Article Text

Abstract
Background: Previous cross-sectional studies have shown that job change due to breathing problems at the workplace (respiratory work disability) is common among adults of working age. That research indicated that occupational exposure to gases, dust and fumes was associated with job change due to breathing problems, although causal inferences have been tempered by the cross-sectional nature of previously available data. There is a need for general population-based prospective studies to assess the incidence of respiratory work disability and to delineate better the roles of potential predictors of respiratory work disability.
Methods: A prospective general population cohort study was performed in 25 centres in 11 European countries and one centre in the USA. A longitudinal analysis was undertaken of the European Community Respiratory Health Survey including all participants employed at any point since the baseline survey, 6659 subjects randomly sampled and 779 subjects comprising all subjects reporting physician-diagnosed asthma. The main outcome measure was new-onset respiratory work disability, defined as a reported job change during follow-up attributed to breathing problems. Exposure to dusts (biological or mineral), gases or fumes during follow-up was recorded using a job-exposure matrix. Cox proportional hazard regression modelling was used to analyse such exposure as a predictor of time until job change due to breathing problems.
Results: The incidence rate of respiratory work disability was 1.2/1000 person-years of observation in the random sample (95% CI 1.0 to 1.5) and 5.7/1000 person-years in the asthma cohort (95% CI 4.1 to 7.8). In the random population sample, as well as in the asthma cohort, high occupational exposure to biological dust, mineral dust or gases or fumes predicted increased risk of respiratory work disability. In the random sample, sex was not associated with increased risk of work disability while, in the asthma cohort, female sex was associated with an increased disability risk (hazard ratio 2.8, 95% CI 1.3 to 5.9).
Conclusions: Respiratory work disability is common overall. It is associated with workplace exposures that could be controlled through preventive measures.
Statistics from Altmetric.com
In recent years, clinicians, researchers and insurers have paid increasing attention to questions of work disability, including ways to improve disability evaluations and approaches to better aid patients in their return to work. In this context, critical knowledge gaps must be addressed. For this effort, it is important to recognise the difference between having a health condition and experiencing disability, including work disability, as a disease may be present without concurrent disability.1 The aetiology of work disability is likely to be multifactorial and to reflect the interaction between the person with a health condition causing impairment and the environment in which that person is found. This interaction may induce or aggravate symptoms, further limiting functional ability and thus increasing the likelihood of disability. This pathway is particularly germane to respiratory disease. Severity of disease is a clear predictor for work disability among adults with asthma,2 3 and occupational exposures to irritants and dusts have been shown to promote respiratory disability.3–7
Respiratory work disability may be defined in a number of ways. Its most severe manifestation is complete cessation of employment due to respiratory difficulties. In addition, there are a number of other important measures of occupational disability, including lost work days, change in employment, limitation in job duties or reduction in work hours due to respiratory symptoms or disease.8 Current knowledge in this field is based on data from cross-sectional studies or from hospital-derived or physician-based panels of persons with asthma or other respiratory diseases. There is a clear need for general population-based prospective studies to assess the incidence of respiratory work disability and to delineate better the roles of potential predictors of respiratory work disability.
The present study is based on follow-up of an international general population study (European Community Respiratory Health Survey, ECRHS) comprising both a general population sample and a group of subjects with asthma at baseline.9 The aim is to measure the frequency of respiratory work disability in the general population and to estimate the impact of workplace exposures as risk factors for new-onset respiratory-related work disability.
METHODS
Baseline and follow-up ECRHS
The methodology of the ECRHS II has been described elsewhere.9 10 In the baseline study (ECRHS I, 1991–3), participating study centres used a short respiratory questionnaire to study a random sample of at least 3000 subjects per centre aged 20–44 years. Among the responders in the baseline study, both a random subsample of 20% of all subjects and a respiratory symptom-enriched group were invited to participate in a clinical investigation. At follow-up in 1998–2002 (ECRHS II), subjects from both the random and the symptom-based samples who participated at baseline were invited to complete a follow-up respiratory questionnaire and to participate in the second clinical investigation. Follow-up participation was achieved for 64% of the eligible baseline subjects.
Definition of study group
In the present study, two partially overlapping groups from ECRHS II were analysed—the random sample and a sample of subjects who reported physician-diagnosed asthma at the time of the baseline ECRHS I study. This “asthma cohort” included both subjects from the random sample and subjects from the symptom-enriched sample.
For the current analysis, subjects were required to meet the following criteria: a complete occupational history recorded at follow-up as well as no other missing data for key study predictors or outcomes; employment at any point since the baseline survey; and absence of reported respiratory work disability at baseline (job change attributed to breathing affected by work).
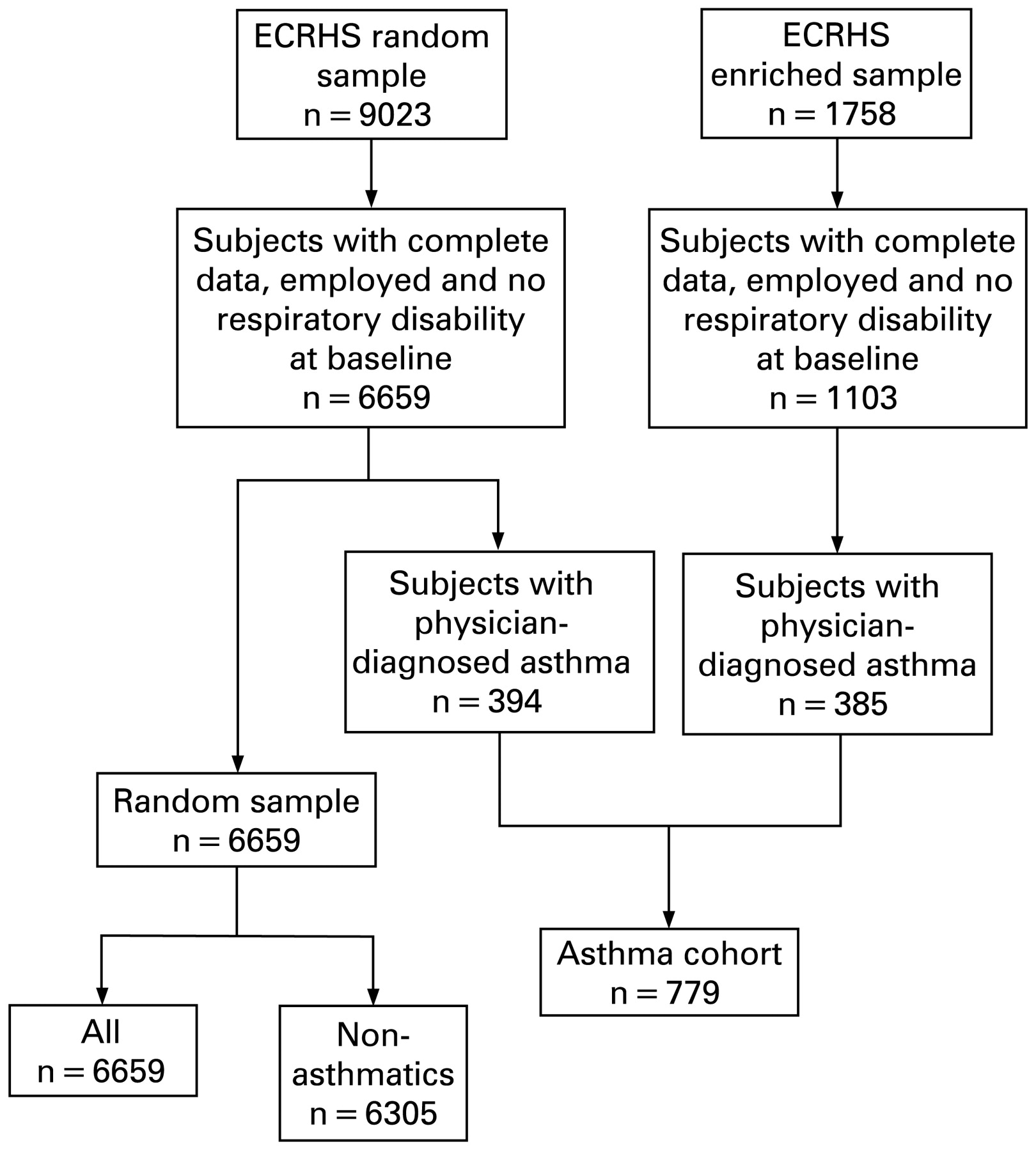
The final study population for this analysis comprised 6659 subjects from the random sample and 779 subjects from the asthma cohort, of which 394 (51%) originated from the random sample and 385 (49%) from the symptom-based sample. The subjects were from 25 centres in 11 European countries and one centre in the USA (fig 1).

{kind=link}
Flow chart of the selection of included subjects. ECRHS, European Community Respiratory Health Survey.
Respiratory work disability
Respiratory work disability was defined as a positive response at the follow-up to the questionnaire item: “Have you had to leave any job (during follow-up) because it affected your breathing?”5–7 Affirmative questionnaire responses to this item were followed up with identification of the specific employment involved.
Predictor variables
Occupations during the period of follow-up, including start-year and stop-year, were classified according to the International Standard Classification of Occupations.11 A job-exposure matrix (JEM) used these codes to classify each job in an individual’s employment history. The codes were linked to a JEM (ALOHA-JEM) to further classify each job as being of likelihood of exposure rated none, low (intermediate) or high for each of three categories of inhalants, biological dust, mineral dust and gases or fumes.12 13 This allowed collapse of exposure likelihood to address any of the three exposures. Thus, a low likelihood for biological dust, none for mineral dust and a high likelihood for exposure to gas or fumes would be assigned a high likelihood of any exposure. For subjects experiencing the event (respiratory work disability), only jobs until the event were taken into account to assess exposure.
A continuous 5-point scale symptom score was computed based on the following five questions concerning asthma-like characteristics during the last 12 months: wheeze with breathlessness; woken with tightness in chest; attack of shortness of breath at rest; attack of shortness of breath after exercise; and woken by attack of shortness of breath.14 Each is scored 1 point, with the resulting score potentially ranging from 0 to 5. We used this score as a proxy of active respiratory disease at baseline in the asthma cohort.
Smoking was classified based on information at baseline. Atopy was defined as a specific IgE level >0.35 kU/l to at least one of house dust mite, cat, timothy grass or Cladiosporium herbarum.15 Forced expiratory volume in 1 s (FEV1) was obtained at baseline for 6084 (91%) of the random sample and 709 (91%) of the asthma cohort by means of spirometry using standardised methods.12
Data analysis
The analyses were carried out using SAS Version 8.3 and STATA 10.0. Hazard ratios (HR) and 95% confidence intervals (95% CI) for respiratory work disability were modelled using Cox proportional hazards regression analyses. The outcome event was defined as respiratory work disability and time until event was determined by reported date of leaving the job in which the disability was reported. The exposure was analysed as a joint JEM exposure (biological dust, mineral dust, gases and fumes) or as separate exposure likelihoods for each subcategory of exposure.
In the multivariate models, potential confounders were selected a priori. These included geographical areas (English speaking (referent), northern, central and southern European countries), sex, age at follow-up, symptom score at baseline (treated as a continuous variable, smoking status at baseline (never, former and current) and exposure to passive smoking at work (at baseline), as well as one model using pack-years. When analysing the impact of each specific occupational exposure, the models also included the other two exposures. All models were run separately for the random sample and the asthma cohort, and stratified by sex and atopy. The main unstratified models were also run again, limited to non-asthmatic subjects in the random sample. Symptom scores were reanalysed, creating indicator variables for different numbers of cumulative symptoms with the referent category being no symptoms. We also re-estimated the basic model substituting FEV1% for the symptom score.
RESULTS
The characteristics of the random population sample and the asthma cohort are shown in table 1. The mean length of follow-up was 8.9 years in the random sample and 8.7 years in the asthma cohort, accumulating 59 265 person-years and 6777 person-years, respectively. The crude incidence rate of respiratory work disability was 1.2/1000 person-years of observation (95% CI 1.0 to 1.5) in the random sample and 5.7/1000 person-years of observation (95% CI 4.1 to 7.8) in the asthma cohort. The prevalence of occupational exposures based on JEM assignments in the two groups are shown in table 2. Altogether, a high likelihood of any exposure was present in 976 (15%) of the random sample and 101 (13%) of the asthma cohort which, as noted, overlaps the former group.
Random sample
Among subjects in the random population sample, a low likelihood of any occupational exposure to biological dust, mineral dust or gases or fumes conferred an increased risk of respiratory work disability (HR 2.0, 95% CI 1.1 to 3.4) with a further step-up in risk for a high likelihood of exposure (HR 3.4, 95% CI 1.8 to 6.6, table 3). Furthermore, when divided into separate exposure categories, a similar step-up in exposure risk was manifest for mineral dust (HR 2.3, 95% CI 1.1 to 4.8 and HR 2.9, 95% CI 1.1 to 7.2 for low and high likelihood, respectively). When we excluded subjects with asthma from the random sample, the “non-asthmatic random sample”, the results were quite similar, except for a higher step-up in risk for high likelihood of exposure to mineral dust (table 3).
Sex was not associated with increased risk for respiratory work disability in any of the multivariate models. The HR for female sex vs male sex was 1.2 (95% CI 0.7 to 2.0) (data not shown in table 3). In order to assess any potential sex-occupational exposure interaction, however, we reanalysed the data stratified by sex. In men, any high exposure to biological dust, mineral dust or gases or fumes was a strong predictor of respiratory work disability (HR 4.2, 95% CI 1.8 to 9.9). In women, the point estimate of risk related to any high exposure to biological dust, mineral dust or gases or fumes was lower and the 95% CI did not exclude unity (HR 2.1, 95% CI 0.5 to 9.4).
Atopy was not associated with an increased risk for respiratory disability (HR 1.5, 95% CI 0.8 to 2.6). Moreover, stratifying by atopy yielded estimates of occupational exposure risk among atopic subjects (HR 3.0, 95% CI 0.8 to 11.2) and non-atopic subjects (HR 4.0, 95% CI 1.5 to 10.6) that did not differ substantively from each other.
Asthma cohort
In the asthma cohort a high likelihood of occupational exposure to any biological dust, mineral dust or gases or fumes was associated with an increased risk of respiratory work disability (HR 3.5, 95% CI 1.4 to 9.0) that was not substantively different from that estimated in the random sample (table 3). When the separate exposure categories were analysed within the asthma cohort, the pattern of risk contrasted with that in the random sample: the highest point estimates were observed for biological dust and gases and fumes, although the 95% CIs did not exclude unity for any of these.
In contrast to the random sample, in the multivariate analysis of the asthma cohort women were at increased risk for respiratory work disability compared with men (HR 2.8, 95% CI 1.3 to 5.9). Stratifying by sex, occupational exposure to biological dust, mineral dust or gases or fumes in men imparted a markedly increased risk (HR 12.8, 95% CI 2.8 to 59.0) which was not the case in the women (HR 1.3, 95% CI 0.2 to 10.5).
Atopy was not associated with an increased risk for respiratory disability (HR 0.8, 95% CI 0.4 to 1.7), and stratifying for atopy yielded similar estimates of occupational exposure risk in subjects with atopic asthma (HR 3.5, 95% CI 0.9 to 13.3) and in those with non-atopic asthma (HR 3.9, 95% CI 0.5 to 27.6).
There was no significant effect of the symptom score (HR 1.2 per one point increase, 95% CI 1.0 to 1.4). Among those reporting one symptom (n = 135) compared with those reporting no symptoms (n = 169), the risk of respiratory disability was not clearly affected (HR 1.9, 95% CI 0.6 to 6.1) for one symptom. Among those reporting five symptoms (n = 90) compared to none, the risk was doubled (HR 2.4 (95% CI 0.7 to 8.0)), although the confidence interval included unity.
Additional analyses
Neither active smoking (either current, former or pack-years) nor second hand smoke exposure appeared to carry a risk for respiratory work disability. In all of the multivariate models, the HRs for the different smoking variables ranged from 0.7 to 1.3 with confidence intervals always including unity in all cases. As an additional sensitivity analysis we further retested the full model replacing the symptom score with baseline FEV1%. The results were similar, yielding increased HRs for high likelihood for any occupational exposures.
DISCUSSION
The key message of this analysis is that workplace exposure to dusts, gas or fumes is strongly associated with the subsequent risk of respiratory work disability, a common adverse event. Moreover, the present study is the first prospective general population study showing that workplace exposures play a substantial role in the occurrence of such disability, even taking into account other demographic and clinical factors.
We defined disability as a job change resulting from respiratory difficulties at work rather than a more extreme criterion such as complete work cessation. Nonetheless, such exposure-related job change is a reasonable marker of disability more broadly defined, subsuming lost work time, decreased productivity and complete job loss.
The results from this prospective study build on the findings of previous cross-sectional analyses. In our earlier analysis of the baseline population (ECRHS I), job change attributed to breathing difficulties was common, affecting approximately 4% of the random population and 12% of those with asthma.7 In that cross-sectional study, asthma-related occupational exposures carried a threefold risk of job change attributed to breathing problems.7 Other cross-sectional studies have also shown that various workplace exposures are of importance for respiratory work disability across income levels,2–6 16–18 and particularly in lower income working groups.6 19 20 Limited longitudinal data also support the role of occupation in asthma-related work disability.21 22
This analysis has important potential limitations that should be acknowledged. Occupational exposure misclassification could have occurred but is unlikely to explain the positive associations we observed. Had we relied on self-reported exposure, this could have led to systematic misclassification error (eg, reporting bias); JEM assignment misclassification is more likely to be random and, to the extent operative, biasing toward the null. Another source of misclassification could arise in relation to diagnostic labelling because, in the asthma cohort, some misclassification between asthma and chronic obstructive pulmonary disease may be present. Given the relatively young age distribution of the study group, however, such misclassification is unlikely to be a major factor.23 24 Having an occupation with a high physical demand is probably associated with an increased risk for respiratory disability.2 In this study we did not analyse the impact of physical exertion, which may be a confounder as dust-exposed blue collar occupations often are physically demanding.
Confounding bias may also affect this analysis. Our random population sample is not free of subjects with asthma. Because persons with illness are not excluded, this random sample should provide meaningful estimates of respiratory disability rates for the populations from which they were drawn. By the same token, the subset of those with disease theoretically could mediate some of the occupational exposure risk, leading to potential confounding. We addressed this by running a separate analysis for the population with the asthmatic subjects excluded (ie, the non-asthmatic random sample). The results were quite similar to those for the total random sample, except for mineral dust which was associated with a higher risk of respiratory work disability.
The current baseline population started with a working population, hence it may be possible that the asthmatic subjects were already self-selected into jobs that did not exacerbate their asthma and they may, to some extent, represent a healthy survivor population which would lead to an underestimation of the current exposure risks.
In addition to respiratory status, we also took into account other key confounders including the geographical region from which the subjects were drawn, active and second hand smoking (at work), age, atopic status and sex. Among these potential confounders, sex-related effects were the most salient. Women were at greater risk of disability, but only in the asthma cohort. In stratified analyses, in contrast, men in both the random sample and the asthma cohort were at substantively higher risk of occupationally-related respiratory work disability. These seemingly contradictory observations can be explained by an effect in which occupational exposure intensity for any given likelihood by JEM assignment is greater in men than women; in those with asthma, female sex is indeed a risk factor for respiratory disability, but this does not appear to be mediated by occupational exposure factors. Of note, previous cross-sectional analyses failed to show this sex-related pattern.7
The respiratory disability outcome central to this analysis was based on self-reporting. We did not validate these reports through external sources such as employment records or various social security measures (which would, in any event, have varied widely among the international centres). Nonetheless, disability in epidemiological studies is commonly measured by survey definitions dependent on self-reporting and thus our measure is comparable with others widely reported in the literature on this subject. One other limitation is that the approach we used does not capture changes of job activities or duties within the same job.
Finally, because this was a random multinational study, our results should have an external validity for other similar populations. Nonetheless, our findings may not extend to certain other populations such as those in emerging economies with different patterns of occupational exposure or profound disincentives to job change even in the face of work-related respiratory symptoms.
In summary, we found that over a period of 8 years, 1% of the population attributed job changes to respiratory problems while, among those with asthma, the cumulative incidence of such change was even higher (approximately 1 in 20). These findings suggest that, during a working career, 5% of all workers will experience such disability and, among those with asthma, 25% might face this challenge. This disability may be preventable in part if working conditions bringing exposure to dusts, gas and fumes were ameliorated.
Acknowledgments
KT, MK, J-PZ, JS, KR, DJ, HK, AdE, JMA and PDB designed the study. KT, JS, KR, DJ, AdE, FP were responsible for data collection in local centres. J-PZ, HK and KR were responsible for exposure assessments. EP and KT managed and analysed the data with additional input from PDB. All authors participated in the interpretation and presentation of the results.
REFERENCES
Footnotes
See Editorial, p 280
Funding: The coordination of the occupational asthma component of the ECRHS-II was supported by grant 1 R01 HL62633-01 of the US NIH/NORA/NHLBI. The coordination of ECRHS II was supported by the European Commission as part of their Quality of Life programme and from research contract No FOOD_CT_2004_506378, the Ga2len project, Global Allergy and Asthma European Network. The following bodies funded the local studies in ECRHS II included in this paper: Albacete: Fondo de Investigaciones Santarias (FIS) (grant code: 97/0035-01, 99/0034-01 and 99/0034-02), Hospital Universitario de Albacete, Consejeria de Sanidad; Antwerp: FWO (Fund for Scientific Research)-Flanders Belgium (grant code: G.0402.00), University of Antwerp, Flemish Health Ministry; Barcelona: SEPAR, Public Health Service (grant code R01 HL62633-01), Fondo de Investigaciones Santarias (FIS) (grant code 97/0035-01, 99/0034-01 and 99/0034-02) CIRIT (grant code 1999SGR 00241) Red Respira ISCII; Basel: Swiss National Science Foundation, Swiss Federal Office for Education & Science, Swiss National Accident Insurance Fund (SUVA), USC NIEHS Center grant 5P30 ES07048; Bergen: Norwegian Research Council, Norwegian Asthma & Allergy Association (NAAF), Glaxo Wellcome AS, Norway Research Fund; Erfurt: GSF-National Research Centre for Environment & Health, Deutsche Forschungsgemeinschaft (DFG) (grant code FR 1526/1-1); Galdakao: Basque Health Dept; Goteborg: Swedish Heart Lung Foundation, Swedish Council for Worklife and Social Research (FAS), Swedish Cancer & Allergy Foundation; Grenoble: Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, Ministere de l’Emploi et de la Solidarite, Direction Generale de la Sante, CHU de Grenoble, Comite des Maladies Respiratoires de l’Isere; Hamburg: GSF-National Reasearch Centre for Environment & Health, Deutsche Forschungsgemeinschaft (DFG) (grant code MA 711/4-1); Ipswich and Norwich: Asthma UK (formerly known as National Asthma Campaign); Huelva: Fondo de Investigaciones Santarias (FIS) (grant code 97/0035-01, 99/0034-01 and 99/0034-02); Melbourne: National Health and Medical Research Council of Australia; Oviedo: Fondo de Investigaciones Santarias (FIS) (grant code 97/0035-01, 99/0034-01 and 99/0034-02); Paris: Ministere de l’Emploi et de la Solidarite, Direction Generale de la Sante, UCB-Pharma (France), Aventis (France), Glaxo France, Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, CHU de Grenoble; Pavia: Glaxo-SmithKline Italy, Italian Ministry of University and Scientific and Technological Research (MURST), local university funding for research 1998 and 1999 (Pavia, Italy); Tartu: Estonian Science Foundation; Turin: ASL 4 Regione Piemonte (Italy), AO CTO/ICORMA Regione Piemonte (Italy), Italian Ministry of University and Scientific and Technological Research (MURST); Glaxo-SmithKline Italy; Umeå: Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Swedish Cancer & Allergy Foundation; Uppsala: Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Swedish Cancer & Allergy Foundation; Verona: University of Verona; Italian Ministry of University and Scientific and Technological Research (MURST); Glaxo-SmithKline Italy. United States: Department of Health, Education and Welfare Public Health Service (grant #2 S07RR05521-28).
Competing interests: None.
Ethics approval: Approval was obtained from all local ethics committees.
List of Principal Investigators and Senior Scientific Team. Australia: Melbourne (M Abramson, R Woods, E H Walters, F Thien, G Benke); Belgium: South Antwerp and Antwerp City (P Vermeire, J Weyler, M Van Sprundel, V Nelen); Estonia: Tartu (R Jogi, A Soon); France: Paris (F Neukirch, B Leynaert, R Liard, M Zureik); Grenoble (I Pin, J Ferran-Quentin); Germany: Erfurt (J Heinrich, M Wjst, C Frye, I Meyer); Iceland (T Gislason); Italy: Turin (M Bugiani, P Piccioni, A Carosso, W Arossa, E Caria, G Castiglioni, E Migliore, C Romano, D Fabbro, G Ciccone, C Magnani, P Dalmasso, R Bono, G Gigli, A Giraudo, M C Brussino, C Bucca, G Rolla ); Verona (R de Marco, G Verlato, E Zanolin, S Accordini, A Poli, V Lo Cascio, M Ferrari); Pavia (A Marinoni, S Villani, M Ponzio, F Frigerio, M Comelli, M Grassi, I Cerveri, A Corsico); The Netherlands (J Schouten); Norway: Bergen (A Gulsvik, E Omenaas, C Svanes, B Laerum); Spain: Barcelona (J M Antó, J Sunyer, M Kogevinas, J P Zock, X Basagana, A Jaen, F Burgos); Huelva (J Maldonado, A Pereira, JL Sanchez); Albacete (J Martinez-Moratalla Rovira, E Almar); Galdakao (N Muniozguren, I Urritia); Oviedo (F Payo); Sweden: Uppsala (C Janson, G Boman, D Norback, M Gunnbjornsdottir), Goteborg (K Toren, L Lillienberg, A Dahlman-Höglund); Umeå (E Norrman, M Soderberg, K Franklin, B Lundback, B Forsberg, L Nystrom); Switzerland: Basel (N Künzli, B Dibbert, M Hazenkamp, M Brutsche, U Ackermann-Liebrich); United Kingdom (P Burney, S Chinn, D Jarvis); Norwich (D Jarvis, B Harrison); Ipswich (D Jarvis, R Hall, D Seaton); USA: Portland (M Osborne, S Buist, W Vollmer, L Johnson). Development of job-exposure matrix: Roel Vermeulen.