Article Text

Abstract
Background: Little is known about the combination of different medications in chronic obstructive pulmonary disease (COPD). This study determined the cost effectiveness of adding salmeterol (S) or fluticasone/salmeterol (FS) to tiotropium (T) for COPD.
Methods: This concurrent, prospective, economic analysis was based on costs and health outcomes from a 52 week randomised study comparing: (1) T 18 µg once daily + placebo twice daily (TP group); (2) T 18 µg once daily + S 25 µg/puff, 2 puffs twice daily (TS group); and (3) T 18 µg once daily + FS 250/25 µg/puff, 2 puffs twice daily (TFS group). The incremental cost effectiveness ratios (ICERs) were defined as incremental cost per exacerbation avoided, and per additional quality adjusted life year (QALY) between treatments. A combination of imputation and bootstrapping was used to quantify uncertainty, and extensive sensitivity analyses were performed.
Results: The average patient in the TP group generated CAN$2678 in direct medical costs compared with $2801 (TS group) and $4042 (TFS group). The TS strategy was dominated by TP and TFS. Compared with TP, the TFS strategy resulted in ICERs of $6510 per exacerbation avoided, and $243 180 per QALY gained. In those with severe COPD, TS resulted in equal exacerbation rates and slightly lower costs compared with TP.
Conclusions: TFS had significantly better quality of life and fewer hospitalisations than patients treated with TP but these improvements in health outcomes were associated with increased costs. Neither TFS nor TS are economically attractive alternatives compared with monotherapy with T.
Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a progressive inflammatory process characterised by airflow limitation, resulting in distressing symptoms and frequent exacerbations.1 Given the high prevalence of COPD and its effect on physical functioning, the societal burden of this disease is very high, and with an aging population, disease burden will likely rise in the future.2 In Canada, COPD is the fourth and sixth most common cause of hospitalisation among men and women, respectively.3
There are a variety of treatment modalities for COPD that depend on the patient’s level of severity, including short and long acting anticholinergics, short and long acting β agonists, oral or inhaled corticosteroids, theophylline and oxygen.4 5 Several clinical trials have evaluated the efficacy of individual treatments compared with placebo or to each other.6–16 In addition, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations suggest that physicians consider adding a second bronchodilator treatment rather than prescribing high dose bronchodilator monotherapy to mitigate adverse effects.4 However, little is known about the combination of different classes of long acting bronchodilator medications in COPD. It is hypothesised that as different classes of drugs have different mechanisms of action, their combined usage might have additive or even synergistic effects4 17 The Optimal Therapy of COPD trial18 19 was a multicentre randomised, double blind, controlled clinical trial designed to compare the effect of 1 year of treatment of COPD with three treatment regimens: (1) tiotropium 18 µg once daily + placebo twice daily (TP group); (2) tiotropium 18 µg once daily + salmeterol 25 µg/puff, 2 puffs twice daily (TS group); and (3) tiotropium 18 µg once daily + fluticasone/salmeterol 250/25 µg/puff, 2 puffs twice daily (TFS group). The primary outcome of the study, the proportion of exacerbation free patients at the end of 1 year of follow-up, did not differ among the three treatment groups. However, there was a statistically significant difference in lung function, number of exacerbations requiring hospitalisations, total hospitalisations and quality of life in favour of the TFS group. As exacerbations and hospitalisations are an important source of resource utilisation and costs in COPD,2 these results suggest that combination therapy with tiotropium–fluticasone/salmeterol might be a favourable treatment alternative compared with tiotropium alone.
The Optimal Trial protocol included a concurrent prospective economic analysis. Data on both resource use and effectiveness outcomes were collected during the trial. The aim of this economic analysis was to compare healthcare utilisation and direct costs for the three different treatment groups. The specific objective of the present study was to determine whether the combination therapies tested in the OPTIMAL trial were cost effective alternatives to monotherapy with tiotropium, based on the incremental cost per exacerbation avoided.
METHODS
The present economic evaluation is based on an intention to treat analysis of the OPTIMAL trial from the perspective of the Canadian healthcare system. The main analysis focuses on the incremental cost per exacerbation avoided. The other outcome studied was the incremental cost per quality adjusted life year (QALY) gained. The time horizon of the analysis was 1 year, in line with the follow-up duration of the OPTIMAL study.
The design, patient recruitment, methods and results of the OPTIMAL trial have been described elsewhere.18 19 The study included 449 patients with moderate to severe COPD from 27 Canadian academic and community medical centres. To be enrolled, patients had to have experienced at least one exacerbation prompting medical intervention in the year preceding randomisation, have had a history of 10 pack-years or more of cigarette smoking and moderate or severe airflow obstruction defined as post-bronchodilator forced expiratory volume in 1 s (FEV1) <65% predicted. The primary outcome measure was the proportion of patients who experienced a respiratory exacerbation within 52 weeks of randomisation. Respiratory exacerbations were defined as a sustained worsening of patient’s respiratory condition, from the stable state and beyond normal day to day variations, necessitating use of oral or intravenous corticosteroids or antibiotics. The study was designed to detect an 18% risk difference with alpha = 0.05, and 80% power, and with the provision of 5% dropouts. Quality of life was assessed by SGRQ at baseline and at four follow-up visits, 4, 20, 36 and 52 weeks after randomisation.
Handling missing data
An important aspect of economic evaluations conducted alongside a clinical trial is how to deal with missing data due to attrition. In the OPTIMAL trial, 13.4% of patients had incomplete follow-up (excluding patients who died). Partially observed longitudinal data may introduce bias into the estimation of the costs and effectiveness20 and several rigorous approaches to rectify this issue have been described.21 22 We followed recommendations by Oostenbrink22 and Briggs and colleagues,23 and the International Society for Pharmacoeconomics and Outcomes Research,24 in dealing with missing cost and effectiveness data. We divided the whole follow-up period into discrete time intervals and used a combination of imputation and bootstrapping to quantify uncertainty caused by missing values and the finite study sample size. For each patient, the last period in which the patient had been followed was determined separately for costs and effectiveness outcomes. We used propensity scores, stratified by treatment group, for imputing the missing costs and effectiveness data caused by attrition.25 Covariates used to calculate the propensity scores were age, gender, study site, number of exacerbations in the preceding year, baseline FEV1 and the value of the missing variable in the preceding period.
Costs
Healthcare utilisation was systematically collected for each patient according to the study protocol. The major resource categories were the study drugs, exacerbation related medications, nursing and respiratory care visits at home, physician and emergency room visits, and hospital or ICU admissions. Among non-COPD related resource utilisation, only the number of hospitalisations for each patient was recorded. The base case analysis therefore considered only COPD related costs. Non-COPD related hospitalisation costs were included in the sensitivity analysis. Protocol driven costs such as the costs of prescheduled follow-up visits were excluded from the analysis.
A unit cost was assigned for each component of resource utilisation (table 1). The price of medications, including the study drugs and medications used to treat exacerbations, were based on the prices the provincial government reimburses under the drug coverage programme.26 All medications for exacerbations were recorded by drug name and duration, enabling the accurate calculation of costs for each patient. The daily cost of hospitalisation for COPD patients was taken from the fully allocated cost model of a tertiary care hospital in Vancouver. The cost of an emergency room visit for a COPD exacerbation was based on the report by Chapman and colleagues.27 All other unit costs were based on the fee-for-service rates of the British Columbia Medical Services Plan.28 All costs were inflated to 2006 Canadian dollars using the consumer price index reported by Statistics Canada.29 Because the period of data collection covered only 1 year, no discounting was necessary. The analysis was performed from the third party payer perspective, and no indirect medical costs or out-of-pocket costs were included.
Effectiveness outcomes
The total number of exacerbations and total QALYs were calculated for each treatment arm. Utilities were calculated from the SGRQ scores according to the algorithm published by Meguro.30 This algorithm divides each of the three domains of the SGRQ (symptoms, activity, and impact) into three levels and assigns a disutility weight for each level. For each patient at each time period, utility was calculated either from the SGRQ score at that time interval (if measured at that interval) or by linearly interpolating the SGRQ scores from the adjacent follow-up visits. The calculated QALYs were adjusted for the estimated baseline utilities using a linear regression model.31
Mortality
Sixteen patients died during the trial. Two deaths occurred between 12 months and 13 months after randomisation and these were not in the time horizon of this analysis. Among the remaining deaths, three were in the TP group, six in the TS group and five in the TSF group. By definition, all costs and utilities after death were set to zero. However, for exacerbation rate as the effectiveness outcome, setting zero costs and zero effectiveness after death would reward the treatment arm with excess mortality. Therefore, for this outcome, we treated the death events as attrition (forced dropout). Alternative scenarios regarding mortality were explored in the sensitivity analysis.
Cost effectiveness analysis
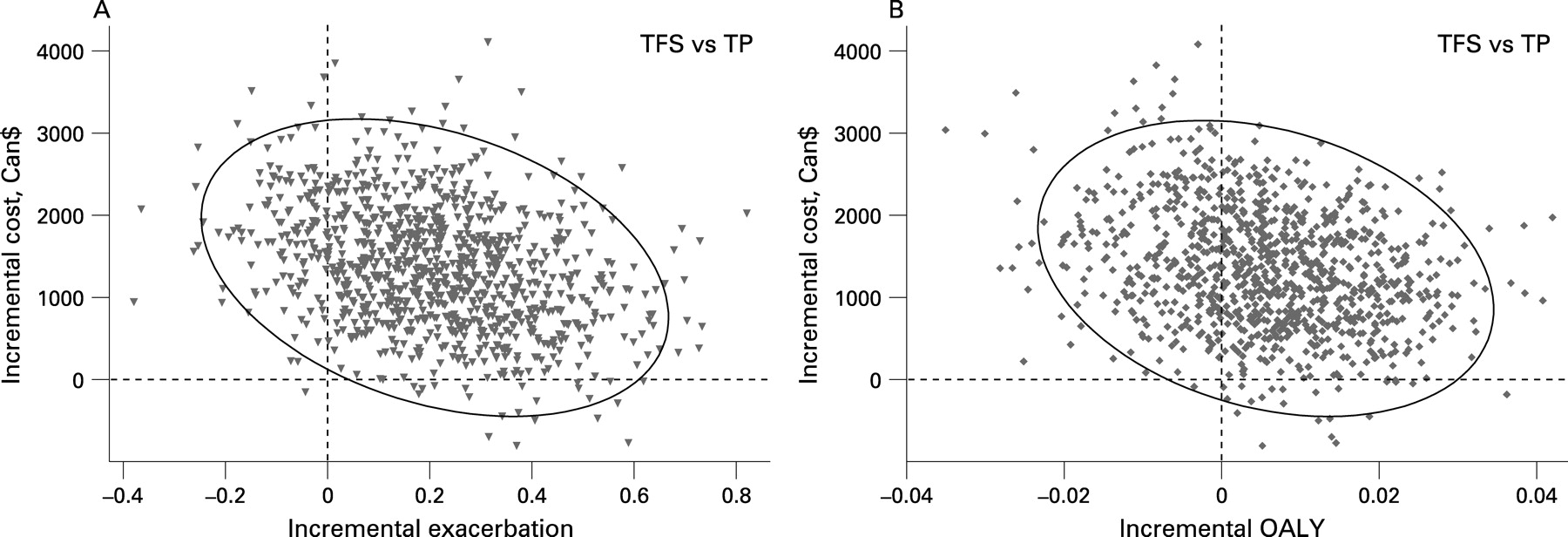
The incremental cost effectiveness ratio (ICER) was calculated for each effectiveness outcome, for TS and TFS versus TP and also for TFS versus TS groups. Uncertainty in the estimation of the costs and effectiveness were modelled by nested imputation and bootstrapping. In each cycle, the missing values were imputed and the complete dataset was bootstrapped within each treatment group. This method accounts for the uncertainty due to both the missing values and the finite study sample size. For each run of imputation and bootstrapping, we calculated (for each patient) the total cost, QALY and number of exacerbations. These outcomes were then averaged for patients within each treatment arm. The contribution of different cost components (MD/emergency department visits, hospital/ICU admission, study treatments and exacerbation medications) to total costs was also evaluated. Expected value (mean) of the cost and effectiveness outcomes along with their confidence intervals, plots on the cost effectiveness plane and cost effectiveness acceptability curves were generated based on 10 000 iterations of nested imputation/bootstrapping. Fiellers’ method was used to generate 95% confidence ellipses for the joint distribution of cost and effectiveness outcomes.32
Sensitivity analysis
Various assumptions and scenarios were evaluated in the one way sensitivity analyses. Firstly, we restricted the dataset to patients for whom all data on costs and effectiveness were available (complete case scenario). This would eliminate the uncertainty caused by missing values. However, as patients who do not complete their follow-up are often those with more severe disease, it was expected that the complete case analysis would underestimate costs and overestimate effectiveness outcomes. Another sensitivity analysis included non-COPD related hospitalisation costs. Daily costs of non-COPD related hospitalisation was modelled as equal to the average daily cost of hospital stay for surgery and medicine wards. Sensitivity analysis also included the calculation of outcomes in subgroups of patients defined by COPD severity (according to the GOLD criteria4). As the administration of SGRQ was performed on predetermined visits and often not during patients’ exacerbations, we felt that it might have failed to capture the effect of exacerbations in quality of life. Therefore, in another analysis, utility loss during exacerbations was modelled by lowering patients’ utilities by 15% and 50% during mild/moderate and severe exacerbations, respectively.33 34 Severe exacerbation was defined as one that requires hospitalisation. Finally, two alternative approaches in estimating exacerbations in those who died were evaluated in sensitivity analysis. In the first approach, it was assumed that if patients had survived, they would have no more exacerbations during the follow-up period. In the second approach, it was assumed that patients would have no more exacerbation free periods had they survived to the end of the follow-up.
RESULTS
Total costs, rate of exacerbation and QALYs stratified by each of the treatment arms, and the ICERs comparing non-dominated strategies with each other, are reported in table 2. When the exacerbation rate was the effectiveness outcome, the TS strategy was dominated by TP as it resulted in higher costs and a higher rate of exacerbations. The ICER for avoiding one exacerbation was $6510 for TFS compared with TP.
After adjusting QALYs for the baseline utilities in each group, the incremental QALYs of TS and TFS versus TP decreased from 0.0032 to −0.0052 and from 0.0125 to 0.0056, respectively, reflecting the lower utility at the start of the trial for the TP group. The 95% confidence intervals of the adjusted incremental QALYs for both TFS versus TP and TS versus TP crossed zero, indicating that the observed QALYs were not significantly different from that of the TP strategy for both alternative treatments. When the adjusted QALY was the health outcome, the TS was dominated compared with TP because of its higher costs and lower effectiveness. The ICER of TFS versus TP was $243 180 per one QALY gained.
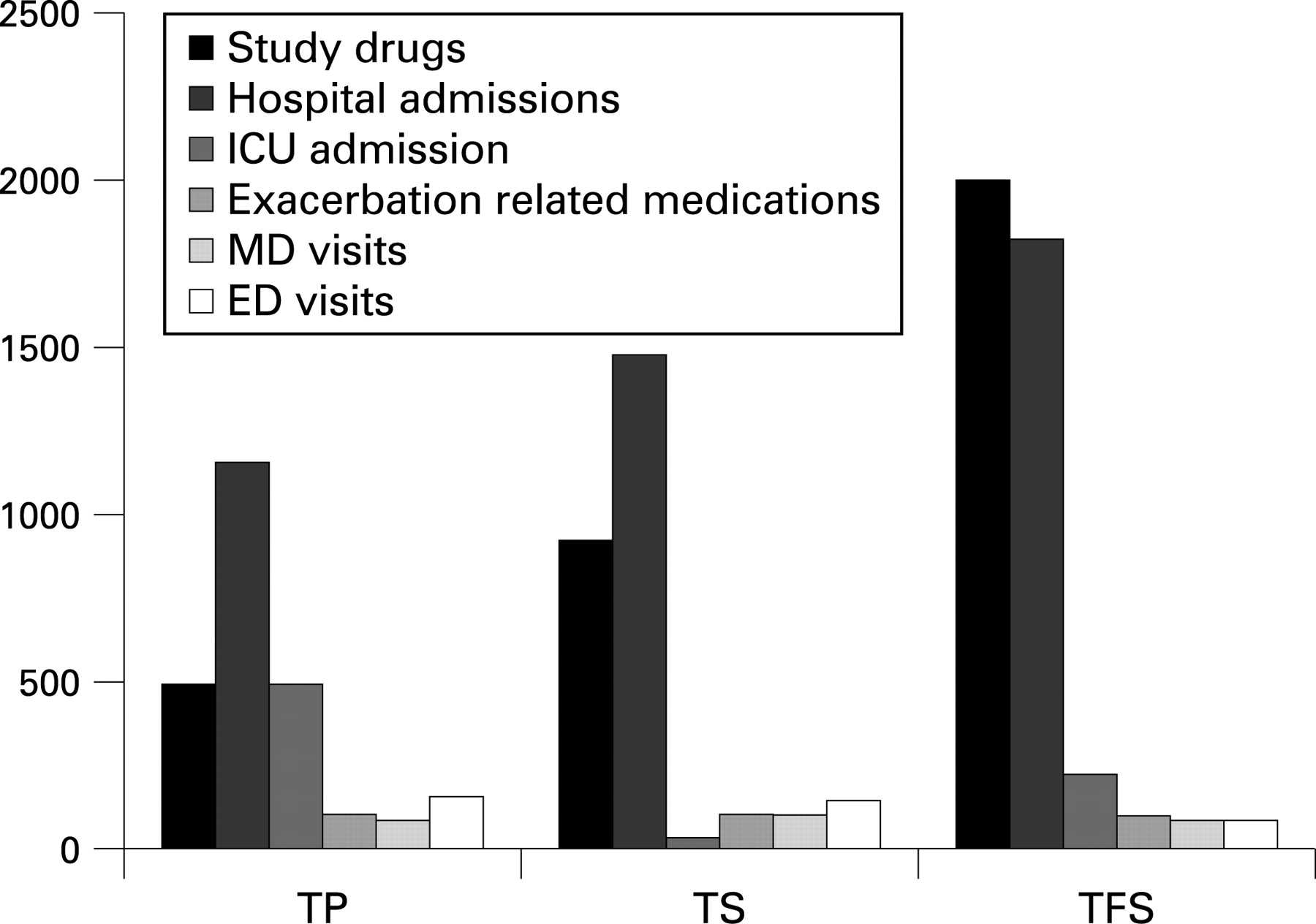
The cost components contributing to the overall COPD related costs in each group are shown in fig 1. Overall, the higher cost of study drugs in the TFS and TS groups was only partially offset by the lower costs in some other components (mainly ICU admissions and MD visits) compared with the TP group. Despite the fact that patients in the TFS group had significantly lower probability of hospitalisation, the total hospitalisation cost was higher in the TFS group. This was because of an extraordinary long length of stay for one patient in the TFS group who was hospitalised from day 36 until his death at day 251 (215 days of hospitalisation). When this patient was removed from the analysis, the COPD related hospitalisation costs reduced by $568 (to $1256) for the TFS group, and the ICER of TFS versus TP decreased to $3876 per one exacerbation avoided and $145 756 per QALY gained.

Sensitivity analysis
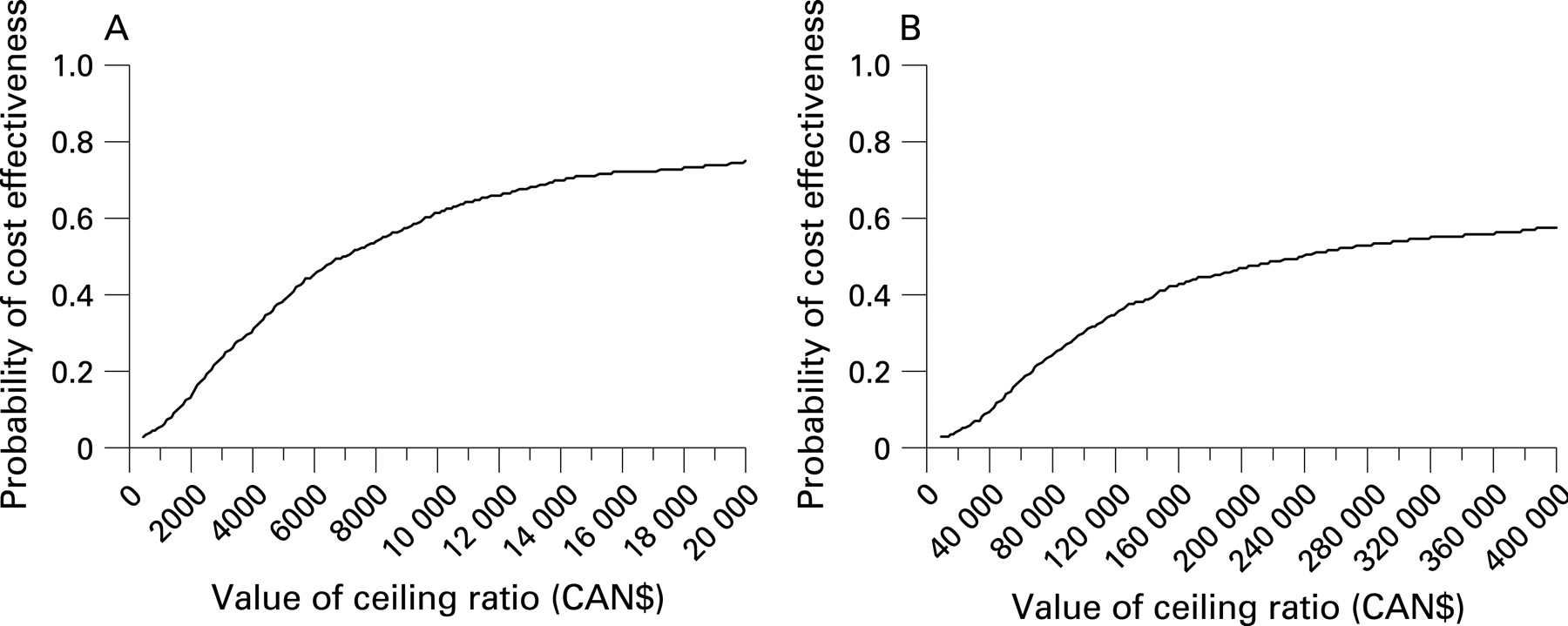
Since for both outcomes TS was dominated by TP, the TS strategy was dropped from further cost effectiveness analyses. Results of the bootstrap/imputation sensitivity analysis are shown in fig 2 (cost effectiveness plane) and fig 3 (cost effectiveness acceptability curve). For the willingness to pay of $6000 per exacerbation or less, treatment with tiotropium alone had the highest probability of being the most cost effective option. When QALYs were the effectiveness outcome, treatment with tiotropium alone had a higher probability of being the best option compared with the other treatments over the whole range of the willingness to pay values analysed ($Can 0–400 000). At the conventional value of $50 000 per QALY, monotherapy with tiotropium had an 80% probability of being the most cost effective strategy compared with the alternatives.

{kind=link}
{kind=link}
{kind=link}
Results of one way sensitivity analyses are presented in table 3. Results were generally robust to the different assumptions explored in the one way sensitivity analysis. Costs in the TS group fell slightly below the costs of the TP group when the data were limited to the complete cases, when non-COPD hospitalisations were included in the costs and in patients with severe COPD. The ICER per exacerbation avoided of TFS versus TP varied from a minimum of $3332 in complete case analysis to more than $47 000 when one exacerbation was assigned to each period after death.
DISCUSSION
Using data from a relatively large, multicentre clinical trial, this study showed that a combination of salmeterol or fluticasone/salmeterol with tiotropium did not seem to be cost effective. The incremental cost effectiveness ratio was more than $6000 for one exacerbation avoided when fluticasone/salmeterol was added to monotherapy with tiotropium. Similarly, the incremental cost effectiveness ratio was more than $200 000 per QALY gained when fluticasone/salmeterol was added to monotherapy with tiotropium. This is despite the fact that exacerbation rates were somewhat lower, and quality of life was significantly higher in the TSF group compared with the two other groups.
There is uncertainty in the findings. For instance, considering the QALY as the effectiveness outcome, and using the conventional effectiveness value of $50 000 per QALY, the probability that monotherapy with tiotropium is the most cost effective choice is 80%. As no other clinical trial has examined similar combinations of medications, we believe this is the only information available to the decision maker on choosing among the treatments examined here. This signifies the need for more studies evaluating the effectiveness of these treatment regimens in patients with COPD. It is also noteworthy that subgroup analyses revealed that treatment with TS was cost effective in patients with severe COPD. However, patients in this group had an equal rate of exacerbations with only slightly lower costs compared with patients in the TP group, causing considerable uncertainty in this finding.
An incremental cost per exacerbations avoided is somewhat more difficult to interpret than the incremental cost per QALY. In the absence of any studies that measure the willingness of society to pay for each exacerbation avoided, such ICERs can only be compared with similar figures in other cost effectiveness studies. Oostenbrink et al estimated the ICER of tiotropium over ipratropium to be €667 per exacerbation avoided,35 which is significantly lower than the ICERs for the same outcome in our study. In a 5 year decision analytic model of COPD, Rutten-van Mölken et al estimated the ICER of an exacerbation free month for tiotropium versus salmeterol and salmeterol versus ipratropium to be €360 and €1711, respectively.36 This value is also remarkably lower than the ICER for an exacerbation free period in our study.
The strength of this analysis includes prospective collection of data on both resource use and effectiveness outcomes, which should have minimised the bias that would result in retrospective data collection. The nested imputation and bootstrapping used in this analysis enabled full incorporation of the uncertainty resulting from missing values and limited sample size of the study.
There are some limitations of our analysis. Estimation of utility values was based on a disease specific questionnaire using a newly developed algorithm, which has not been independently validated. As the indirect costs (eg, productivity loss) were not systematically gathered in the OPTIMAL study, the cost effectiveness analysis could not be performed from a societal perspective, as recommended by several authorities37 38 However, productivity losses are likely to be minimal in this elderly population with advanced COPD, as the vast majority of these patients are no longer working. Among the non-COPD related resource utilisation, only hospitalisations were recorded. Deciding whether a particular event with its associated costs is COPD related or not could be difficult at times and the decision will inevitably be subjective to some extent, although such discretion was made by a physician blinded to the treatments.
Another shortcoming of this analysis, like the majority of economic evaluations conducted alongside clinical trials, is the difference in the management of patients in reality and in the carefully controlled setting of a clinical trial. For instance, patients in the OPTIMAL study received a specific recommendation on the usage of other COPD related medications and received regular follow-up visits. Such protocol specific management options might have had an impact on the observed resource utilisation and effectiveness outcomes. A good example, as discussed by Oostenbrink and colleagues,35 is the possibility that patients following prescheduled follow-up visits during a clinical trial might prefer not to initiate an unscheduled visit to another physician or healthcare facility for their complaints, and instead might seek treatment during their protocol driven visit. Therefore, the resource utilisation when protocol driven visits are excluded may underestimate the cost of physician visits that would have occurred in real life settings.
The 1 year time horizon of this study is in line with many other clinical trials and cost effectiveness studies in this field but decision makers might be interested in results over a longer time horizon. We chose not to extrapolate the results of this study beyond 1 year as there is little reason to believe that long term usage of these medications would change the order of their cost effectiveness as observed. There are some instances in which the cost effectiveness is strongly affected by the choice of the time horizon. For example, the ICER of lung volume reduction surgery versus medical therapy in the US was found to change from $190 000 to $53 000 per QALY at 3 and 10 years, respectively.39 Such dependency on the time horizon, in our belief, is mainly due to the difference in the pattern of costs over time between the two arms. In the lung reduction surgery arm, a significant portion of costs accumulates at the beginning and is diluted over time while costs of medical therapy tend to be constant throughout time. Here, costs and effectiveness outcomes in all three arms were accumulated at relatively steady rates and hence it is unlikely that the extrapolation of outcomes beyond the time horizon of the study will have any asymmetric effects on the treatment strategies.
In summary, although the OPTIMAL clinical trial demonstrated that patients treated with tioropium plus fluticasone/salmeterol had significantly better disease specific quality of life and fewer hospitalisations than patients treated with tiotropium plus placebo, these improvements in health outcomes were associated with increased costs. Increased costs associated with the medication more than offset the reduction in the costs of other healthcare resources. The results of this study suggest that among the three treatment options evaluated here, monotherapy with tiotropium appears to be the most economically attractive.
REFERENCES
Footnotes
Funding: This study was funded, in part, by the National Sanitarium Association, Ontario, Canada and the Canadian Institutes of Health Research (CIHR) through an operating grant for the clinical trial. CAM is funded by a Canada Research Chair in Pharmaceutical Outcomes and a Michael Smith Foundation for Health Research Scholar Award in Health Services Research. JMF is funded by a Michael Smith Foundation for Health Research Distinguished Scholar Award and a CIHR/BC Lung Association Investigator Award. SDA holds a CIHR New Investigator Award.
Competing interests: None.
Ethics approval: Ethics approval was obtained.