Article Text

Abstract
Background: A biologically plausible link between gastro-oesophageal reflux (GOR), aspiration, and lung allograft dysfunction has been suggested, but there is no systematic evidence indicating the presence of gastric contents in the lung. We have tested the hypothesis that pepsin, as a marker of aspiration, is detectable in bronchoalveolar lavage (BAL) fluid of allograft recipients who had not reported symptoms of GOR.
Methods: Standardised 3×60 ml surveillance BAL fluid samples from 13 chronologically sequential stable lung allograft recipients without chronic rejection (10 patients treated with a prophylactic proton pump inhibitor) were studied. Lavage supernatants were assayed by an ELISA based on a monospecific goat antibody for pepsin/pepsinogen. Pepsin levels were compared with those from four normal volunteer controls.
Results: Pepsin levels were measurable in all allograft recipients, in keeping with gastric aspiration (median 109 ng/ml (range 35–1375)). In the control group the pepsin levels were below the limit of detection. Treatment with a proton pump inhibitor was not correlated with pepsin levels. There was no correlation between BAL fluid neutrophils and pepsin levels.
Conclusion: These data demonstrate lung epithelial lining fluid concentrations of pepsin in lung allograft recipients which are much higher than blood reference levels, with no detectable pepsin in controls. This provides direct evidence of gastric aspiration, which is potentially injurious to the allograft.
- BAL, bronchoalveolar lavage
- GOR, gastro-oesophageal reflux
- TBB, transbronchial biopsy
- lung transplantation
- lung allograft
- gastro-oesophageal reflux
- pepsin
Statistics from Altmetric.com
Human lung transplantation is a well accepted therapeutic option for selected patients with advanced cardiopulmonary disease, but long term survival is limited by the development of obliterative bronchiolitis, the physiological hallmark of which is the bronchiolitis obliterans syndrome.1 The pathophysiology of obliterative bronchiolitis is poorly understood, but it is increasingly recognised to represent immunological and non-immunological mechanisms and an aberrant response to injury.1,2
Gastro-oesophageal reflux (GOR) has been implicated as a possible cause of non-immunological allograft injury.3 Allograft recipients have a number of risk factors for GOR. Lung allograft surgery causes significant damage to vagal innervation of the gastrointestinal tract and the immunosuppressant drugs cyclosporin and tacrolimus reduce gastric motility.4 In addition, cough reflexes and mucociliary clearance, the normal defence mechanisms against aspiration, are attenuated.5 All the above make reflux more likely, which is why many allograft recipients are given prophylactic acid suppression treatment.
Despite a high clinical suspicion regarding GOR in lung allografts, the literature is small and largely retrospective. However, formal oesophageal pH studies, when carried out, do indicate that GOR may be a significant problem in lung allografts and fundoplication surgery is associated with improved allograft function.6
We are unaware of any literature to date indicating gastric aspiration into the lung, and we have therefore tested the hypothesis that pepsin—as a marker of aspiration—is detectable in the lungs of allograft recipients who do not present with obvious symptoms of GOR.
METHODS
The study was approved by the local research ethics committees for Newcastle and North Tyneside, with separate applications for prospective studies in lung allografts and normal volunteer controls.
Following informed consent, 13 chronologically sequential unselected subjects undergoing either routine or symptom driven transbronchial biopsy (TBB) and bronchoalveolar lavage (BAL) were recruited (table 1), with the research sample intercalated within this procedure. Research samples were taken at least 1 month after any preceding bronchoscopic procedure and in the absence of any clinical evidence of prior microaspiration. All patients were receiving a standard long term maintenance regimen of immunosuppressive therapy comprising cyclosporin, azathioprine and prednisolone. The patients were not formally investigated for GOR, but did not report symptoms suggestive of GOR. In particular, there were no reports of heartburn, stomach ache, sour taste in the mouth, or pain on swallowing. Ten patients were treated with a prophylactic proton pump inhibitor, which is a common empirical treatment in this patient population.
Summary of patient demographic data, BAL and pathological rejection assessments
Four normal non-smoking controls (one woman, median age 39, range 32–46) were recruited from volunteer hospital staff for a research BAL. These subjects were recruited 9 months after the transplant patients, as soon as full ethical approval had been gained for bronchoscopic investigations in normal volunteers.
Bronchoscopy, BAL, and TBB
Bronchoscopy was carried out in accordance with published guidelines.7 Subjects were premedicated with intravenous midazolam. 4% lignocaine was applied topically to the nose, pharynx, and larynx and below the cords in 1 ml aliquots, as required, up to a maximum dose of 8 mg/kg body weight. Bronchoscopy was carried out with patients in a semi-reclined position.
Bronchoalveolar lavage was standardised to a 3×60 ml procedure with oxygen saturation routinely measured during the procedure. The BAL fluid sample was split and assessed for clinical microbiology and differential cell counts on Giemsa stained cytocentrifuge preparations. Cell free BAL supernatants were prepared by centrifugation (10 minutes, 1500 rpm, 10 minutes), aliquots snap frozen by immersion in liquid N2, and stored at −80°C prior to ELISA.
Transbronchial biopsies were obtained from allograft patients only.
Pepsin/pepsinogen ELISA
A locally developed ELISA was performed using 100 μl of unconcentrated BAL supernatants. The assay, based on a monospecific antibody to porcine pepsin, measured both pepsin and total pepsinogens, referred to henceforth as “pepsin”, with a lower limit of detection of <1 ng/ml.8,9 All assays were performed by one individual and the coefficient of variation for the assay was 13%. Serum reference levels for pepsin are 49.8–86.6 μg/l).8 The ELISA on the samples from normal subjects were performed 9 months after the transplant patients.
Processing of TBB samples
Five to seven TBB samples were taken at each allograft bronchoscopy, fixed in 10% formalin, embedded in paraffin, and stained with haematoxylin and eosin to assess acute or chronic rejection according to standard criteria.10
Statistical analysis
Non-parametric methods were used throughout using Minitab statistical software. The median pepsin levels in allograft recipients were compared with those in control subjects by the Mann-Whitney U test (two tailed).
RESULTS
Patient demographic data, BAL and pathological rejection assessments are summarised in table 1. Five of the 13 subjects had clinically significant mild to moderate (a2) acute rejection, but all were free from long term irreversible loss of lung function.
BAL fluid data
The median BAL return was 90 ml (range 55–100) in allograft recipients and 80 ml (range 55–90) in controls, indicating technically satisfactory procedures. As in our previously published data on allograft patients, the percentage of neutrophils in the BAL fluid of allograft recipients was variable (median 2.0% (range 0.2–35.6)) and higher than our normal range (1.6% (range 0–2), p = 0.03).11
BAL fluid pepsin levels
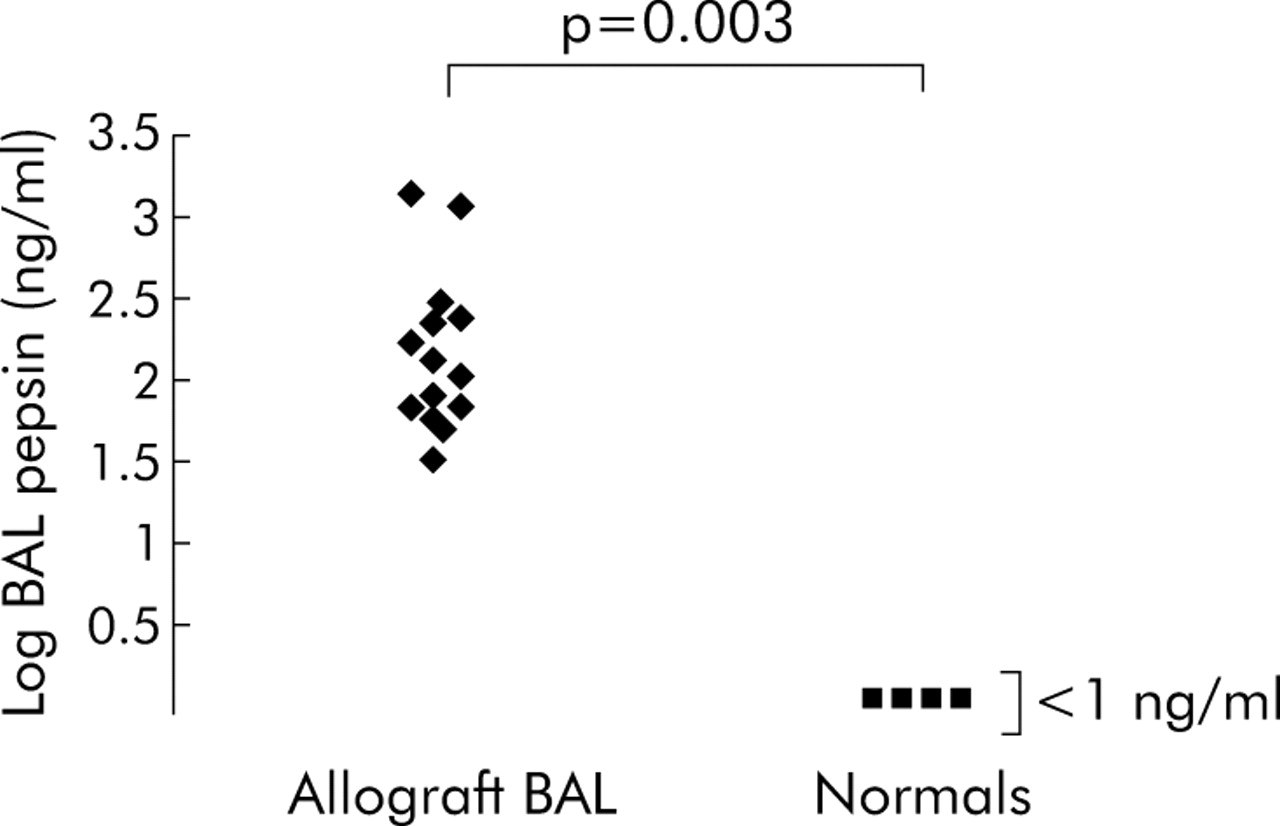
Pepsin levels were measurable in all BAL fluid samples from allograft recipients (fig 1), suggesting gastric aspiration (median 109 ng/ml (range 35–1375)). In the control group pepsin levels were below the limit of detection (<1 ng/ml). Treatment with a maintenance dose of proton pump inhibitor did not correlate with pepsin levels. There were no correlations between BAL neutrophils, acute rejection, and pepsin levels.

{kind=link}
BAL fluid pepsin levels in allograft recipients and controls.
DISCUSSION
Limited previous reports, largely retrospective but some with formal objective oesophageal pH monitoring, have suggested that GOR is a significant problem in lung allograft recipients,6 and treatment of GOR has been cited as a new therapeutic option to treat patients with the bronchiolitis obliterans syndrome.12
In this study we have shown that high and variable levels of pepsin are detectable in BAL fluid of allograft recipients, with no pepsin detected in normal control BAL fluid samples. To our knowledge, this is the first systematic direct evidence of gastric aspiration into lung allografts. This may be a continuing and cumulative potential injury to allografts, and we provide mechanistic support for this contention.
Absolute determination of the dilution of the pericellular epithelial lining fluid (ELF) sampled by BAL is not possible,13 but estimations are practicable, based on the morphometric data of Weibel (cited by Widdicombe14). These considerations suggest that our BAL procedure represents a dilution of approximately 1 in 200 of the ELF sampled, with our present data consistent with ELF concentrations of pepsin 10–103 times higher than serum reference levels.8 In contrast, our published data on BAL fluid levels of albumin in allografts are consistent with ELF levels substantially lower than those found in serum.15 Overall, our data indicate a gastric source of the pepsin detected.
Pepsin is a proteolytic enzyme, active at acidic pH. There are no data of which we are aware regarding the pH of allograft ELF, but acidic breath condensate is increasingly reported as a marker of inflammation in asthma, chronic obstructive pulmonary disease, bronchiectasis, cystic fibrosis, and following cardiothoracic surgery.16 These pH levels are consistent with potential proteolytic activity for pepsin. Aspiration of gastric contents into the lung would be anticipated to cause epithelial damage in allografts, stimulation of cytokine production, and an airway inflammatory/remodelling response, potentially contributing to irreversible loss of allograft function and eventual failure.1,2
It was noteworthy that most of the patients we studied were being treated with a prophylactic proton pump inhibitor at a low maintenance dose. This reflects widespread empirical use in allograft recipients in view of concurrent oral corticosteroid use and their role in patients with cystic fibrosis to prevent pancreatic enzyme supplement degradation. Such medication would be expected to suppress symptoms associated with GOR caused by acid, but a potential concern highlighted by our study is that “clinically occult” aspiration of other gastric contents would still be possible.
Our study, though novel, is preliminary and our control information is limited. However, we specifically adopted a rigorous approach to this by recruiting normal volunteers, and no pepsin was detected in these controls. Our results therefore indicate the presence of unexpectedly high, potentially deleterious levels of pepsin in lung allografts. This may be significant, irrespective of aetiology, with lung allografts singularly vulnerable to injury.1,2 Longitudinal studies are now required to assess whether the presence of BAL pepsin and other markers of GOR are related to long term allograft failure and chronic rejection, and such techniques may be broadly useful in studying other patients with GOR who develop lung disease.
REFERENCES
Footnotes
-
Published Online First 29 July 2005
-
This study was funded by the Freeman Hospital and University trustees, the European Respiratory Society, and the Medical Research Council
-
Competing interests: none declared