





Figures
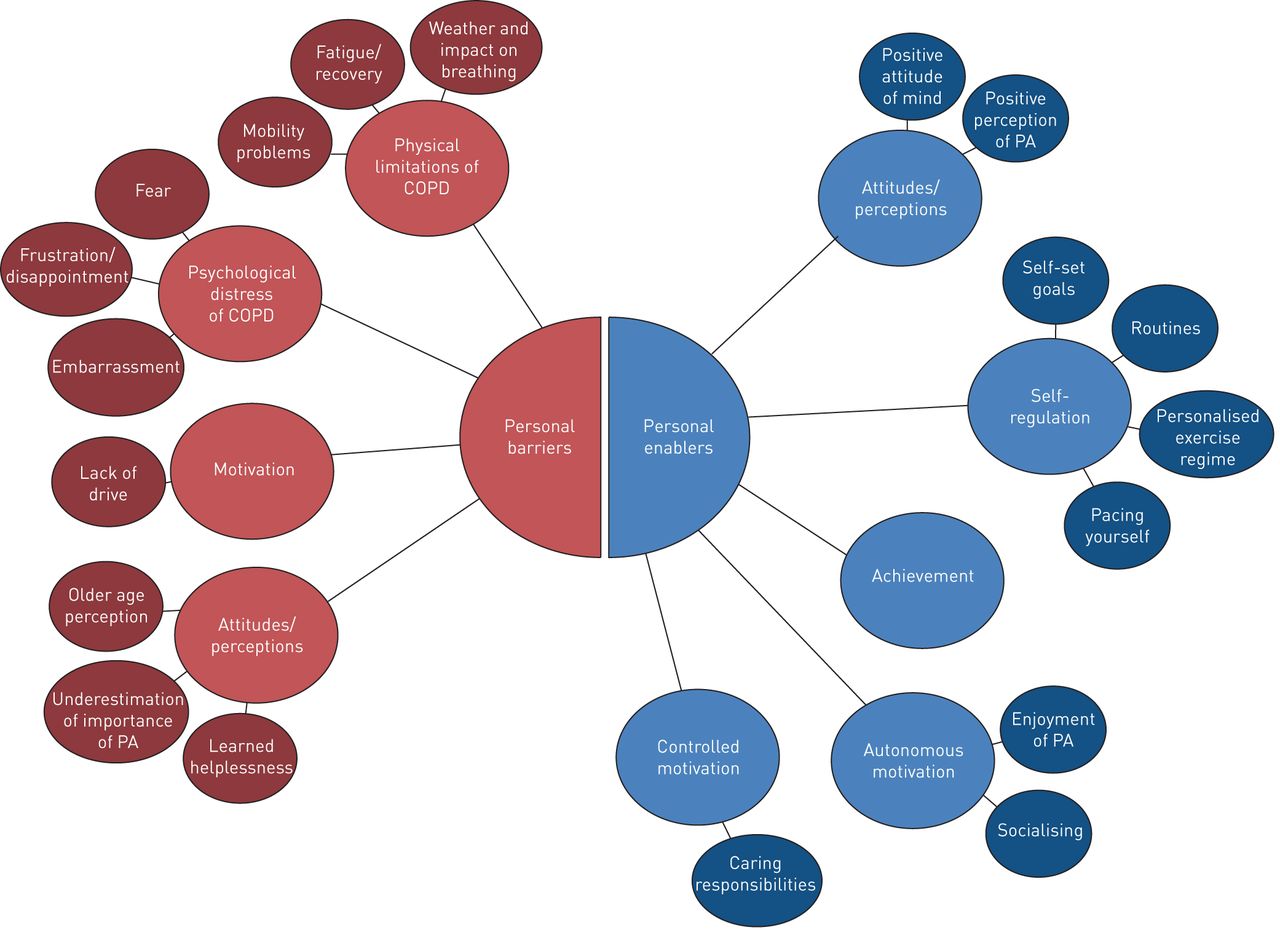
- FIGURE 1
Examples of personal barriers and enablers that both encourage and limit participation in physical activity for patients with chronic obstructive pulmonary disease (COPD). PA: physical activity. Reproduced from [53] with permission.
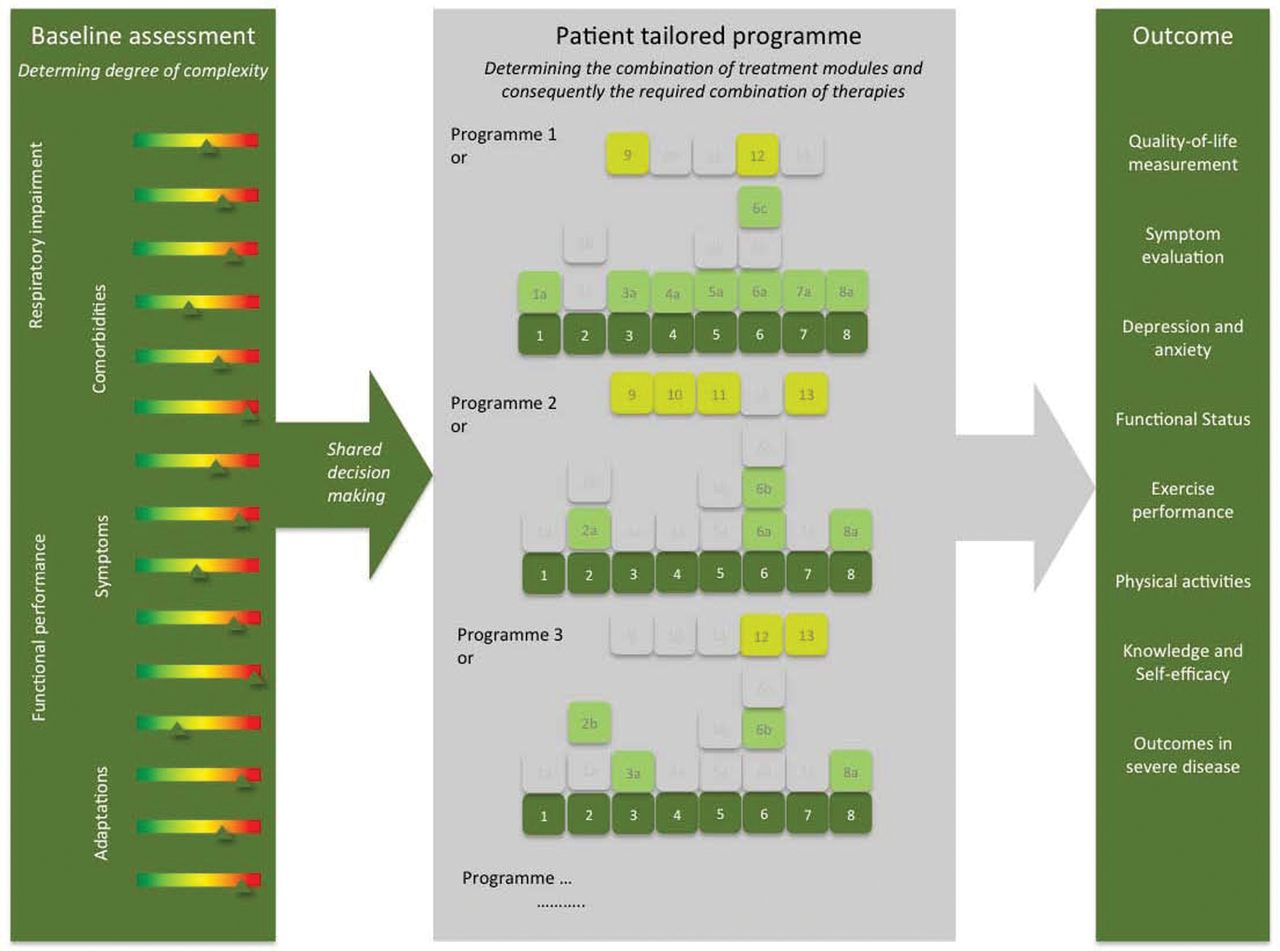
- FIGURE 2
The process of a patient-tailored programme including the three core processes (baseline assessment, tailored treatment and outcome assessment). An integrated baseline assessment identifying the complexity of the disease is followed by a treatment programme composed of at least all basic modules. Depending on the complexity, specific burden-driven modules can be added. Each individualised programme is followed by an outcome measurement. Examples of adaptations include degree of self-management and coping. Reproduced from [21] with permission.


{kind=link}
{kind=link}
Tables
- TABLE 1
Overview of strategies to classify, assess or group patients with chronic obstructive pulmonary disease (COPD)
Goal Advantages Shortcomings Heterogeneity Complexity GOLD Classification of COPD based on the degree of airflow obstruction (up to 2011), in combination with symptoms/exacerbations (2011–2017), or symptoms/exacerbations only (2017) From an FEV1 centric view to a more extensive approach and a more prominent role of symptoms/individual measures [13] Parameters assessing COPD severity still very limited; ignoring variability and unpredictability of symptoms/exacerbations/hospitalisations; proposed cut-off points for symptom measures mostly expert driven Separation of airflow limitation
from clinical parameters (GOLD 2017) [9] clarifies what is being evaluated and ranked and might facilitate more precise treatmentNot addressed Multidimensional indices Prognostic indices to predict survival; screening instruments As prognostic markers: useful in grouping patients in terms of clinically relevant outcomes [14]; as a screening instrument: multidimensional assessment of COPD [11, 15] Identification of substitute groups or phenotypes only by selected variables included in the respective index; consist of a limited number of variables; have not been developed to guide future treatment [16] Multidimensional assessment, including, for example, medical, pathophysiological, symptomatic [14] and/or psychological [15] parameters Not addressed Phenotypes Grouping patients based on certain characteristics From “blue bloater” and “pink puffer” to complex cluster analyses identifying existing and novel phenotypes Cluster analyses only moderate reproducibility, clinical application disputable [17], considerable overlap between phenotypes for some specific attributes As a screening instrument: differentiating between individuals by assessing/clustering various characteristics Not addressed COPD control panel Assessment of different elements of the disease Assessing at least three dimensions (severity, activity and impact), can be customised to the need of the patient [18] Unclear which characteristics should exactly be assessed, which methods, cut-off points, etc. should be used Multidimensional assessment; might serve as a “clinical decision support system” (by selecting/classifying patients) Not addressed Treatable traits Label-free, precision medicine approach COPD management based on individual treatable characteristics (intra- and extrapulmonary treatable traits, treatable behaviour/lifestyles (including patients’ environment)) [19] Separate assessment of treatable traits results in fragmented treatment; frequency of assessment and inter-relationships between traits unknown Assessing heterogeneity by individual unique traits Not addressed Pulmonary rehabilitation Personalised, holistic approach of treatable traits Comprehensive intervention based on a thorough assessment taking into account the combination and interaction between the (treatment of) individual treatable traits [20] Applicability in routine clinical practice (dependent on organisational structure, facilities, workforce, funding, etc.) is challenging; poor referral and compliance; not all traits are always addressed (yet); mostly non-pharmacological generic interventions Assessing heterogeneity by individual unique traits Assessment of complex interactions of physical, psychological, social and environmental factors by dedicated, transdisciplinary teams being able to respond flexibly as well as accept unpredictability and non-linear outcomes [21] GOLD: Global initiative for chronic Obstructive Lung Disease; FEV1: forced expiratory volume in 1 s.










