





Abstract
Patients with chronic obstructive pulmonary disease (COPD) show impaired hypoxic pulmonary vasoconstriction that might contribute to abnormal gas exchange and could be related to endothelial dysfunction in pulmonary arteries. The aim of the study was to investigate the response of PA to hypoxic stimulus in vitro in COPD, and the role of endothelium-derived nitric oxide (NO) in this response.
The pulmonary arteries of 25 patients who underwent lung resection were studied. Patients were divided into controls, COPD+normoxaemia (COPDN) and COPD+hypoxaemia (COPDH). Hypoxic vasoconstriction (HV) was evaluated before and after stimulation or inhibition of the endothelial release of NO, and in the presence of exogenous NO.
Compared with the other groups, HV was reduced in COPDH. The magnitude of HV correlated with the oxygen tension in arterial blood. The hypoxic stimulus induced greater contraction after stimulating endothelial release of NO, whereas its inhibition practically abolished HV. Exogenous NO completely inhibited HV. Maximal relaxation induced by endothelium-dependent vasodilators correlated with the magnitude of HV.
In conclusion, pulmonary arteries of patients with chronic obstructive pulmonary disease and hypoxaemia have an impaired response to hypoxic stimulus, and the endothelial release of nitric oxide modulates hypoxic vasoconstriction. The depressed response of pulmonary arteries to hypoxia may contribute to abnormal gas exchange in chronic obstructive pulmonary disease.
- chronic airflow obstruction
- endothelial function
- gas exchange
- hypoxic pulmonary vasoconstriction
- lung
- nitric oxide
This study was supported by Grants 99/0188 and 00/0922 from the Fondo de Investigación Sanitaria, and SEPAR-2000 from the Sociedad Española de Neumología y Cirugía Torácica. V.I. Peinado is supported by the Comissió Interdepartamental de Recerca i Innovació Tecnològica and the Fundació Clínic per a la Recerca Biomèdica. S. Santos is the recipient of a Research Fellowship Award from the Sociedad Española de Neumología y Cirugía Torácica (SEPAR).
Hypoxic pulmonary vasoconstriction (HPV) is an effective mechanism regulating ventilation/perfusion ratio (V′A/Q′) matching, which plays an important role in modulating the arterial partial pressure of oxygen (PO2) in many respiratory disorders, including chronic obstructive pulmonary disease (COPD). Indeed, in this condition the inhibition of HPV deteriorates V′A/Q′ relationships, as shown by the diversion of blood flow to poorly ventilated alveolar units [l, 2]. Previous studies have shown that patients with mild COPD and moderate hypoxaemia may exhibit a reduced vascular response to both hypoxic stimulus 3 and the administration of 100% oxygen 4, suggesting an altered reactivity of pulmonary vessels to changes in inspired O2 concentration. Although the pathogenic mechanisms of this altered reactivity in COPD are not fully understood, in a previous study, the current authors showed that it was associated with changes in the normal structure of small pulmonary muscular arteries 2.
Endothelium-derived nitric oxide (NO) plays an important role in modulating both the vascular tone and vessel remodelling in pulmonary circulation. Studies conducted in isolated pulmonary arteries from COPD patients have demonstrated endothelial dysfunction in patients with severe 5 and mild 6 disease. In the latter study, both endothelial dysfunction and structural derangement of pulmonary arteries were already present in patients with mild COPD who were not hypoxaemic, and even in smokers with normal lung function. Accordingly, the authors suggested that arterial hypoxaemia might exert a secondary role in the pathogenesis of these vascular alterations at an early stage and that they were more likely to be related to a direct effect of tobacco smoke products 6. Therefore, the authors hypothesised that the impairment of endothelial function takes place early in the course of COPD and that it alters the response to hypoxic stimulus, hence promoting further gas exchange alterations.
The assessment of the response to hypoxic stimulus in patients with COPD in vivo is difficult, due to the frequent concurrence of hypoxaemia. In vitro studies, where pulmonary artery rings are exposed to hypoxia, have only been conducted in series of patients with undefined respiratory disease 7–9. To the current authors' knowledge, there are no studies where the profile of the response to hypoxic stimulus in pulmonary arteries of COPD patients had been characterised in vitro. Accordingly, the aims of the present study were two-fold: first, to characterise the response of pulmonary arteries to hypoxic stimulus in vitro in COPD patients with and without associated hypoxaemia; and second, to investigate the relationship between hypoxic vasoconstriction (HV) and endothelial function by specifically assessing the role of endothelium-derived NO.
Material and methods
Subjects
Twenty-five patients (two females, 23 males) who had undergone lobectomy or pneumonectomy because of localised lung carcinomas were studied. None of the patients had clinical evidence of pulmonary hypertension. Pulmonary function tests (forced spirometry, static lung volumes measured by body plethysmography and carbon monoxide diffusing capacity) and arterial blood gas measurements (23 patients) were performed during the days prior to surgery. The study was approved by the Ethical Research Committee of Hospital Clínic (Barcelona, Spain).
According to the results of forced spirometry and arterial blood gases, patients were classified into three groups. 1) Controls. Patients with normal lung function and an oxygen tension in arterial blood (Pa,O2) within the normal range (>10.64 kPa (80 mmHg)). 2) COPD+normoxaemia (COPDN). Patients with airflow obstruction (forced expiratory volume in one second (FEV1) <80% predicted and FEV1/forced vital capacity (FVC) <70% pred) and Pa,O2 >10.64 kPa (80 mmHg). 3) COPD+hypoxaemia (COPDH). Patients with airflow obstruction along with arterial hypoxaemia (Pa,O2 <10.64 kPa (80 mmHg)). General characteristics and lung function data are shown in table 1⇓.
Characteristics of the patients
Preparation of pulmonary artery rings
Artery rings were processed as described previously 6. Briefly, resected lung specimens were placed in cold Krebs-Henseleit's (KH) buffer (containing (in mM) 118 NaCl, 24 NaHCO3, 11.1 glucose, 4.7 KCl, 1.2 KH2PO4, 1.2 MgSO4, 2.5 CaCl2) and gassed with 21% O2/5% carbon dioxide (pH 7.35–7.45). Arterial segments with an external diameter of 1.8–2.3 mm were carefully dissected free of visible fat and connective tissue, and cut into rings ∼3 mm long. Four rings per patient were suspended in 20 mL organ bath chambers (Panlab, Barcelona, Spain) filled with KH buffer, aerated continuously with 21% O2 and 5% CO2, and kept at 37°C by an outer water bath warmed by a recirculating heater. Changes in isometric tension were recorded in each ring by a force transducer (Panlab) connected to a computerised chart drive recorder. A resting tension of 1.75 g was applied to each ring. After equilibration for ≥90 min, all rings were pre-incubated for 30 min with indomethacin (1×10−5 M) in order to inhibit the synthesis of cyclooxygenase products of arachidonic acid, which was present in the bath throughout all the experiments. The O2 tension in the organ bath was continuously recorded by immersing an oxygen electrode (Oxygen Meter, Model 781; Strathkelvin Instruments, Bearsden, UK) in one of the chambers. Arterial rings were studied under normoxic and hypoxic conditions. For normoxic conditions, KH was gassed with a 21% O2/5% CO2/74% (nitrogen) N2 gas mixture, which yielded a PO2 in the organ bath chamber of 20.1±0.3 kPa (151±2 mmHg) at 37°C in the proximity of the artery ring. Hypoxic conditions were induced by bubbling KH with a 5% CO2/95% N2 gas mixture, which resulted in a decrease of PO2 to 0.53±0.1 kPa (4±1 mmHg) after 1–2 min.
Response to hypoxic stimulus
After equilibration, all rings were precontracted with noradrenaline (NA) (1×10−7–1×10−6 M) to obtain a stable plateau of tension. After the contraction had stabilised, hypoxia was rapidly induced for 10 min, and the change in vascular tension recorded. After exposure to hypoxia, normoxic conditions were re-established and rings were rinsed with KH and allowed to equilibrate for 60 min.
Interaction between nitric oxide and the response to hypoxic stimulus
To determine the potential role of endothelium-derived NO in the responsiveness to hypoxia, arterial rings were studied in three steps. In the first step, rings were initially contracted with NA (1×10−7–1×10−6 M) and after the contraction had stabilised, two rings were assayed with a single dose of the following NO-dependent vasodilators: adenosine diphosphate (ADP) (1×10−6 M) and histamine (1×10−7 M), one in each ring. A third ring was assayed with the NO donor sodium nitroprusside (SNP) at a concentration of 1×10−8–1×10−7 M. In the second step, when the maximal relaxation for each vasodilator was achieved, rings were exposed to hypoxia for 10 min and then normoxic conditions were re-established. In the third step, the effect of NO synthesis inhibition was assessed. To this end, NG‐monomethyl‐l‐arginine (l‐NAME) (1×10−3 M) was added to the vasodilator present in the bath chamber (histamine or ADP) and the hypoxic stimulus was repeated after 10 min. At the end of the experiments, all rings were rinsed out and contracted maximally with KCl (60 mM) in order to establish the maximal contractile response. Additionally, the microscopic appearance of endothelium was evaluated after the experiments in some of the arteries, by staining with anti-factor VIII-related antigen, in order to rule out the possibility that the manipulation during the experiment could have damaged the endothelial cells.
After exposure to hypoxia in NA precontracted rings, four different doses of SNP in a concentration range from 1×10−11–1×10−7 M were assayed in 12 patients (four rings per patient, one dose in each ring) and then re-exposed to hypoxia. The response to hypoxia after the treatment with SNP was expressed as a percentage of previous response. In order to check the direct effect of NO on the response to hypoxia, a second set of experiments was performed in four artery rings, where the bath solution was bubbled with NO gas at a concentration of 50 parts per million (ppm) NO, measured by a chemiluminiscence analyser (CLD 700 AL; Eco Physics, Hombrechtikon, Switzerland), and then exposed to hypoxic stimulus. All drugs were purchased from Sigma Chemical Company (St Louis, MO, USA).
Measurements
HV was assessed as the difference between the maximal tension achieved after exposure to hypoxia and the tension recorded just prior to the hypoxic stimulus. The change in tension induced by hypoxia was expressed as the percentage of maximal contraction induced by KCl. Relaxation of each pulmonary artery ring was determined by measuring the reduction in tension induced by each vasodilating agent (ADP and histamine) and expressed as the percentage of maximal contraction to KCl.
Statistical analysis
All data are expressed as means±sd. Comparisons between groups were performed using an analysis of variance (ANOVA). When significant, post hoc pairwise comparisons using the Newman-Keuls test were applied. Comparisons of hypoxic responses between NA precontracted rings before and after incubation with a vasodilator were performed using a paired t‐test. Relationships between variables were assessed using the Pearson's correlation test. Logarithmic transformation of variables was applied when appropriate. A p‐value <0.05 was considered significant in all cases.
Results
The control group was composed of two nonsmokers and five smokers. COPD patients were heavy smokers and showed a moderate degree of airflow obstruction (table 1⇑).
Vascular reactivity to hypoxia
A representative response of an isolated pulmonary artery ring to hypoxic stimulus is shown in figure 1⇓. After precontraction with NA, exposure to hypoxia caused an intense contraction that started at a PO2 in the organ bath of 20–30 mmHg, although to obtain maximal and reproducible responses, a PO2 <1.33 kPa (10 mmHg) was required. Contraction to hypoxia peaked within 3–5 min of exposure and remained stable for ≥5 min (fig. 1⇓). Lengthy exposures induced a slow and gradual decrease in tone in some rings. Restoration of normoxic conditions completely abolished the hypoxia-induced contraction. The pattern of response to hypoxic stimulus observed in the present study is similar to that shown in pulmonary arteries with smaller diameter 7. The results of the response to hypoxia in the three groups are summarised in table 2⇓. The change in tension generated by the hypoxic stimulus was significantly lower in hypoxaemic COPD patients, as compared with the other two groups. No differences in the response to the hypoxic stimulus were observed between normoxaemic COPD patients and controls. The magnitude of the response to hypoxia in vitro was significantly correlated with the arterial PO2 (r=0.62, p<0.01) (fig. 2⇓).

Representative response of an isolated pulmonary artery ring precontracted with noradrenaline (NA) and exposed to hypoxia (95% nitrogen). PO2: partial pressure of oxygen in the organ bath medium. 1 mmHg=0.133 kPa.

Relationship between the change in tension induced by hypoxic stimulus in vitro in pulmonary artery rings and the arterial partial pressure of oxygen (PO2). •: controls; ○: chronic obstructive pulmonary disease (COPD)+normoxaemia; ▴: COPD+hypoxaemia. r=0.62, p<0.01. 1 mmHg=0.133 kPa.
Changes in tension of pulmonary artery rings induced by different interventions
Hypoxic vasoconstriction after induction of endogenous nitric oxide release
Maximal contraction to NA (1×10−6 M) was similar in the three groups. In agreement with previous observations 6, the relaxation induced by ADP (1×10−6 M) was reduced in the COPD patients, taken as a whole group, when compared with the control group (31±14 versus 22±8% of maximal contraction to KCl, controls and COPD patients, respectively; p=0.05). As shown in table 2⇑, hypoxaemic COPD patients exhibited the lowest reactivity to NO-dependent vasodilators. Indeed, the endothelial function, as assessed by the magnitude of vasorelaxation induced with ADP or histamine, correlated with the magnitude of the response to hypoxic stimulus (ADP: r=0.59, p<0.01; histamine: r=0.46, p<0.05) (fig. 3⇓). When the hypoxic stimulus was applied to artery rings pretreated with an NO-dependent vasodilator (histamine or ADP), there was a change in tension greater than that obtained with hypoxia alone (p<0.01) (fig. 4a⇓, table 2⇑), although the maximal tension achieved was similar. Artery rings from hypoxaemic COPD patients also showed a reduction in the magnitude of the contraction to hypoxia after induction of NO release, as compared with the other two groups (table 2⇑).

Relationship between the endothelial function, assessed by the maximal relaxation induced by adenosine diphosphate (ADP) (log transformed), and the response to a hypoxic stimulus in pulmonary artery rings. •: controls; ○: chronic obstructive pulmonary disease (COPD)+normoxaemia; ▴: COPD+hypoxaemia. r=0.59, p<0.01.

Evaluation of the effect of endothelium-derived nitric oxide (NO) on hypoxic contraction in pulmonary arteries. Experimental procedures were performed in three steps. In the first step, after contraction with noradrenaline, endothelium-dependent relaxation was assessed with a) histamine (HIS; 1×10−7 M) or b) the NO donor sodium nitroprusside (SNP; 1×10−8 M). In the second step, when maximal relaxation for histamine was achieved, the artery rings were exposed to hypoxia (H) for 10 min and then normoxic conditions were re-established. In the third step, NO synthesis was inhibited with NG‐monomethyl‐l‐arginine (l‐NAME; 1×10−3 M) and, after 10 min, the hypoxic stimulus was repeated. The change in tension was measured as the difference between the maximal tension achieved after exposure to H and the tension recorded just prior to the hypoxic stimulus. N: normoxia.
Hypoxic vasoconstriction after treatment with exogenous nitric oxide
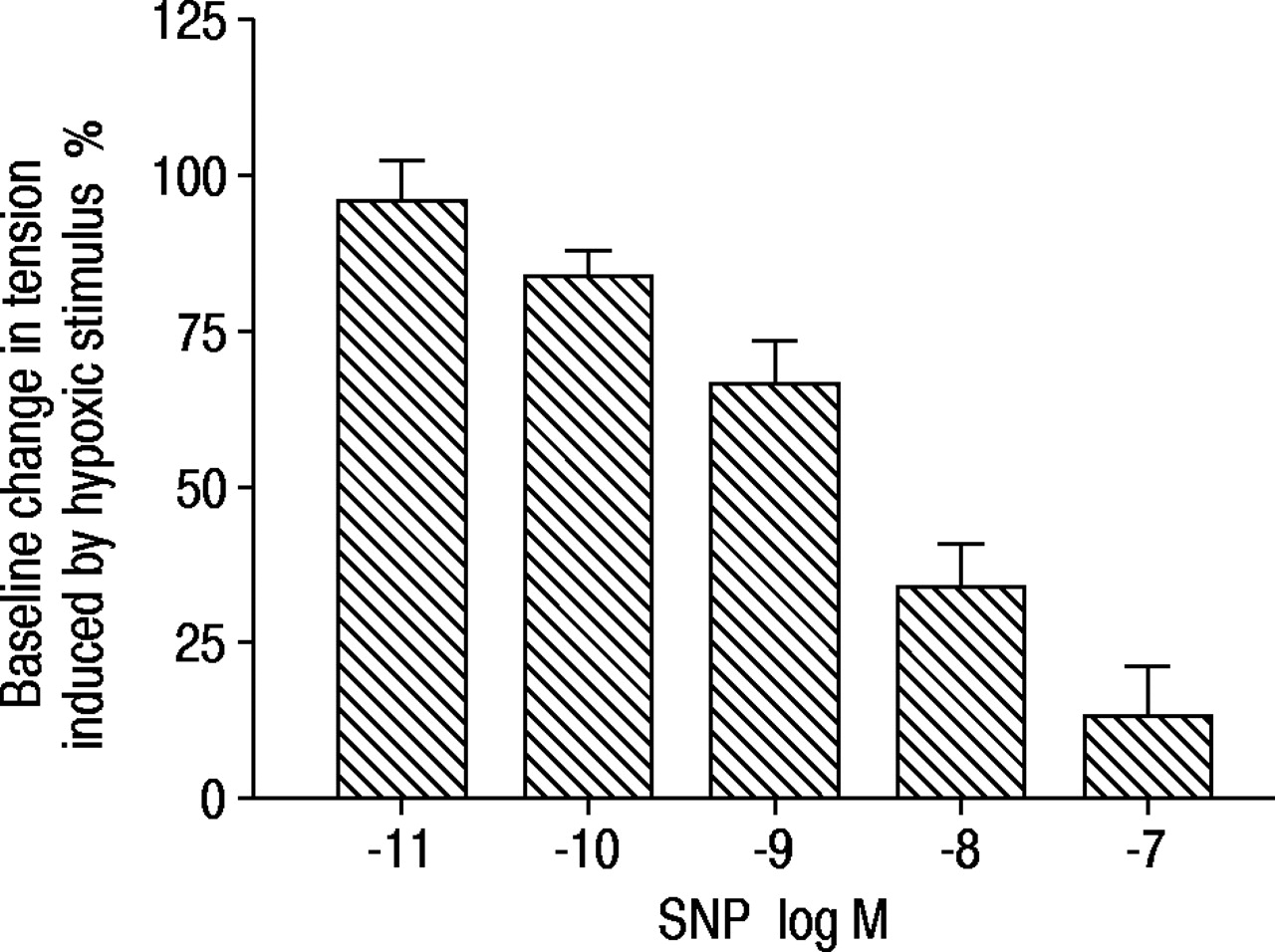
In contrast with the previous findings, when the hypoxic stimulus was applied to arteries pretreated with SNP the contraction was practically abolished (fig. 4b⇑). Such inhibition of the contraction to hypoxia was dose-dependent (fig. 5⇓), with total inhibition at a concentration 1×10−7 M. Furthermore, NO (50 ppm) directly bubbled into the organ bath also completely inhibited HV (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in tension induced by a hypoxic stimulus in pulmonary artery rings pretreated with different concentrations of sodium nitroprusside (SNP). Data are presented as mean±SD. n=6–12.
Hypoxic vasoconstriction in nitric oxide inhibited rings
The addition of l‐NAME (1×10−3 M) to artery rings pretreated with an NO-dependent vasodilator caused an intense increase in tension under normoxic conditions, which was similar in all groups. The subsequent change in tension in response to the hypoxic stimulus was significantly attenuated in all groups and totally inhibited in hypoxaemic COPD patients (fig. 4a⇑, table 2⇑).
Discussion
The results of the present in vitro study show a reduction in the response to hypoxic stimulus in the pulmonary arteries of patients with moderate COPD and mild hypoxaemia, compared to control subjects and normoxaemic COPD patients. This reduction was associated with a decline in endothelium-dependent relaxation. Moreover, the response to hypoxic stimulus in vitro correlated significantly with arterial PO2 values.
It is generally accepted that in disease states associated with decreased alveolar PO2, persistent HV and vascular remodelling are the main mechanisms of pulmonary hypertension. For this reason, the reduced response to hypoxia in vitro in hypoxaemic COPD patients found in this study may seem controversial. However, studies performed in COPD patients have shown a wide variation in the individual responses of the pulmonary circulation to changes in inspired O2 concentration 2, 3, 10. In general, patients with end-stage COPD tend to exhibit a lower vascular response to O2 breathing than patients with milder forms of the disease 4, 11. Overall, these clinical findings and the results of the current investigation are consistent with a diminished vascular reactivity to hypoxic stimulus in a subgroup of patients with COPD, especially those with greater gas exchange impairment.
A reduced response to hypoxic stimulus may have detrimental effects on pulmonary gas exchange in COPD, where hypoxaemia is essentially due to a V′A/Q′ imbalance 12, 13. The impairment of the vascular regulation of V′A/Q′ matching may worsen arterial oxygenation. This hypothesis appears to be confirmed by the significant correlation between the response of pulmonary artery rings to hypoxia in vitro and the arterial PO2 (fig. 2⇑), namely the lower the response to hypoxia in vitro the lower the Pa,O2. This finding is in agreement with the results of McMurtry et al. 14 who showed a decreased pressor response to acute hypoxia in chronically hypoxic rats. However, it is important to note that the COPD patients in the present study only had a moderate degree of airflow obstruction and did not have clinical evidence of pulmonary hypertension. Even in the majority of hypoxaemic patients, the Pa,O2 was >9.31 kPa (70 mmHg). Therefore, these findings suggest that alterations in the reactivity of pulmonary arteries to hypoxia may develop when the degree of airflow obstruction is modest, and may play a pathogenic role in gas exchange impairment.
Pulmonary endothelium is a well-known modulator of vascular tone. Its role in the hypoxic response has been recognised by many authors 15, 16, although there is controversy in many aspects. In this study, patients with better endothelium-dependent relaxation were those with a greater response to hypoxia (fig. 3⇑). This observation suggests that the NO pathway could be partially involved in the regulation of HPV. Indeed, the change in tension induced by hypoxia was greatest in arteries pretreated with agents that induce the endothelial release of NO (fig. 4a⇑). This does not seem to be an effect of a lower precontractile arterial tone, since vessels that were previously relaxed with SNP did not contract when exposed to hypoxia (fig. 4b⇑). Furthermore, whereas the inhibition of endothelial nitric oxide synthase (eNOS) with l‐NAME in artery rings pretreated with an endothelium-dependent vasodilator induced a strong increase in tension during normoxia, there was little additional contraction when hypoxic stimulus was applied (table 2⇑). All in all, these findings are consistent with the notion that HPV is somehow related to the inhibition of an endogenous vasodilator, rather than to the synthesis and release of a vasoconstrictor 7, 17, 18. Hypoxia might induce a decrease in NO availability, although the mechanisms of this inhibition are uncertain. Since molecular O2 is needed to form NO and l‐citruline by eNOS, it is conceivable that hypoxia could be a rate-limiting factor for NO synthesis. However, additional mechanisms should contribute to HV, since, in this series, the current authors found a few number of arteries with reduced or absent HV despite stimulation of eNOS.
HV was also abolished by an exogenous source of NO, in agreement with previous experimental data documented by Ohe et al. 9 and clinical studies in healthy subjects 19 and COPD patients 12. The authors found that the presence of endothelium-independent vasodilators, such as SNP or NO gas bubbled directly in the organ bath chamber, were potent and effective antagonists of hypoxic contraction. With regard to SNP, the inhibitory effect was dose dependent (fig. 5⇑). Presumably, an excess of exogenous NO acts directly on soluble guanylate cyclase overcoming the effect of hypoxia on smooth muscle cells. In perfused rabbit lungs, Weissmann et al. 20 showed that NO-dependent guanylate cyclase activity had an important role in attenuating the vasoconstrictor response to hypoxia, whereas NO-independent stimulation of guanylate cyclase did not modify HV. This inhibitory action of exogenous NO on HV does not rule out the concept that HV could be caused by the decreased availability of endogenous NO, since an exogenous source of NO could exert a negative feedback on its endogenous synthesis 21. Evidence of an altered vasoreactivity to hypoxia-induced hypertension has also been reported in lungs perfused after a prolonged period of NO inhalation, suggesting a direct inhibition of eNOS activity by NO itself 22.
The mechanisms by which some COPD patients show a reduced response to hypoxia are unclear. It is commonly believed that chronic hypoxaemia plays a key pathogenic role in altering endothelial NO-dependent vasodilation in the pulmonary vasculature 23–25. However, this view has been challenged by the finding that both structural abnormalities and endothelial dysfunction in pulmonary arteries can be observed, at least in part, in both smokers with normal lung function and nonhypoxaemic patients with mild COPD 6, 12, 26. This suggests that tobacco smoke components may play a direct role in altering the pulmonary circulation 6, 27. The current authors have recently shown a decreased expression of eNOS in the pulmonary arteries of smokers 28. Presumably, the initial event in the natural history of pulmonary hypertension in COPD could be the lesion of the pulmonary endothelium by cigarette-smoke products, with subsequent downregulation of eNOS expression and impairment of endothelial function. According to the present investigation, HV might also be impaired at this stage. This may further worsen V′A/Q′ matching and promote the development of arterial hypoxaemia. In this scenario, sustained exposure to moderate hypoxaemia may eventually lead to pulmonary vascular remodelling that may further amplify the initial effects of tobacco-smoke products.
In summary, the results of the present study show that in pulmonary arteries of chronic obstructive pulmonary disease patients, endothelium-derived nitric oxide synthase-dependent relaxation and hypoxic vasoconstriction seem to be associated phenomena. These findings also suggest that a depressed hypoxic response in chronic obstructive pulmonary disease can diminish the effectiveness of vessel contraction, altering the adaptation of pulmonary circulation to different oxygen concentrations, and thereby promoting the development of arterial hypoxaemia.
- Received January 17, 2002.
- Accepted March 12, 2002.
- © ERS Journals Ltd
References









