Article Text

Abstract
Background: Appropriate ventilation together with improvement of clinical care of premature babies can contribute to reducing lung inflammation, known to represent the “primum movens” of bronchopulmonary dysplasia (BPD). High-frequency oscillatory ventilation (HFOV) and volume-guarantee (VG) ventilation are effective in the treatment of neonatal respiratory distress syndrome (RDS).
Objective: To assess the potential of HFOV and VG to prevent BPD in the acute phase of RDS, by a randomised clinical study evaluating lung inflammation in premature infants.
Study design: Forty infants (gestational age 25–32 weeks) with RDS were assigned to assist-control ventilation plus VG (Vt = 5 ml/kg) or HFOV (both with a Dräger Babylog 8000 plus ventilator). Levels of interleukin (IL) 6, IL8 and tumour necrosis factor were determined in tracheal aspirate on days 1, 3 and 7 of life.
Results: In the HFOV group IL6 levels were significantly higher on day 3 (0.5 (0.2) vs assisted-control ventilation plus VG group 0.1 (0.2) ng/ml) and oxygen dependency was significantly longer (36 (23) vs assisted-control ventilation plus VG group 19 (11) days).
Conclusion: VG ventilation is an effective lung-protective strategy to be used in acute RDS, inducing a lower expression of early inflammation markers than HFOV. Whether the use of this initial ventilatory strategy contributes to the prevention of BPD requires further studies.
Statistics from Altmetric.com
Bronchopulmonary dysplasia (BPD) still remains one of the most important sequelae in mechanically ventilated preterm infants with respiratory distress syndrome (RDS). Volutrauma, infections, persistent ductus arteriosus (PDA) and oxygen promote lung inflammation inducing alveolar growth disorders and the development of BPD.1 2
Increased levels of cytokines have been observed in bronchoalveolar lavage fluid of ventilated preterm infants who subsequently developed BPD.3–5 Lung-protective strategies during mechanical ventilation have been strongly recommended to avoid “ventilation-induced lung injury”.6 First intention high-frequency oscillatory ventilation (HFOV) applied as a high lung volume strategy by using a small tidal volume (Vt) and with a constant alveolar distending pressure optimises lung recruitment7 8 and recently, HFOV and conventional ventilation appeared equally effective for RDS.9–11 On the other hand, the patient-triggered ventilation (PTV) plus volume-guarantee (VG) option, maintaining a constant preset Vt, was shown to limit lung volutrauma.12 13
PTV plus VG (with an adequate Vt of 5 ml/kg) has been shown to reduce lung inflammation in preterm infants during the acute phase of RDS compared with PTV alone14 or PTV plus “low” VG (Vt of 3 ml/kg).15 Dani et al demonstrated that HFOV is associated with a reduction of lung inflammation versus pressure support ventilation plus VG (Vt = 5 ml/kg) and positive end expiratory pressure (PEEP) levels of 3–4 cm H2O, in preterm infants with RDS.16 The relative efficacy of HFOV and PTV plus VG during the acute phase of RDS and their long-term effect on lung injury have not yet been compared. We hypothesised that assist-control (A/C) plus VG (Vt = 5 ml/kg) with an adequate PEEP could be safely used in the acute phase of RDS, inducing the same or lower lung inflammation as HFOV, thus reducing length of ventilation and the risk of BPD.17
METHODS
Forty-five inborn premature infants consecutively born at 25–32 weeks’ gestation, who had received at least one course of prenatal glucocorticoids and who required tracheal intubation and mechanical ventilation in the first hour of life because of severe RDS (arterial-to-alveolar oxygen ratio <0.2) were considered eligible. RDS was diagnosed according to usual radiological and clinical criteria. Five infants were excluded owing to the presence of lethal congenital anomalies, severe intraventricular haemorrhage (IVH, above grade II), suspected infection or absence of parental consent. After delivery all neonates underwent the same management and were given distending pressure for alveolar recruitment using a pressure control system (Neopuff, Fisher & Paykel, Rome, Italy): Peak inflation pressure (PIP) was increased to 20–25 cm H2O for 2 seconds to open up atelectatic regions, then reduced (by observing chest–wall motion and air entry) with a continuously delivered PEEP of 5 cm H2O to maintain an oxygen saturation (Sato2) of 88–92% with a minimal fractional inspired oxygen concentration (Fio2). Infants not breathing spontaneously were intubated in the delivery room and supported with conventional ventilators (delivered PEEP 5 cm H2O).
Within 60 minutes of birth, all studied infants required intubation and A/C ventilation was performed (Babylog 8000 plus; Dräger, Lubeck, Germany) with the ventilatory settings selected to maintain a Vt of 5 ml/kg. All the patients received the first dose of endotracheal porcine natural surfactant (200 mg/kg; Curosurf, Chiesi, Italy) within the first 3 hours of life. Additional doses were given if the infants required ventilation with mean airway pressures (PAW) above 7 cm H2O and FiO2 over 0.30, 6–12 hours after the previous dose.
All the enrolled infants (n = 40) were randomised at 1 hour of life into two groups—A/C+VG (Vt = 5 ml/kg) and the HFOV group—using a stratified randomisation for gestational age (GA) (GA 25–28 weeks; GA 29–32 weeks). Every eligible infant entered the A/C+VG (n = 19) or HFOV group (n = 21) following a sequence of random numbers. Both groups were ventilated using Babylog 8000 plus, software version 5.0. In the high-frequency mode, this device delivers a high inspiratory continuous flow (max 30 l/min) and generates oscillations by rapidly switching the inspiratory valve. The oscillation amplitude is adjustable as a percentage from 0 to 100% (100%, the highest possible amplitude according to PAW, frequency settings and the characteristic of the respiratory system). The Babylog 8000 plus uses a PEEP/continuous positive airway pressure-servocontrol system to adjust PAW. Active expiration is provided with a jet Venturi system. The I:E ratio is automatically regulated (range 0.2–0.8) depending on PAW setting and frequency.
In the A/C+VG group, we set a back-up ventilation using PIP to deliver a Vt = 5 ml/kg. The set Vt was always kept constant. Moreover, we set a mean PEEP of 5 cm H2O, a minimal Fio2 to maintain Sato2 90–94%, an inspiratory time set at 0.35 seconds, an inspiratory flow allowing plateau pressure to be reached within the first third of the inspiratory time (mean 6 l/min) and a respiratory rate of 60 bpm, which was reduced when the neonate was able to maintain an adequate gas exchange (eg, pH >7.25; po2 50–75 mm Hg; pco2 40–65 mm Hg). HFOV was initiated with a rate of 10 Hz, a PAW of 8–10 cm H2O, and an amplitude of 40%. Since the effective amplitude of the Babylog HFOV is frequency dependent, we always kept the frequency at 10 Hz. Then the high-volume strategy was applied: in order to maintain a Pao2 >50 mm Hg, when the Fio2 was >0.3 the PAW was increased by 0.5 to 1 cm H2O every 10–15 minutes until it was possible to reduce the Fio2.18
According to our protocol, weaning during VG occurred in real time by automatic reduction of PIP in response to improving pulmonary mechanics (self-weaning mode);19 in the HFOV group, when the PAW level was below 8 cm H2O and FiO2 was below 0.3, the neonates were switched to A/C+VG (Vt = 5 ml/kg and PEEP = 5 cm H2O). The extubation was mandatory within 2–3 hours after reaching extubation criteria (PIP: 10–15 cm H2O, PAW <6 cm H2O and Fio2 <0.3 to maintain a po2 >50 mm Hg and pco2 <65 mm Hg). None of the patients needed reintubation. Heart rate, systemic blood pressure and Sato2 were monitored, while arterial blood gas measurements were regularly made. We also recorded duration of ventilation, incidence and rate of treatment of PDA, surfactant treatment, incidence of air leaks, IVH occurrence, oxygen dependency on day 28 and/or at 36 weeks of postconceptional age. Within 24 hours of life, an echocardiographic evaluation was done to identify PDA which needed treatment (ibuprofen 10 mg/kg intravenously (IV), followed by two doses of 5 mg/kg IV at 24-hour intervals). No steroids were given in the first week of life. Infants who were more than 15 days of age and ventilated with an Fio2 of at least 0.40 received a short course of dexamethasone (0.5 mg /kg IV a day for 3 days).
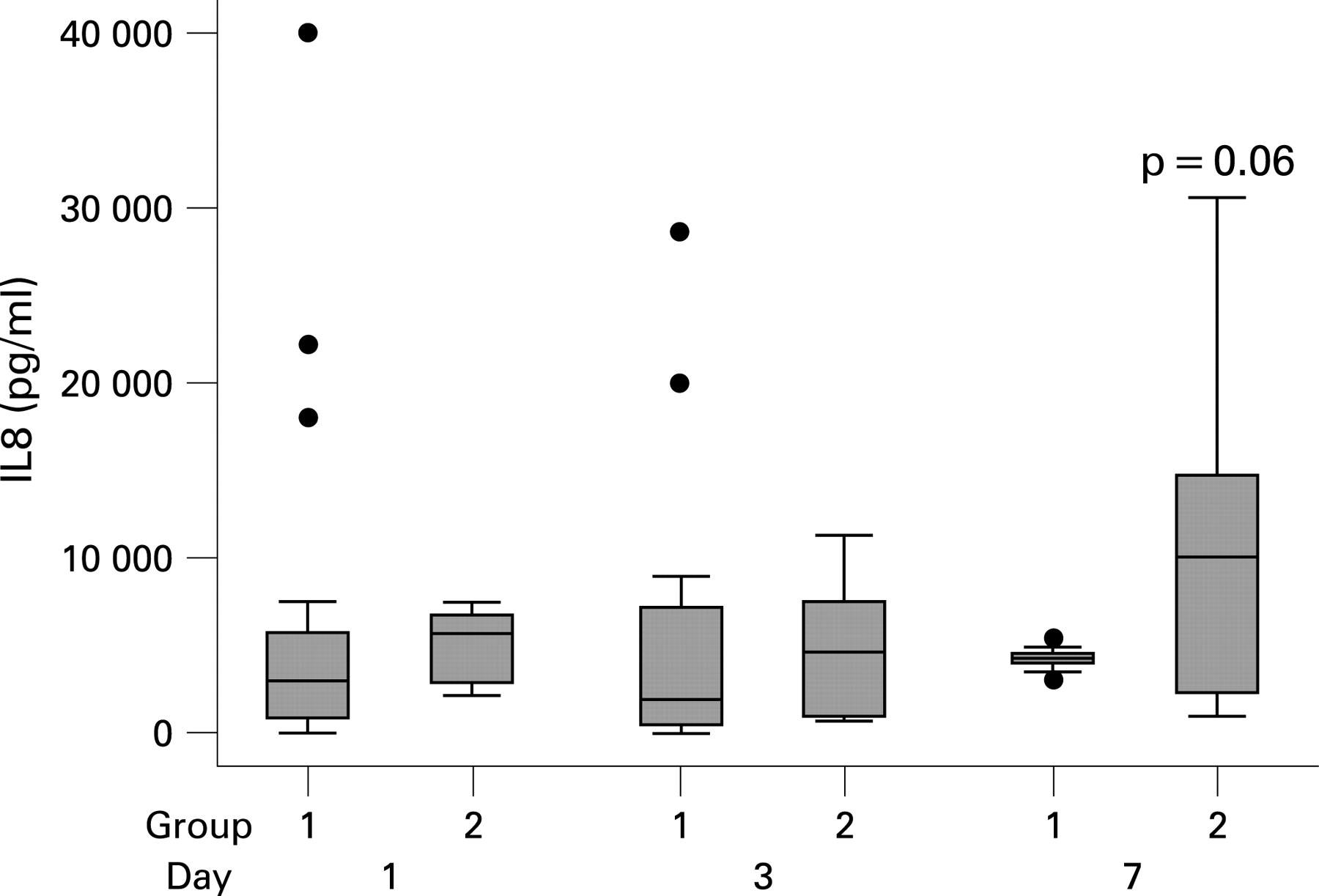
Samples of tracheal aspirate (TA) were collected on the first day of life (before the surfactant treatment and before placing the infants on the assigned ventilator), and on days 3 and 7 of life. After introducing 2 ml of saline solution into the trachea using a suction catheter, the patients were reconnected to the ventilator for 10–15 seconds with the same parameters. Samples of TA were then collected with the tip of catheter at the end of the tracheal tube.20 The procedure was always well tolerated and was performed as previously described.15 Serial TAs were collected on days 1, 3 and 7 while the infants remained intubated, to evaluate interleukin (IL) 6, IL8 and tumour necrosis factor α (TNFα) levels. We chose IL6 (early peak) as it is an early marker of inflammation, IL8 as it is the most important chemotactic factor of the lung; TNFα (later peak) as it seems to have a role in maintaining chronic inflammation in BPD.21
Ethics committee approval and parental consent before randomisation were obtained.
Data acquisition and analysis
We calculated a sample size of at least 12 neonates in each group to detect a difference of 50% in TA fluid IL6, IL8, TNFα in the VG 5.0 vs HFOV group at 7 days of life, with 80% power at 0.05 level.
Data within each group were compared by analysis of variance (Bonferroni post hoc test). The Mann–Whitney U test was performed for cytokine comparisons, categorical outcomes and for analysis of duration of oxygen dependency. Significance was set at p<0.05. Neither staff nor investigators were blinded. All cytokines samples were analysed in duplicate by the laboratory staff, unaware of the ventilatory strategies and the results were communicated to the investigators at the end of the analysis.
RESULTS
Forty infants were studied: 19 patients were randomised to A/C+VG and 21 patients to HFOV at 1 hour of life; clinical characteristics, respiratory and ventilatory status of infants in the two groups were similar (table 1). Fio2, adjusted to maintain Sato2 at 90–94%, did not differ between groups. Cytokine levels in the TA samples in the VG group showed a stable profile in the first week of life. IL6 levels in the TA samples in the HFOV group were significantly higher on day 3 (p<0.05) and day 7 (p = 0.03); moreover in the HFOV group, IL6, IL8 and TNFα levels were higher, but not significantly so, on day 7 (median values, Mann–Whitney U test, p = 0.09) (figs 1, 2 and 3).


{kind=link}
{kind=link}
{kind=link}
Ventilatory strategy according to randomisation (HFOV or A/C plus VG) was maintained until the 96th hour (table 2), when neonates in the HFOV group started to meet criteria for switching to A/C, according to protocols in our unit. On day 7 no infants assigned at birth to the HFOV group was still receiving HFOV, but they were spontaneously breathing (n = 6) or in A/C ventilation (n = 13). Of the infants assigned at birth to A/C ventilation, 14 were still receiving ventilation on day 7, while seven were extubated. No significant differences were seen in the duration of mechanical ventilation, in the need for surfactant administration, incidence of periventricular leucomalacia, IVH, retinopathy of prematurity or BPD between the two groups (table 3). The mortality rate was the same in both groups: one patient in each group died owing to late-onset sepsis. We observed a significantly longer oxygen dependency (p<0.05) in the HFOV group. No steroids were given in the first week of life. All infants, in both groups who developed BPD had high IL8 (>20 ng/ml) and TNFα (>0.35 ng/ml) levels on day 7. All extubations were successfully performed, with no need for reintubation.
What is already known on this topic
Bronchopulmonary dysplasia which remains common, may be mediated by proinflammatory cytokines.
Modes of ventilation may differ in relation to cytokine release in the lung.
DISCUSSION
Preterm infants are at risk of developing lung injury induced by inflammation. Barovolutrauma, oxygen, pulmonary infections and PDA are the main factors predisposing to lung inflammation and to BPD.22–24 Antenatal steroid treatment and postnatal surfactant therapy help in preventing BPD, but they need to be associated with protective ventilatory strategies in order to minimise lung damage.25–27 Repeated alveolar collapse and re-expansion and/or the administration of large Vt may lead to shear stress forces with alveolar damage and worsening of chronic lung injury. HFOV optimises lung recruitment, by using a stable, small Vt and maintaining a constant alveolar distending pressure. Although many authors speculated about the most effective and gentle ventilatory approach to the premature lung, uncertainty remains as to whether HFOV presents advantages over conventional ventilation. Marlow et al recently concluded that the initial mode of ventilation has no impact on early and late respiratory and neurological outcomes.28
What this study adds
An increased cytokine response was associated with a longer O2 dependency in babies given high-frequency oscillatory ventilation.
Volume-guarantee ventilation may offer advantages over high-frequency oscillatory ventilation, at least on the Dräger ventilator.
Conventional ventilation is still often considered as a whole, but it really is a multifaceted entity, in which synchronisation and mode of ventilatory support differ widely. Animal studies demonstrated that PTV, in combination with an “open lung” approach during recruitment manoeuvre, has the same level of gas exchange, protein infiltration and lung mechanics as HFOV.29 Human data are still lacking on this point. A/C ventilation plus VG with a Vt of 5 ml/kg and the application of an adequate PEEP (5 cm H2O), combined with a recruitment manoeuvre at birth, optimises lung filling, avoiding volutrauma with minimal haemodynamic interference and reducing work of breathing.30 A recent comparison of conventional ventilation and HFOV in preterm infants with RDS showed an association of early HFOV with lower lung inflammation and a shorter need for ventilation.16 Limitations of the study of Dani et al, and possible causes of results contrasting with ours, may be recognisable in the choice of pressure support ventilation (an effective strategy in the weaning phase) as a term of comparison with HFOV, the use of a different oscillator device (Sensormedics 3100A), the application of a low PEEP and the declared possibility for doctors to change the Vt during the study in the pressure support ventilation + VG group.
In our study we compared the effects of HFOV and A/C plus VG on lung inflammatory response in the early treatment of acute RDS, following a similar alveolar recruitment at birth. In the VG group we observed a stable profile of all cytokines levels in the first week of life; IL6 levels in the HFOV group were significantly higher on days 3 and 7 (p<0.05). The early increased cytokine response was associated with a longer O2 dependency in the HFOV group, as would be expected of a marker of lung injury. We believe that VG ventilation offers easily recognisable signals of the improvement of lung mechanics (eg, progressive reduction of PIP to reach the set Vt, increasing of spontaneous efforts, etc). This provides the clinicians with adequate information about the respiratory status, reducing the need for repeated chest x-rays or blood gases and can help to modulate ventilation. With HFOV, the improvements in lung mechanics are not so clearly identified and the hyperinflation point may be rapidly exceeded, following sudden improvements in compliance, with subsequent lung damage. At present, the choice of ventilatory strategy mainly depends on the experience of the different neonatal intensive care teams, rather than the clinical characteristics of the preterm infants. Our study confirms the hypothesis that PTV, in particular A/C, with a small Vt (Vt = 5 ml/kg) plus an adequate PEEP (5 cm H2O) is an effective and safe lung-protective strategy in the acute phase of RDS, inducing lower early lung inflammation than HFOV. Shorter need for O2 administration in the A/C plus VG group is a powerful positive respiratory outcome.
Limitations to this study include the relatively small number of patients, and wider studies are needed to confirm our conclusions. Moreover, our results apply to the HFOV option of the Dräger ventilator, about which limited data exist in the literature, and may not be generalisable to all high-frequency ventilators. HFOV may be provided by a variety of devices with well-documented and substantial differences in their performance, making it impossible to compare studies that do not use the same oscillators. However, the Dräger Babylog 8000, the Sensormedics 3100A and the SLE 2000HFO used in the UK Oscillation study11 have been shown to have similar performance at the frequencies recommended in our study.31 Early crossover from HFOV to AC+VG ventilation is an important study design flaw and may lead to confounding results: we followed our usual ventilation protocols but we cannot exclude the possibility that ventilatory switching interfered with the inflammatory reaction in the latter part of measurements. We will need to recalculate power analysis in the future, considering both the variability of data and reduction of the sample owing to extubation or switching ventilation in time. Postnatal steroid treatment was uncommon and similar in the groups, it always occurred after the first week of life and its influence on outcomes is balanced between groups.
REFERENCES
Footnotes
Competing interests: None.
Ethics approval: Approval from the ethics committee of Azienda ICP, Milan, Italy was obtained.
Linked Articles
- Fantoms