, and will be in the near future, confronted by a hard core of smokers who show great resistance to all resources available for help in smoking cessation [20]. Jarvis et al. [20] have evaluated for England, UK, the proportion of the hard core smokers to be 16%, rising from 5% in young smokers (aged 16–24 yrs) to 30% in those aged >65 yrs. Again, socioeconomic deprivation is identified as one factor in those belonging to this category. This category also contains a lot of chronic obstructive pulmonary disease (COPD) patients, who combine a long duration of smoking, a rather low socioeconomic status and heavier irreversible obstruction [21].
Therefore, the question of reaching, in the general population, much less than 20% smokers is not solved and we believe that, despite the urge for a general improvement in the level of education that should improve the situation, we should make more effort to help those attempting smoking cessation and consider with more attention special interventions that are targeted to the hard core smokers.
Lung physicians should be more involved, at least with an important part of the hard core smokers, often COPD patients. This view was expressed by Tonnesen et al. [22] in 2007; we are in total agreement with this recommendation, which is far for being largely applied among European pulmonologists.
Moreover, better knowledge is needed concerning addiction and the brain mechanisms that lead to initiation and dependence on smoking. Nicotine psychopharmacology is making rapid progress, because it illustrates the physiological mechanisms of attention, learning and pleasure, and perhaps depression, besides its addictive properties, thus becoming a tool for a more in-depth understanding of the fundamental processes of brain evolution with increasing age. Perhaps more lung physicians should be aware of the pioneering work that has been done by Henningfield et al. [23] in this field.
Of course the strategies required for hard core smokers imply more collaborative work with psychologists and psychiatrists, with a team approach being increasingly necessary.
Therefore, as many European countries still need a strong improvement in their tobacco control policies, all the European countries, even those with a high tobacco control scale score, should now increase their financial support for smoking cessation and give dependent smokers better access to medication and dedicated care, especially when they belong to the hard core category of smokers, which most often corresponds to the more socioeconomically deprived group of individuals.
Statement of interest
None declared.
{kind=link}
The evolution of smoking prevalence in Ireland over a 12-month moving trend ending in December 2007. The smoking prevalence within each group is shown. —: overall prevalence; ······: 15–18 yrs old; –·–·–·–·: 19–35 yrs old; - - - - -: 36–70 yrs old; -- -- --: >71 yrs old.
- © ERSJ Ltd
References









