





Abstract
Bullectomy, lung volume reduction surgery and transplantation can palliate dyspnoea in emphysema. The available data suggest that their mode of action, at least with regard to pulmonary mechanics, includes beneficial effects on dynamic hyperinflation. In single lung transplant recipients, this may be asymmetric, causing native lung hyperinflation.
Considerable data exists to show that, despite maximal medical therapy, advanced emphysema causes disabling breathlessness. Prior to the renaissance of lung volume reduction surgery (LVRS), except for occasional patients who could benefit from a bullectomy [1, 2] or a Monaldi procedure [3], the only surgical therapy available was single lung transplantation (SLT) or double lung transplantation (DLT).
SLT or DLT for emphysema can be effective for the palliation of breathlessness in emphysema, though it probably does not greatly increase lifespan. However, typically the operation has a 1-yr mortality approaching 15% and donor organs are usually in short supply. Indeed, as there have always been more potential recipients than donors, the technique of lung volume reduction, originally conceived of in 1959 [4], was revived in 1996 by Cooper et al. [5]. The approximate present status of LVRS is that forced expiratory volume in one second (FEV1) is increased in 75% of patients against a perioperative mortality, which is typically 4–5% [6–9]. Benefits may be expected to last ∼3–5 yrs in the best responders [10, 11] but ∼25% of patients do not derive measurable benefit.
Clearly, the magnitude of benefit varies between LVRS, SLT and DLT. Of course, no study has compared these interventions prospectively and few have directly measured dynamic hyperinflation (DH). Nevertheless, some feel for the benefits of these therapies may be gained from table 1⇓.
Representative data for different surgical therapies in emphysema
EFFECT OF SPECIFIC THERAPIES ON RESTING AND DH
Bullectomy
O'Donnell et al. [2] followed eight patients who had undergone bullectomy, four of whom also had partial lung resection. Improvement in resting lung volumes was observed (table 1⇑) and DH (i.e. exercise-induced) was also measured using the inspiratory capacity technique, utilising the widely held assumption that total lung capacity does not change. Significant improvements were observed in end-expiratory lung volume (EELV; fig. 1⇓). Relief of exertional breathlessness, measured as change in Borg score during exercise, correlated best with change in EELV.

Dynamic lung volumes before (•) and after (○) bullectomy in eight subjects during an incremental exercise test. Area marked by dotted lines indicates the predicated values for normal subjects. % pred: % predicted; TLC: total lung capacity; VT: tidal volume. Reproduced and modified from [2] with permission from the publisher.
LVRS
Wisser et al. [12] reported uncontrolled data on 54 patients undergoing bilateral LVRS. Static lung volumes were reduced by surgery. Dynamic lung volumes were not reported but, interestingly, a significant fall in intrinsic positive end-expiratory oesophageal pressure (PEEPi) was observed, suggesting reduced flow limitation and intuitively less DH. This observation was also reported by Tschernko et al. [13] at rest and during exercise. However, both these studies used the Bicore device, which does not monitor gastric pressure trace, thereby making it difficult to determine how much of the observed PEEP is due to PEEPi and how much is due to abdominal muscle recruitment (for further discussion on this point see [14, 15]). Shade et al. [16] presented uncontrolled data on 33 patients undergoing bilateral LVRS; although an increase in exercise endurance was observed, dynamic lung volumes were not reported. Similar data were reported by Stammberger et al. [17] and Leyenson et al. [18].
In the National Emphysema Treatment Trial, significant improvements in walking distance were more likely in patients randomised to the surgical arm, but no data is provided on operating lung volumes during exercise or indeed on static lung volumes [7].
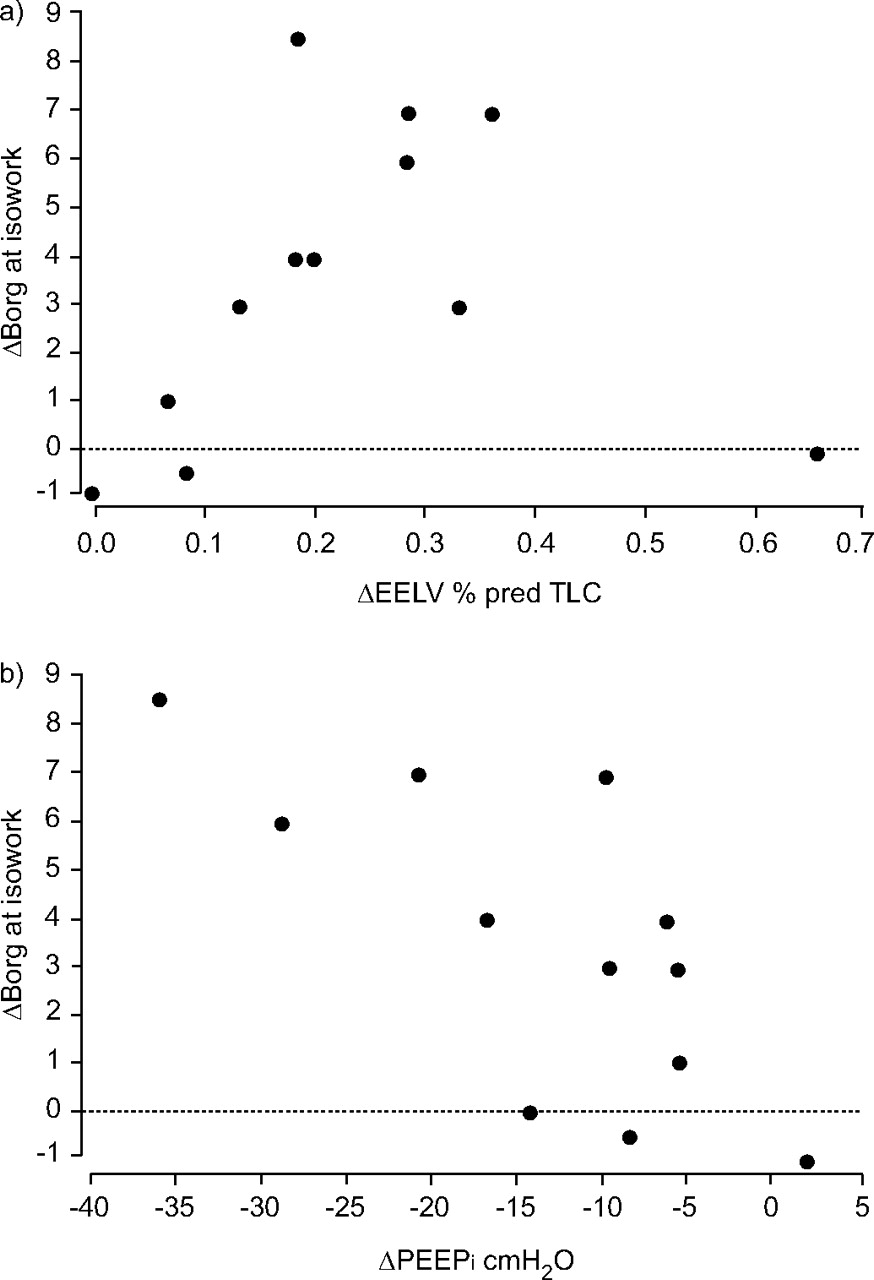
To the best of the present author’s knowledge, only one study has sought to measure DH directly in patients undergoing LVRS [19]. Martinez et al. [19] studied 17 patients before and after bilateral LVRS; DH was measured in a subgroup of 12 using the inspiratory capacity technique. A reduction in both EELV and end-inspiratory lung volume was observed after surgery, typically by ∼1 L. As shown in figure 2⇓, relief of breathlessness was strongly associated with reduced DH. Reduction in DH was not clearly related to improvement in FEV1, mirroring subsequent observations from pharmacological studies [20].

The change in Borg score at isowork in 12 patients during an incremental exercise protocol is shown on the vertical axis. Reduced breathlessness is strongly related to a) reduced dynamic hyperinflation and to its indirect relation, b) reduced intrinsic positive end-expiratory pressure (PEEPi). ΔEELV: change in end-expiratory lung volume; % pred: % predicted; TLC: total lung capacity. Reproduced from [19] with permission from the publisher.
Lung transplantation
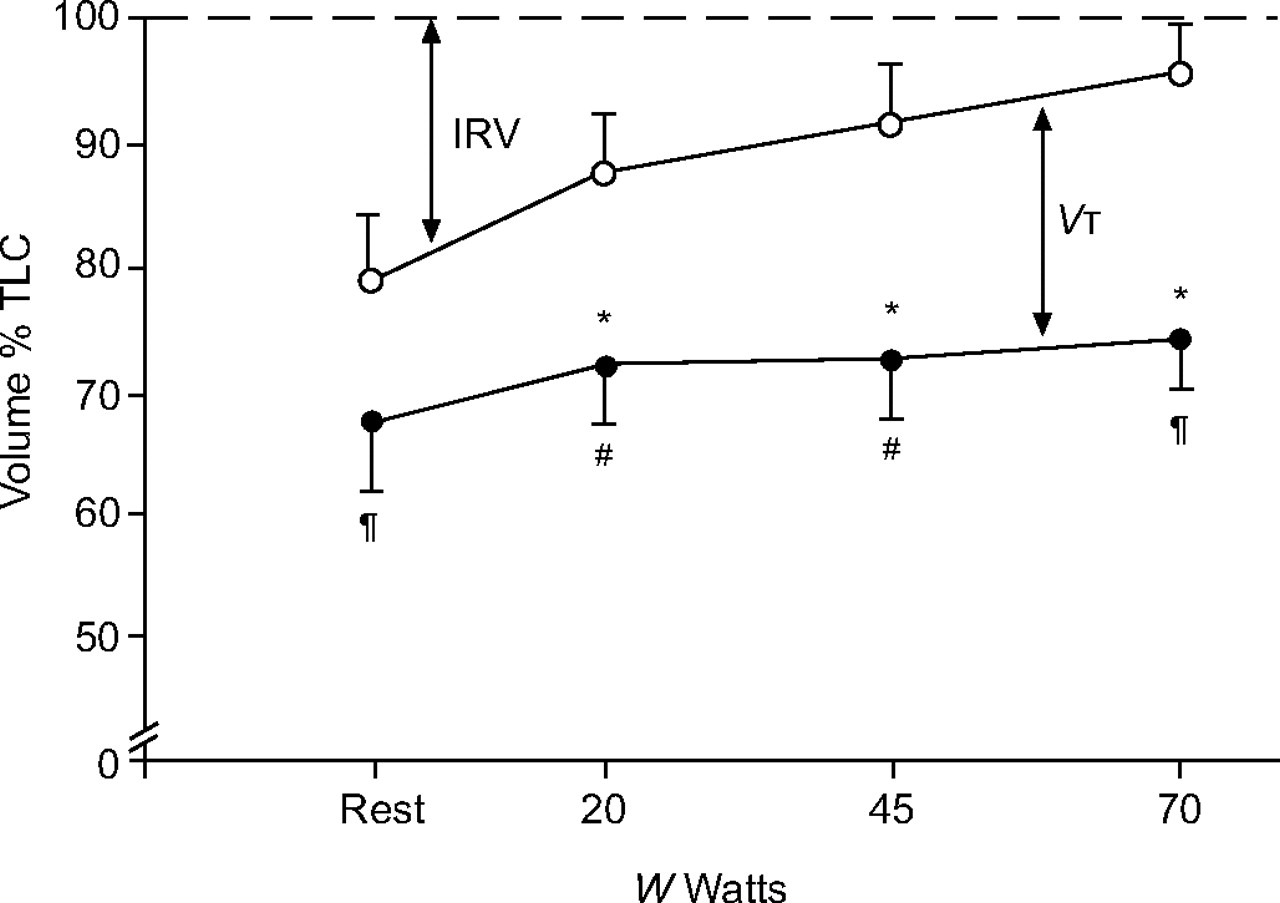
Martinez et al. [21] also studied SLT and DLT recipients using the inspiratory capacity technique. Clearly it was not possible to obtain data from patients prior to surgery but those authors found that most DLT patients could reach their peak exercise without increasing EELV; mean EELV at peak exercise was 100 mL less than resting. In contrast, eight out of eight SLT recipients increased EELV during exercise by a mean of 370 mL (fig. 3⇓). This observation was repeated in SLT recipients by Murciano et al. [22]. If it is clear that SLT patients usually develop DH whilst DLT patients frequently do not, it seems likely that SLT patients could develop native lung hyperinflation during exercise (and conversely that the transplanted lung does not). This has not, to the best of the present author’s knowledge, been identified during exercise but it has been identified at rest, and LVRS to the native lung may be of benefit in this situation [23].
{kind=link}
{kind=link}
{kind=link}
Progression of operating lung volumes during incremental exercise in emphysema patients who have undergone single lung transplantation. ○: end-inspiratory lung volume; •: end-expiratory lung volume. IRV: inspiratory reserve volume; VT: tidal volume; TLC: total lung capacity; W: external power. #: n = 8; ¶: n = 7. *: p<0.05. Reproduced and modified from [22] with permission from the publisher.
CONCLUSION
Although physiological data are sparser than desired, various surgical interventions can palliate dyspnoea and probably do so in part by reducing hyperinflation. Understanding the mechanisms underlying dynamic hyperinflation, particularly with regard to collateral ventilation, may allow better selection of patients for surgery.
- © ERSJ Ltd
References









