
Abstract
Objective
To evaluate the effect of extracorporeal gas exchange (ECMO) on mortality of patients referred with severe acute respiratory distress syndrome (ARDS).
Design and setting
Prospective observational study in a university hospital ICU.
Patients
150 patients with severe ARDS.
Interventions
Multimodal treatment with and without ECMO.
Measurements and main results
We treated 118 patients (78.7%) conservatively and 32 patients with ECMO. Patients in the ECMO group presented with significantly more severe disease (lung injury score 3.8 ± 0.3 vs. 3.3 ± 0.4; SOFA score 52 ± 14 vs. 43 ± 12; and SAPS score 14 ± 3.3 vs. 10 ± 3.5). Mortality in ECMO-treated patients tended to be higher than that with conservative treatment (46.9% vs. 28.8%, p = 0.059). Multivariate logistic regression analyses with backward selection excluded ECMO as predictor of mortality (p = 0.79). Independent predictors of mortality were age (odds ratio 1.044, 95% confidence interval 1.014–1.075, p = 0.004), mean pulmonary artery pressure (1.082, 1.026–1.141, p = 0.036), sequential organ failure assessment score (1.148, 1.018–1.294, p = 0.024), and days of mechanical ventilation prior to referral (1.064, 1.008–1.123, p = 0.025).
Conclusion
ECMO treatment does not predict mortality in patients with most severe ARDS.
Similar content being viewed by others
Introduction
Extracorporeal membrane oxygenation (ECMO) provides the theoretical advantage of dissociation of oxygenation and ventilation. The failing lungs are kept inflated and resting by the mechanical ventilator while ECMO eliminates CO2 and improves oxygenation. In theory, given a severe case of acute respiratory distress syndrome (ARDS), this should reduce both ventilator-induced lung injuries and the subsequent systemic inflammation and may improve the patient's outcome. Randomized controlled trials, however, have failed to demonstrate that ECMO improves outcome in ARDS [1, 2, 3]. Nevertheless, ECMO treatment is still widely performed, and the Extracorporeal Life Support Organisation counts 115 active members throughout the world (http://www.elso.med.umich.edu). ECMO thus divides ICU physicians into friends and foes as the role of the procedure during treatment of severe ARDS remains questionable.
As a tertiary ICU specialized in multimodal ARDS treatment including ECMO we prospectively studied the effect of ECMO treatment on mortality of patients with severe ARDS.
Methods
Patients and primary care
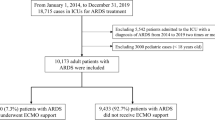
Between January 1998 and September 2003, 150 consecutive patients diagnosed with ARDS and referred from external hospitals to our ICU were assessed prospectively using a dedicated database. ARDS was defined as described elsewhere [4] and by Lung Injury Score (LIS) higher than 2.5 [5]. All patients had previously been mechanically ventilated in other ICUs and were enrolled if they fulfilled the ARDS criteria, were younger than 70 years, and weighed more than 15 kg. Exclusion criteria were: malignancy, end-stage lung disease, and intracranial bleeding.
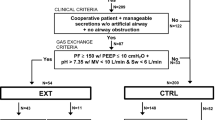
For patients' acquisition staff physicians were dispatched to the referring ICU to optimize the patient's condition prior to transport with ambulance or helicopter. Patients unresponsive to conservative measures (arterial oxygen saturation > 90% after positive end-expiratory pressure, PEEP, adjustment and prone position trial) were placed on ECMO and transported on extracorporeal bypass. Standardized ventilatory protocol consisted tidal volume of 6–8 ml/kg, respiratory rate (RR) of 20 bpm, and inspiratory to expiratory ratio of 1 using a mobile intensive care ventilator (Evita 2 dura, Dräger Medical, Lübeck, Germany). In the case of respiratory acidosis (pHa < 7.2) RR was increased up to 30 bpm avoiding air trapping. The patients were sedated with fentanyl and midazolam and were paralyzed for transport only. No patient was rejected as unstable for transport. If hypoxemia (SaO2 < 90%) persisted despite optimum PEEP we added inhaled nitric oxide (2–40 ppm; Pulmonox mini, Tyco Healthcare, Hennef, Germany). Dependency on inhaled nitric oxide was tested by daily interruption and discontinued if it was possible without iNO to achieve FIO2 of 0.4 or less and pulmonary artery pressure (PAP) below 35 mmHg. In persistent hypoxemia and/or decompensated severe acidosis (pH < 7.1) venovenous ECMO was initiated.
Management of venovenous extracorporeal gas exchange
For ECMO two large-bore cannulae were inserted percutaneously into the superior (19 F) and inferior (23 F) caval veins via the jugular and femoral veins for blood return and drainage, respectively (BioMedicus Cannula, Medtronic, Düsseldorf, Germany). A heparin bonded ECMO circuit (Super Tygon, Medtronic) was used with two silicon membrane oxygenators (Medtronic, I3500-2A). A bypass (CAPS, Stöckert Instrumente, Munich, Germany) flow of 30–50% of the patient's cardiac output was applied with oxygen sweep flow averaging 8 l/min. ECMO discontinuation criteria were: PaO2/FIO2 ratio higher than 200 torr at a mean airway pressure less than 25 cmH2O and pHa greater than 7.2.
Measurements
The main outcome measure was hospital mortality. All cardiopulmonary variables were recorded after admission to our ICU along with the first laboratory findings, and catecholamine dose. All pressures were recorded at end-expiration at adjusted PEEP. The Simplified Acute Physiology Score (SAPS) II [6] and Sepsis-Related Organ Failure Assessment (SOFA) score [7] were calculated from the lowest values within the first 24 h after admission.
Statistical analysis
All metric data are presented as means (± standard deviation). We tested the main hypothesis that ECMO treatment would increase patients' in-hospital mortality. Furthermore, we compared variables of respiratory and pulmonary function that were recorded on the day of admission between patients treated conservatively and those undergoing ECMO. SAS 8.2 software (SAS Institute, Cary, N.C., USA) was used for statistical analysis. The Wilcoxon rank-sum test was used for testing continuous variables, Fisher's exact test for dichotomous variables, and the χ2 test for ordinal variables. A p value less than 5% was considered significant; the α error (significance level) was fixed at 5%. With exploratory intention we also compared the effect of ECMO therapy on mortality in the subgroup that were most frequently treated with ECMO in our institution, i.e., patients with community-acquired pneumonia (CAP). We entered the variables of age, PaO2/FIO2 ratio, duration on mechanical ventilation prior to admission, SOFA score, mean PAP, and ECMO treatment in multivariate logistic regression analyses with backward selection to identify independent predictors of outcome. Additionally, we performed survival analysis with backward selection to confirm results of the multivariate logistic regression.
Results
The mean survival rate of patients with severe ARDS was 67%. Of the 150 patients 32 were treated with ECMO (21.3%). The severity of the disease was significantly higher in ECMO treated patients (Table 1) than in those without ECMO treatment, particularly on LIS (3.8 ± 0.3 vs. 3.3 ± 0.4, p < 0.0001), SOFA score (14 ± 3.3 vs. 10 ± 3.5, p < 0.0001), and plasma lactate concentration (6.9 ± 3.7 vs. 3.6 ± 3.1 mg/dl, p < 0.0001). Mortality in ECMO-treated patients was not significantly higher than in those receiving conservative treatment (46.9 vs. 28.8%, p = 0.059). Multivariate logistic regression revealed the following independent predictors of death: age (odds ratio, OR, 1.044, 95% confidence interval, CI, 1.014–1.075, p = 0.0041), mean PAP (OR 1.082, CI 1.026–1.141, p = 0.036), SOFA (OR 1.148, CI 1.018–1.294, p = 0.024), and days of mechanical ventilation prior to referral (OR 1.064, CI 1.008–1.123, p = 0.025) but not ECMO treatment (p = 0.79) or PaO2/FiO2 ratio (p = 0.17). Survival analysis affirmed age (p = 0.01) and PAP (p = 0.004) as independent predictors of survival. Main causes of death were septic multiorgan failure (n = 25, 51%) and right ventricular failure (n = 13, 26.5%). Sepsis (n = 51; 34%), CAP (n = 47, 31.3%), hospital-acquired pneumonia (n = 24, 16%), aspiration (n = 15, 10%), and trauma (n = 13, 8.7%) were the causes of ARDS.
ECMO was performed most frequently in patients with CAP (53.1% of ECMO treatments; Table 2). In cases of CAP the mortality among patients treated with ECMO was similar to that in those treated conservatively (29.4 vs. 23.3%, p = 0.73); age (OR 1.072, CI 1.003–1.145, p = 0.039) was the only independent predictor of death in this subgroup of patients with ARDS.
Discussion
ECMO treatment was not a predictor of mortality. In patients with severe ARDS even though ECMO patients had significantly more severe disease than those treated conservatively. Age, PAP, SOFA score, and duration of mechanical ventilation (Table 3) before initiation of a multimodal treatment independently predicted mortality in multivariate logistic regression. While age [8, 9, 10] and SOFA score [6, 11, 12] are general predictors of mortality in critical illness, prolonged mechanical ventilation and pulmonary hypertension are more ARDS-specific risk factors. Prolonged mechanical ventilation prior to ECMO treatment has been shown by others to affect outcome [13, 14]. In our patients with severe ARDS right ventricular failure was the second leading cause of death, and pulmonary hypertension proved to be an independent predictor of survival. These data support the findings of earlier studies reporting pulmonary hypertension in ARDS [15, 16, 17].
Our therapeutic regimen for treating severe ARDS focused upon avoiding ECMO because this treatment is associated with increased transfusion requirement and life-threatening complications [18], theoretically increasing mortality. However, in our study ECMO treatment was not significantly associated with increased mortality despite the fact that the severity of the disease (LIS, SOFA, and plasma lactate concentration) among these patients was significantly higher than that in patients who were treated conservatively. Further studies with an even greater number of patients are needed to clarify whether the trend towards higher mortality in the ECMO group, as observed in our study, was a random observation or a significant finding.
Our therapeutic strategy prevented ECMO in nearly 80% of patients with severe ARDS referred for ECMO therapy. ECMO was most frequently implemented in patients with severe CAP-induced ARDS. Patients with severe CAP showed a rapid progression to ARDS and (septic) shock refractory to standard ICU care and mechanical ventilation in the referring ICUs, such that ECMO was implemented earlier after onset of the disease. Mortality in patients with CAP treated with ECMO did not differ from that in patients treated conservatively.
The main limitation of our study is the lack of randomization. Therefore we are not able to drawing final conclusions about the impact of any single treatment modality. Randomized controlled trials that implement disease entity-based subgrouping are useful to evaluate the effectiveness of ECMO treatment in well-defined patient populations.
References
Zapol WM, Snider MT, Hill JD, Fallat RJ, Bartlett RH, Edmunds LH, Morris AH, Peirce EC 2nd, Thomas AN, Proctor HJ, Drinker PA, Pratt PC, Bagniewski A, Miller RG Jr (1979) Extracorporeal membrane oxygenation in severe acute respiratory failure. A randomized prospective study. JAMA 242:2193–2196
Gattinoni L, Pesenti A, Mascheroni D, Marcolin R, Fumagalli R, Rossi F, Iapichino G, Romagnoli G, Uziel L, Agostoni A (1986) Low-frequency positive-pressure ventilation with extracorporeal CO2 removal in severe acute respiratory failure. JAMA 256:881–886
Morris AH, Wallace CJ, Menlove RL, Clemmer TP, Orme JFJ, Weaver LK, Dean NC, Thomas F, East TD, Pace NL (1994) Randomized clinical trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med 149:295–305
Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, Lamy M, Legall JR, Morris A, Spragg R (1994) The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 149:818–824
Murray JF, Matthay MA, Luce JM, Flick MR (1988) An expanded definition of the adult respiratory distress syndrome. Am Rev Respir Dis 138:720–723
Le Gall JR, Lemeshow S, Saulnier F (1993) A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 270:2957–2963
Vincent JL, Moreno R, Takala J, Willats S, De Mendonca A, Bruining H, Reinhart CK, Suter PM, Thijs LG (1996) The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure. Intensive Care Med 22:707–710
Brun-Buisson C, Cosetta M, Bertollini G, Brazzi L, Pimentel J, Lewandowski K, Bion J, Romand JA, Villar J, Thorsteinsson A, Damas P, Armaganidis A, Lemaire F, for the ALIVE Study Group (2004) Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med 30:51–61
Squara P, Dhainaut JFA, Artigas A, Carlet J, and the European Collaborative ARDS Working Group (1998) Hemodynamic profile in severe ARDS: results of the European Collaborative ARDS Study. Intensive Care Med 24:1018–1028
Martin GS, Mannino DM, Moss M (2006) The effect of age on the development and outcome of adult sepsis. Crit Care Med 34:15–21
Moreno R, Vincent JL, Matos R, Mendonca A, Cantraine F, Thijs L, Takala J, Sprung C, Antonelli M, Bruining H, Willats S, on behalf of the working group on sepsisrelated problems of the ESICM (1999) The use of the maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Intensive Care Med 25:686–695
Bota DP, Melot C, Ferreira FL, Ba VN, Vincent JL (2002) The multiple organ dysfunction score (MODS) versus the sequential organ failure assessment (SOFA) score in outcome prediction. Intensive Care Med 28:1619–1624
Hemmila MR, Rowe SA, Boules TN, Miskulin J, McGillicuddy JW, Schuerer DJ, Haft JW, Swaniker F, Arbabi S, Hirschl RB, Bartlett RH (2004) Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann Surg 240:595–607
Pranikoff T, Hirschl RB, Steimle CN, Anderson HL, Bartlett RH (1997) Mortality is directly related to the duration of mechanical ventilation before the initiation of extracorporeal life support for severe respiratory failure. Crit Care Med 25:28–32
Villar J, Blazquez MA, Lubillo S, Quintana J, Manzano JL (1989) Pulmonary hypertension in acute respiratory failure. Crit Care Med 17:523–526
Squara P, Dhainaut JFA, Artigas A, Carlet J,and the European Collaborative ARDS Working Group (1998) Hemodynamic profile in severe ARDS: results of the European Collaborative ARDS Study. Intensive Care Med 24:1018–1028
Beiderlinden M, Kuehl H, Boes T, Peters J (2006) Prevalence of pulmonary hypertension associated with severe acute respiratory distress syndrome: predictive value of computed tomography. Intensive Care Med 32:852–857
Hemmila MR, Rowe SA, Boules TN, Miskulin J, McGillicuddy JW, Schuerer DJ, Haft JW, Swaniker F, Arbabi S, Hirschl RB, Bartlett RH (2004) Extracorporeal life support for severe acute respiratory distress syndrome in adults. Ann Surg 240:595–607
Acknowledgements
We thank the nursing staff of our ICU for their dedicated support. Furthermore, we thank all physicians for referral of their patients and the confidence in our work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beiderlinden, M., Eikermann, M., Boes, T. et al. Treatment of severe acute respiratory distress syndrome: role of extracorporeal gas exchange. Intensive Care Med 32, 1627–1631 (2006). https://doi.org/10.1007/s00134-006-0262-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0262-y