Article Text

Abstract
Background Respiratory failure is a life-threatening and unpredictable complication of systemic sclerosis (SSc). A study was undertaken to assess the value of alveolar nitric oxide (NO) in predicting the risk of lung function deterioration leading to respiratory failure or death in patients with SSc.
Methods 105 patients with SSc were enrolled in this prospective cohort and were followed longitudinally over a 3-year period during which the risk of occurrence of deleterious events was analysed according to alveolar concentration (CAno), conducting airway output (J′awno) and fractional concentration (FEno0.05) of exhaled NO measured at inclusion. Comparison was made between each NO parameter to predict the occurrence of deleterious events, defined as a 10% decrease in total lung capacity or forced vital capacity from baseline, or death.
Results The area under the receiver operating characteristic curve of CAno to predict the occurrence of the combined events was 0.84 (95% CI 0.76 to 0.92; p<0.001), which was significantly higher than those of J′awno and FEno0.05 (p<0.001). A cut-off of CAno of 5.3 ppb had a sensitivity of 88% and a specificity of 62% for the prediction of the occurrence of combined events during follow-up, and was validated in an independent cohort of patients with SSc. Combined events occurred more frequently in patients whose CAno was >5.3 ppb. The adjusted HR for patients with CAno >5.3 ppb was 6.06 (95% CI 2.36 to 15.53; p<0.001). CAno accurately predicted the occurrence of combined events irrespective of forced vital capacity values or the presence of interstitial lung disease at baseline.
Conclusions Increased CAno accurately identifies patients with SSc with a high risk of developing lung function deterioration and may help to initiate early appropriate treatment.
- Alveolar concentration of nitric oxide
- systemic sclerosis
- interstitial lung disease
- exhaled nitric oxide
- prognostic factor
- exhaled airway markers
- interstitial fibrosis
- lymphocyte biology
- COPD epidemiology
- interstitial fibrosis
- sleep apnoea
- systemic disease and lungs
Statistics from Altmetric.com
- Alveolar concentration of nitric oxide
- systemic sclerosis
- interstitial lung disease
- exhaled nitric oxide
- prognostic factor
- exhaled airway markers
- interstitial fibrosis
- lymphocyte biology
- COPD epidemiology
- interstitial fibrosis
- sleep apnoea
- systemic disease and lungs
Key messages
What is the key question?
Identification of progressive form of scleroderma lung disease by nitric oxide (NO) exhaled marker
What is the bottom line?
Elevated Alveolar concentration of NO (CANO) is valuable marker in predicting the risk of subsequent lung function deterioration or death in patients with scleroderma.
Why read on?
CANO cut-off is validated, as predictive marker of progressive form of scleroderma lung disease in an independent cohort, which allows clinician initiating appropriate treatment in early phase of disease.
Introduction
Systemic sclerosis (SSc) is a connective tissue disease characterised by immune activation, vascular damage and fibrosis of various organs including the skin, gastrointestinal tract, kidneys and lungs.1 Interstitial lung disease (ILD), an unpredictable and life-threatening condition that occurs in more than half of patients,2 is the main cause of death in SSc.3 ILD related to SSc (SSc-ILD) gradually and irreversibly decreases lung volumes, impairs lung gas exchanges and reduces walking distance. As a result, quality of life and daily activities are markedly impaired in most patients, and death eventually occurs in those with the most severe form of the disease.2 4 Annual pulmonary function tests (PFTs) are recommended to detect lung function worsening, which is considered a critical turning point in the natural course of SSc-ILD.5
The current hypothesis regarding the pathogenesis of SSc-ILD suggests the occurrence(s) of pulmonary injuries initiated by unknown factor(s) followed by cryptic but sustained and incompletely resolved autoimmune alveolitis that eventually results in pulmonary fibrosis.6 Immunosuppressive agents only have minor beneficial effects to slow down the rate of lung function decline of patients with SSc in whom it is impossible to restore lung volumes to normal.7 8 There is an urgent need to find biomarkers capable of identifying patients whose lung function might deteriorate dramatically and rapidly and who will consequently benefit from timely and effective treatment.
Alveolar inflammation, which releases proinflammatory cytokines into the bloodstream and nitric oxide (NO) into the exhaled air,9 10 is the main monitoring option for ILD. NO, a key intercellular and intracellular mediator, is both a powerful endogenous vasodilator and a highly reactive biomarker of inflammation. In patients with SSc, inducible NO synthase is abundantly expressed in inflamed lung tissue, thus favouring excessive synthesis of NO and its resulting increased concentration in the exhaled air of patients with SSc-ILD.11 Using a partitioned exhaled NO model12 that splits fractional exhaled NO (FEno) into airway conducting maximal NO output (J′awno) and alveolar concentration of NO (CAno)—reflecting the underlying bronchi and alveolar inflammation—we and others13 have previously shown that increased CAno levels are related to the importance of SSc-ILD in vivo14 and the ability of the serum from patients with SSc to induce fibrosis in vitro.15 However, the relationship between exhaled NO output and subsequent occurrence of lung function deterioration or death has not yet been studied in patients with SSc. We hypothesised that partitioned measurement of exhaled NO, enabling assessment of fractioned exhaled NO at 50 ml/s of outflow (FEno0.05) and calculation of J′awno and CAno, might help to estimate the risk of developing subsequent lung function deterioration or death in patients with SSc. A prospective cohort study was therefore conducted to assess the predictive power of FEno0.05, J′awno and CAno to predict lung function deterioration or death in patients with SSc.
Methods
Study design
Enrolment was conducted from November 2004 to May 2007 in the Department of Internal Medicine, Hospital Saint Antoine, Paris, France, and the follow-up of this time to event driven study ended in May 2010.
Inclusion criteria
Patients were considered for inclusion if they were aged >18 years and had a diagnosis of SSc16 with diffuse or limited forms,17 the presence of ILD diagnosed by chest high-resolution computed tomography (HRCT) and the presence of pulmonary hypertension (PH) ascertained by right heart catheterisation (RHC), irrespective of the level of forced vital capacity (FVC) and lung transfer factor for carbon monoxide (Tlco). Patients treated with corticosteroids and immunosuppressive agents were also eligible and recorded as presence of immunosuppressive therapy.
Exclusion criteria
Exclusion criteria were the presence of recent airway upper tract infection or pneumonia in the previous 3 months, the presence of lung cancer, asthma, allergic rhinitis, chronic obstructive pulmonary disease and treatment by NO donors. Patients who were unable to perform partitioned exhaled NO were also excluded.
Study design
At the start of the study, demographic data, duration of disease (delay between first symptom attributable to SSc and inclusion date), subset of SSc and history of smoking were recorded. All patients underwent extended NO analysis, PFTs, chest HRCT scanning and an echocardiogram. PFTs were routinely performed with a standard methodology and quality controls according to the American Thoracic Society and the European Respiratory Society (ATS/ERS) recommendations.18 ILD related to SSc was determined by the presence of reticular or ground glass changes extending at least to the venous confluence on the chest HRCT scan according to the ATS/ERS consensus19 and recorded as presence of ILD. Systolic pulmonary artery pressure was first estimated by echocardiography. All patients with >40 mm Hg subsequently underwent RHC. PH was confirmed as mean pulmonary artery ≥25 mm Hg according to ATS/ERS consensus20 and recorded as presence of PH.
Partitioned exhaled NO measurement
Briefly, fractional exhaled NO (FEno) was measured using a chemiluminescent analyser (EndoNO 8000, SERES, Aix-en-Provence, France) according to the ATS/ERS recommendations.21 After a full inspiration of room air, the subject exhaled against a positive pressure to generate exhalation flow rates (V′E) of 50, 100, 150 and 200 ml/s. For each V′E, the elimination rate of NO (V′NO) was calculated as a function of V′E (V′NO = V′E × FEno). At a flow rate of >50 ml/s, this relationship is linear and can be expressed as V′NO = V′E × FEno = CAno × V′E + J′awno.12 22 J′awno is the maximal conducting airway flux of NO.
Endpoint
The endpoint was the occurrence of combined deleterious events, defined as a 10% decrease in total lung capacity or FVC from baseline, or death.2 Survival status was obtained from visits and telephone interviews. Patients not seen within 3 months were called to confirm their living status. Patients were evaluated by PFTs, chest HRCT and echocardiography annually (or earlier in an additional visit if symptoms required).
Confirmation study in an independent population
To validate the prediction power of extended NO analysis for lung function deterioration or death in SSc, we performed a confirmation study involving patients with SSc enrolled in the same inclusion protocol from September 2006 to September 2007 in the Department of Rheumatology (Cochin Hospital, Paris, France) and followed up over 3 years to determine the occurrence of combined events.
Statistical analysis
We first assessed the diagnostic performance of CAno, J′awno and FEno0.05 for identifying patients with SSc who were going to have subsequent worsening of their lung disease or were going to die within the 3 years after inclusion (positive if combined events occurred within 3 years of follow-up and negative if combined events did not occur) using receiver operating characteristic curves (ROC) analysis. We compared their performances with each other using the method described by DeLong et al.23
We next determined the threshold of the best parameter that was able to predict the subsequent occurrence of combined events in the 3 years after inclusion based on Youden's index (maximal sum of sensitivity + specificity). To ensure the relevance of the predicted cut-off of the extended NO analysis for subsequent lung function deterioration or death within 3 years after inclusion, a confirmation study was performed in an independent cohort of patients with SSc from Cochin Hospital (figure 1). Continuous and categorical variables were presented as mean±SD and percentages and were compared between groups by two-sample t tests and χ2 tests, respectively.

Details of enrolment and flow of patients through study. CAno, alveolar concentration of nitric oxide.
We divided the studied population into two groups according to the best threshold to predict the subsequent occurrence of combined events of each exhaled NO parameter (FEno0.05, J′awno and CAno) at baseline. To estimate the predictive value of exhaled NO parameters on lung function outcomes during the whole follow-up period, cumulative risks were computed by Kaplan–Meier analysis. ORs for lung function deterioration over time according to NO measurements were estimated by the Cox proportional hazard model. For all parameters, the conformity with the proportional hazards assumption was tested by linear regression of Schoenfeld residuals on the time variable in observations with event=1. For categorical parameters, the conformity with the proportional hazards assumption was verified graphically in addition to construction of Kaplan–Meier curves. Only parameters fulfilling the proportional hazards assumption were used in the Cox analysis.
We first conducted unadjusted Cox analyses according to each baseline characteristic separately. In these models, NO variables were set as continuous variables. For any NO variable significant in this procedure, an additional unadjusted model was performed with a categorical two-level NO variable according to the corresponding optimal threshold in ROC curves. A multivariable Cox model further adjusted the categorical NO variable for age, FVC, Tlco and duration of disease as continuous variables and gender, smoking status, form of disease, the presence of ILD, PH diagnosed by RHC and immunosuppressive therapy as categorical variables.
We then assessed the relationship between change in FVC and variation of exhaled NO parameters between baseline and the last visit using a linear regression model. All tests were two-sided with a significance level of 5%. All analyses were performed with STATA Statistical Software Release 10 (Stata Corporation, College Station, Texas, USA).
Results
Baseline characteristics of population
One hundred and nine patients with SSc were eligible for this prospective study. Four patients were excluded (two with pneumonia, one with bronchitis and one with sigmoiditis; figure 1). One hundred and five patients were therefore consecutively included in the study (table 1).
Baseline characteristics of studied population and population for external validation of CAno threshold
The mean age of the patients at inclusion was 54.8±12.9 years and 13 (12.4%) were men. One-third of the patients had the diffuse form of SSc and half of the patients had ILD. Seventeen of the 105 patients (16.2%) took immunosuppressive agents (cyclophosphamide, n=1; mycophenolate mofetil, n=1; corticosteroids, n=15). After a mean follow-up of 36.3±17.2 months, five patients with SSc died from end-stage lung fibrosis, 34 had lung function deterioration, 66 were censored and no patient was lost to follow-up. The composite events, defined as death or a decrease of 10% in total lung capacity or FVC, occurred in 39 patients (37%). Three new cases of ILD were diagnosed by chest HRCT during the follow-up period.
A comparison of the characteristics of the studied population and those of the population used for external validation is shown in table 1 and figure 1. At baseline the mean duration of disease and the rate of smokers were higher in the study group of patients than in the external validation group of patients with SSc.
Prediction power of FEno0.05, J′awno and CAno for occurrence of combined events during 3 years after start of study
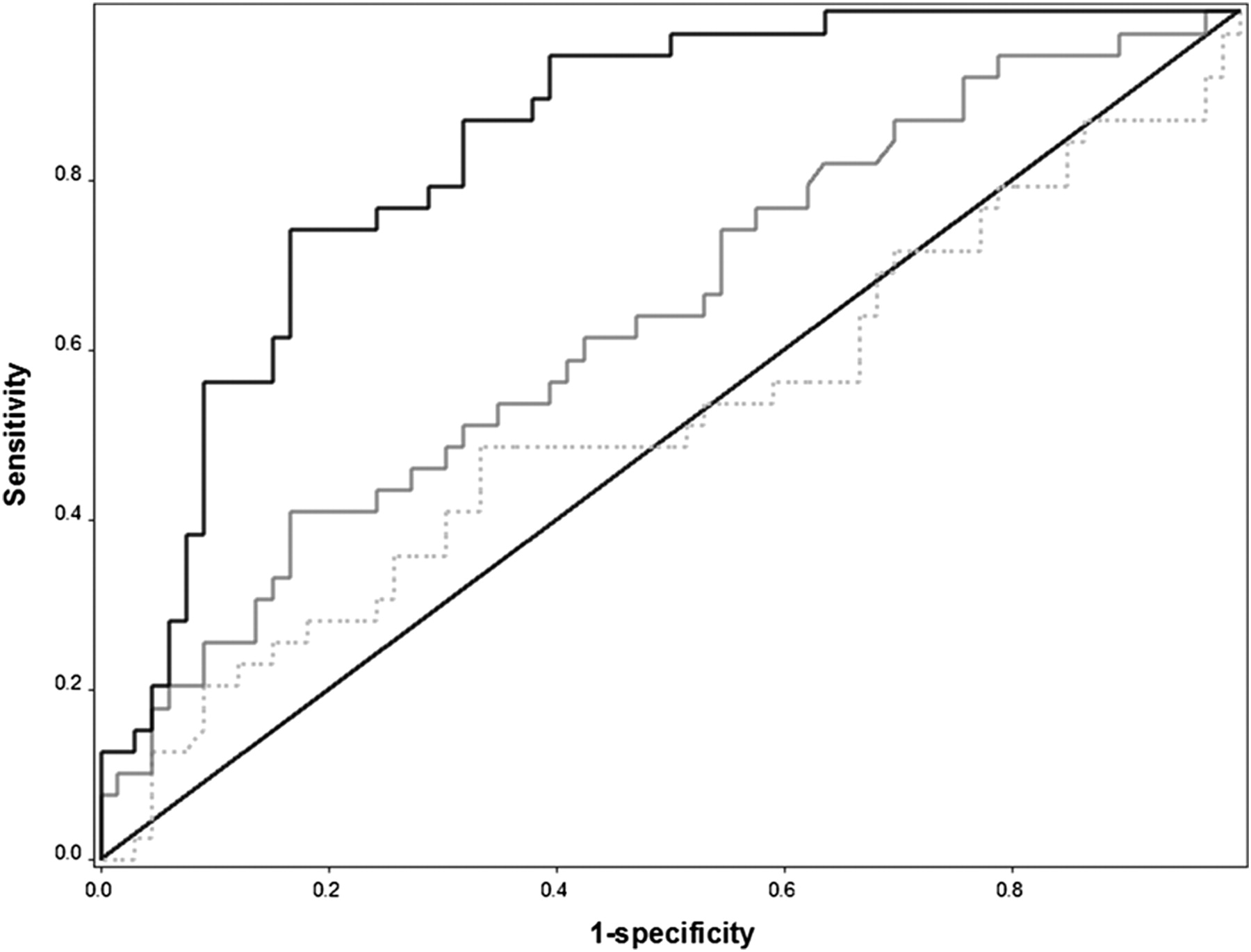
The area under the ROC curve (AUROC) of FEno0.05, J′awno and CAno for prediction of occurrence of combined events during the 3 years after inclusion in the study were significantly different from one another (p<0.001, figure 2). The AUROC of CAno for predicting the occurrence of combined events was 0.84 (95% CI 0.76 to 0.92; p<0.001) while the AUROC of FEno0.05 was significantly lower (0.64, 95% CI 0.53 to 0.75; p=0.007). In contrast, J′awno had no value for predicting the occurrence of combined events (AUROC=0.52, 95% CI 0.40 to 0.64; p=0.194). Moreover, the AUROC curve of CAno for predicting the occurrence of combined events during the 3 years after inclusion in patients from Cochin Hospital (0.83 (95% CI 0.75 to 0.92); p<0.001) was comparable with that in patients from Saint Antoine Hospital. Among the exhaled NO parameters, CAno had the best performance power. We therefore determined the best cut-off of CAno for predicting the combined events during the 3 years after inclusion and compared the risk of developing worsening lung function or dying during the whole follow-up with patients with SSc with CAno higher than this latter cut-off and the remaining patients.
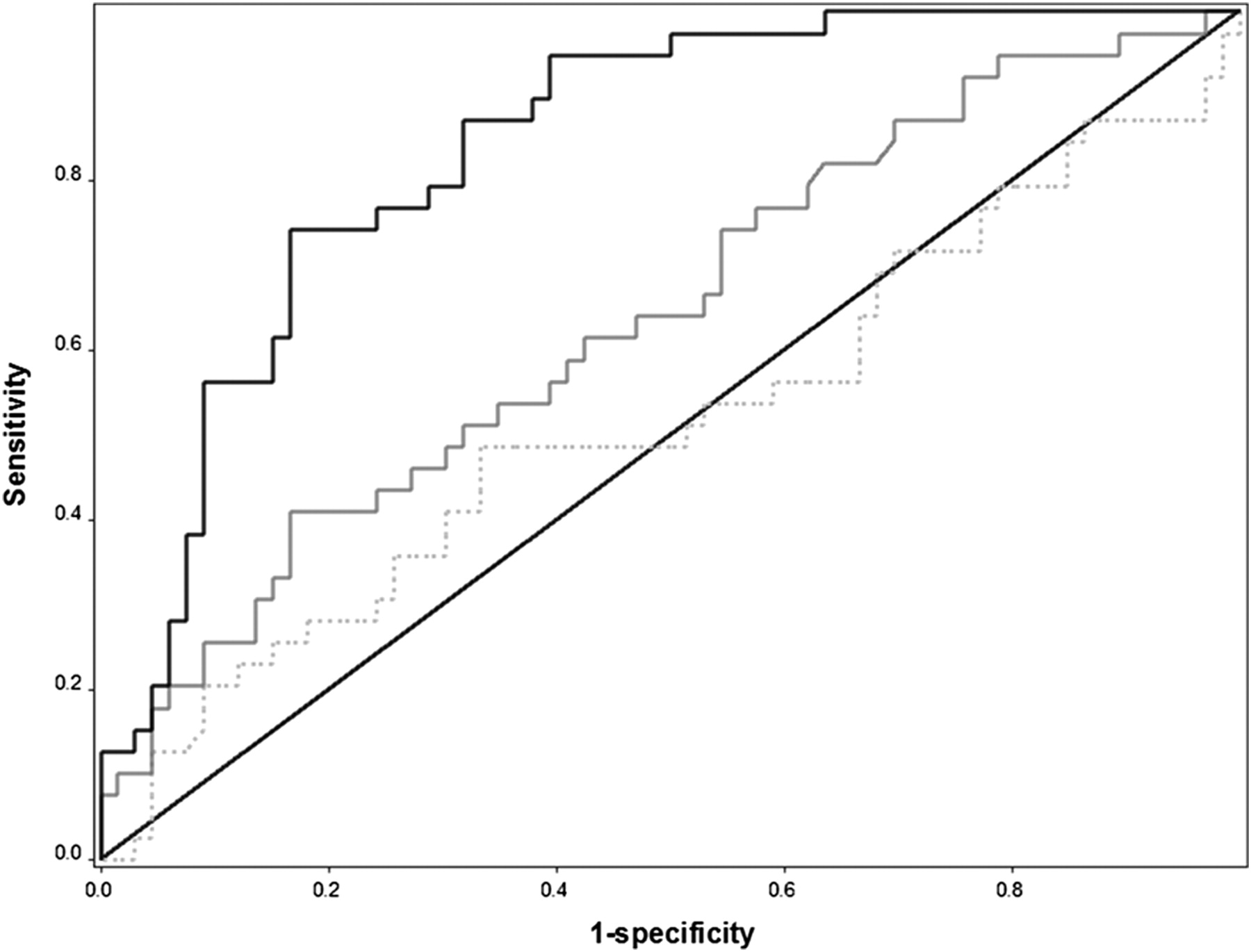
Performance of alveolar concentration of nitric oxide (CAno), conducting airways output of nitric oxide (J′awno) and fractional exhaled concentration of nitric oxide at 50 ml/min of outflow (FEno0.05) for predicting lung function deterioration or death 3 years after inclusion in the study. The black line represents the receiver operating characteristic (ROC) curve of CAno with an area under the curve of 0.84 (95% CI 0.76 to 0.92; p<0.001), the grey line represents the ROC curve of FENO0.05 with an area under the curve of 0.64 (95% CI 0.53 to 0.75; p=0.007) and the dotted grey line represents J′awno with an area under the curve of 0.52 (95% CI 0.40 to 0.64; p=0.194). The difference between the three areas under the ROC curves was statistically significantly (p<0.001).
Threshold of CAno to identify patients with SSc at risk of deterioration of lung disease or death during the 3 years after inclusion
The best cut-off of CAno for identifying deterioration in lung disease within 3 years was 5.3 ppb (95% CI 3.4 to 7.4). The sensitivity (Se), specificity (Sp), positive and negative predictive values (PPV and NPV) were 0.88 (95% CI 0.74 to 0.96), 0.62 (95% CI 0.49 to 0.74), 0.61 (95% CI 0.47 to 0.73) and 0.89 (95% CI 0.75 to 0.96), respectively compared with values of Se, Sp, PPV and NPV were 0.80 (95% CI 0.52 to 0.96), 0.61 (95% CI 0.42 to 0.77), 0.50 (95% CI 0.27 to 0.69) and 0.87 (95% CI 0.66 to 0.80), respectively, in the validation population. Se and Sp obtained in the validation study with 5.3 ppb as cut-off were very close to those observed in the studied population, confirming the robustness of CAno as a predictor of deteriorating lung function or death occurring during the 3 years after inclusion. The CAno threshold with 90% specificity for identifying subsequent deterioration of lung disease within 3 years was 8.5 ppb. Se and Sp obtained in the validation study with 8.5 ppb (Se=0.53, 95% CI 0.27 to 0.79; Sp=0.85, 95% CI 0.68 to 0.95) were also very close to those observed in the studied population (Se=0.56, 95% CI 0.40 to 0.72; Sp=0.91, 95% CI 0.81 to 0.96).
Association between CAno, FEno0.05 and J′awno at baseline and subsequent deterioration in lung function or death in patients with SSc
In an unadjusted Cox model, CAno had a predictive value for the occurrence of combined events (p<0.001) but FEno0.05 (p=0.061) and J′awno (p=0.762) did not (table 2).
Unadjusted Cox HRs for deterioration in lung function over time according to each baseline characteristic
In the Cox proportional hazards model adjusted for age, gender, smoking status, form of disease, duration of disease, presence of ILD, FVC, Tlco, presence of PH diagnosed by RHC and immunosuppressive therapy, patients with CAno >5.3 ppb had a higher risk of subsequent occurrence of combined events (HR 6.06, 95% CI 2.36 to 15.53; p<0.001). The adjusted HR for subsequent combined event occurrence in patients with CAno >8.5 ppb was 3.06 (95% CI 1.43 to 6.55; p=0.004).
Although the level of Tlco might in theory affect CAno values, it had a low impact on the ability of CAno to predict lung function deterioration or death related to lung fibrosis. Indeed, CAno was still an accurate predictive factor for the combined event in both patients with Tlco <60% of the predicted value and those with Tlco ≥60% of the predicted value. In patients with SSc with Tlco <60% of the predicted value the HR was 17.35 (95% CI 2.25 to 113.96; p=0.006) compared with 4.06 (95% CI 1.44 to 11.43; p=0.008) in those with Tlco ≥60% of the predicted value. The difference between patients with Tlco <60% and ≥60% of the predicted value was not significantly different (p=0.074).
Relationship between variation in CAno level and change in FVC
After adjustment for FVC at baseline, FVC at the follow-up visit was related to CAno at baseline (β±SE −0.022±0.007, p=0.004) but not to its change (CAno at inclusion minus that at the follow-up visit; β±SE −0.003±0.004, p=0.450).
Discussion
In this prospective study which assessed various exhaled NO parameters, we found that CAno, a marker of alveolar inflammation, was able to predict subsequent lung function deterioration or death in patients with SSc (HR=6.06) with a CAno cut-off at 5.3 ppb. A CAno cut-off at 8.5 ppb allowed the identification (with 90% specificity) of patients at high risk of deteriorating lung function who subsequently developed SSc-related ILD. This prediction power of elevated CAno was then validated in an independent cohort population (figure 3 and 4).
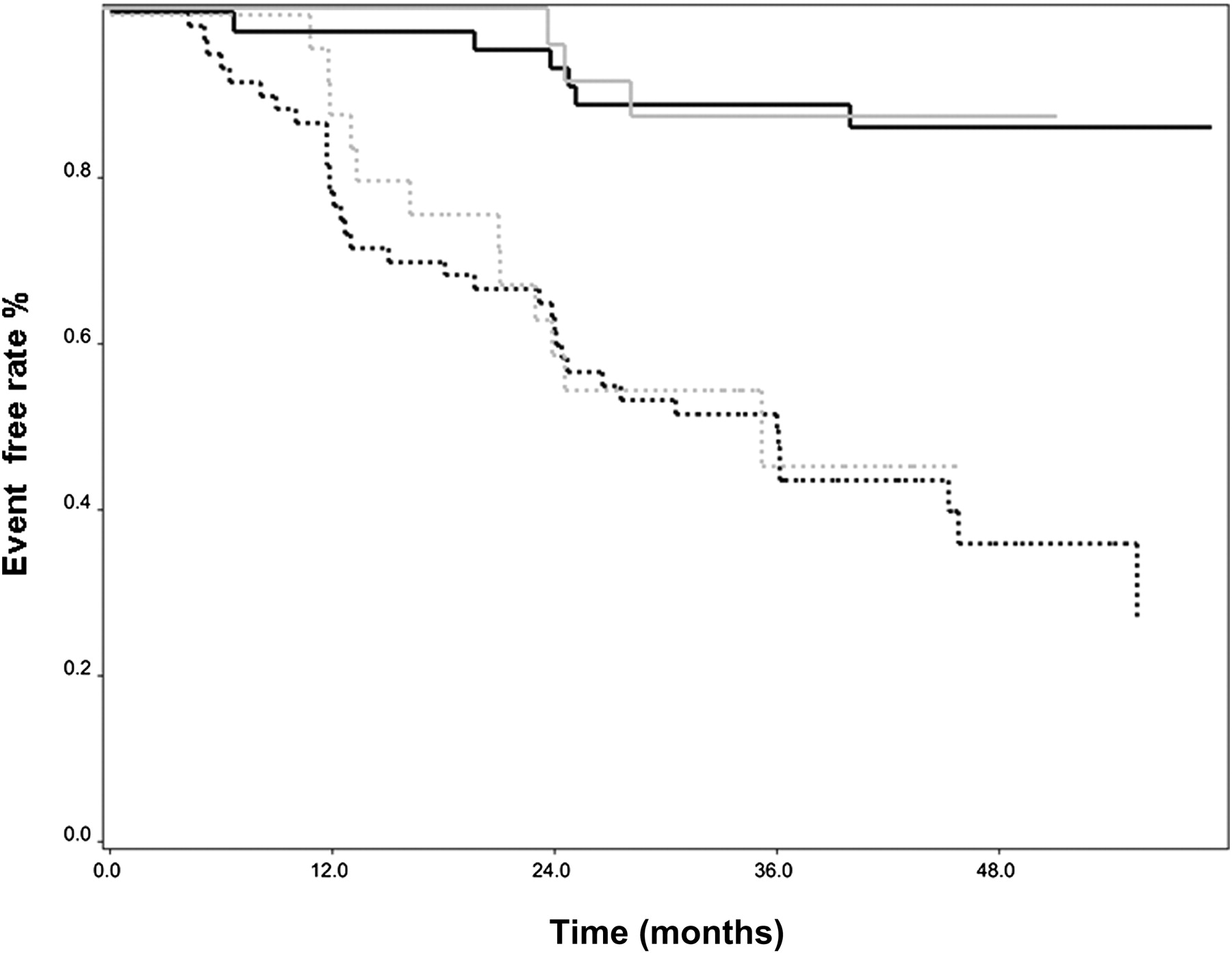
Kaplan–Meier survival analysis grouped by baseline alveolar concentration of nitric oxide (CAno) according to the best cut-off to predict deterioration in lung function or death 3 years after inclusion in the study. The survival curves are from two different populations. The black lines represent patients with systemic sclerosis (SSc) from Saint Antoine Hospital (n=105) and the grey lines represent patients with SSc from Cochin Hospital for external validation (n=48). The continuous lines show the survival curves for patients with SSc with CAno ≤5.3 ppb and the broken lines represent patients with SSc with CAno >5.3 ppb. Patients with SSc with CAno >5.3 ppb were more likely to develop lung function deterioration or death than other patients (log rank, p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
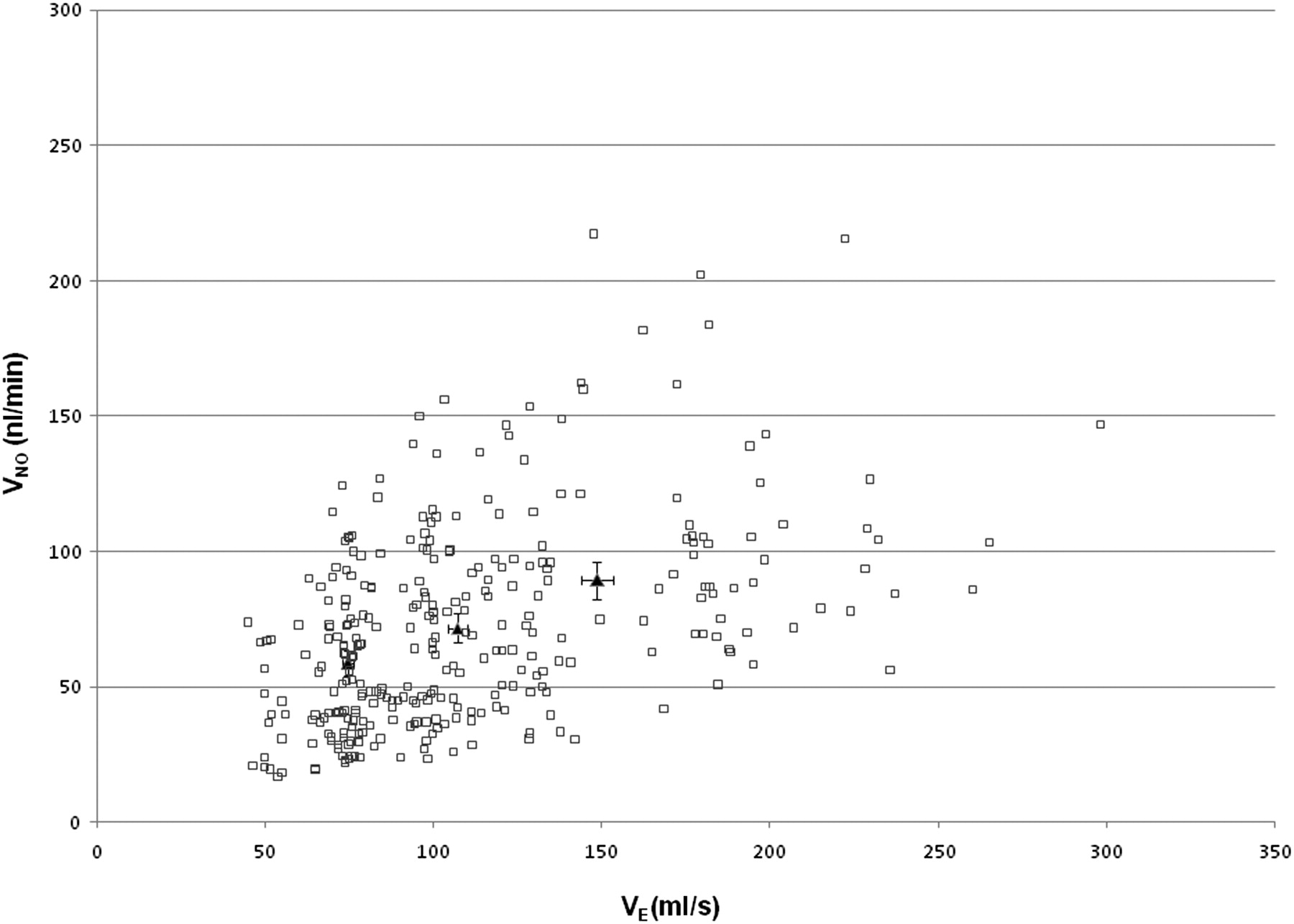
Exhaled flow rate (Ve) and nitric oxide exhaled flow rate (VNO) from patients with systemic sclerosis (SSc). Extended NO analysis may be less accurate in low exhaled flow rate <50 ml/s due to axial back diffusion. Eight of 105 patients with SSc had a first VE measurement of ≤50 ml/s; exclusion of these eight patients from the analysis did not affect the prediction power of baseline alveolar concentration of nitric oxide (CAno) for subsequent lung function deterioration or death (adjusted HR 2.98, p=0.0003). Each square represents one exhaled flow rate measurement. Each patient had three or more exhalations against positive different pressures that enabled calculation of CAno according to the model described by Tsoukias et al.12 The triangles represent the mean VE for exhalation against 50 ml/s, 100 ml/s and 150 ml/s; the majority of patients with SSc cannot maintain a stable VE against 200 ml/s.
The results of this study are consistent with the hypothesis that alveolar inflammation plays an important role in the progression of pulmonary fibrosis leading to SSc-related ILD. They provide strong evidence linking alveolar inflammation (as reflected by high levels of CAno) with losses in lung volumes due to progression of lung fibrosis during the natural course of the disease. Other prediction factors such as chest HRCT and FVC can also accurately detect or assess the extent of lung fibrosis in patients with SSc24 25 and have a relevant predictive value. Thus, a subgroup of patients with SSc with a history of progressive lung disease testified by a large area of ILD on HRCT scanning or lung volume restriction were more likely to have progression of lung disease during long-term follow-up.4 24 These morphological abnormalities of the lung and impaired pulmonary volumes resulted from initial alveolar inflammation that could not be currently measured by lung HRCT or PFTs. In this study, CAno added relevant information on the activity of lung disease, irrespective of the presence of ILD or a decreased level of FVC that are currently used as accurate predictive markers in SSc.24
Athough increased fractional exhaled NO is seen in patients with active alveolitis, documented by bronchoalveolar lavage cells count,26 and also in those without ILD-SSc,27 fractional exhaled NO was related to the severity of scleroderma lung disease.14 Assessing the locoregional NO output enables us to measure more precisely deep lung inflammation. Previous cross-sectional studies by our group have shown that CAno is increased in patients with SSc compared with controls14 28 and is higher in SSc patients with ILD than in patients without ILD.14 Moreover, CAno is directly related to the presence of ILD on chest HRCT scanning,29 probably due to as yet unknown biological mechanisms linking active alveolitis to cell proliferation and lung fibrosis in patients with SSc.15
Chest HRCT scanning and FVC are reliable tools for describing radiological abnormalities and lung volumes losses. Conversely, as increased NO synthesis directly results from inflammatory processes, CAno can accurately and specifically sense the presence of lung inflammation and quantify its importance, irrespective of the presence of lung fibrosis and its severity. It is therefore conceivable that high levels of CAno occur in some patients with lung inflammation but without ILD—for example, during the early course of their disease. Conversely, a patient with a long history of ILD can have normal levels of CAno during a quiescent phase of the disease when inflammatory processes are controlled or absent.
In this study the rate of progression in our patients was consistent with that reported in previous large cohort studies.4 The greater power of CAno to predict deteriorating lung function compared with FEno0.05 and J′awno is probably due to the fact that alveolar inflammation (as measured by CAno) rather than inflammation of the proximal airways (as measured by FEno0.05 and J′awno),30 31 plays an important role in the pathogenesis of pulmonary fibrosis in patients with SSc.
The optimal threshold of CAno allows us to demonstrate the relevance and the validation of CAno as an accurate predictor of subsequent deterioration in lung function or death in the course of SSc. The threshold of CAno, presently set at 8.5 ppb, might be useful to initiate treatments to prevent lung volume loss in future randomised clinical trials or to treat alveolar inflammation in the hope of delaying the development of lung fibrosis. We have previously reported in cross-sectional studies that high CAno levels were associated with the presence of ILD on lung HRCT scans or the ability of the serum to induce myofibroblast transition.14 28 29 Indeed, ILD can be ruled out in patients with CAno <3.8 ppb29 and increased CAno is associated with a severe form of ILD in SSc.14 Moreover, the serum from patients with CAno >4.3 ppb was able to induce lung fibroblast proliferation and myofibroblast conversion.15 These cut-offs were still relevant and added functional information on scleroderma lung disease at the time extended NO analysis was performed. In contrast to these previous thresholds, the present prospective cohort study reinforces the clinical usefulness of this measurement as CAno levels >8.5 ppb are strongly associated with the subsequent risk of lung function deterioration or death. External validation in an independent cohort of patients with SSc further reinforced the validity of this cut-off value.
In conclusion, our findings show that increased CAno is a non-invasive and valuable means of identifying patients with SSc at high risk of developing subsequent lung function deterioration or death, irrespective of the FVC level and the presence of ILD. This should allow clinicians to follow closely patients with progressive form and to initiate appropriate treatments in an early phase of disease.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval Ethics approval was provided by CPP Ile de France.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves